
- Issue 4 Pages 137-
- Issue 3 Pages 101-
- Issue 2 Pages 57-
- Issue 1 Pages 1-
- Issue Supplement-1 Pa・・・
- Issue 12 Pages 535-
- Issue 11 Pages 495-
- Issue 10 Pages 437-
- Issue 9 Pages 381-
- Issue 8 Pages 327-
- Issue 7 Pages 265-
- Issue 6 Pages 221-
- Issue 5 Pages 173-
- Issue 4 Pages 131-
- Issue 3 Pages 91-
- Issue 2 Pages 43-
- Issue 1 Pages 1-
- Issue Supplement-3 Pa・・・
- Issue Supplement-2 Pa・・・
- Issue Supplement-1 Pa・・・
- Issue 12 Pages 535-
- Issue 11 Pages 489-
- Issue 10 Pages 445-
- Issue 9 Pages 391-
- Issue 8 Pages 347-
- Issue 7 Pages 307-
- Issue 6 Pages 261-
- Issue 5 Pages 215-
- Issue 4 Pages 165-
- Issue 3 Pages 111-
- Issue 2 Pages 57-
- Issue 1 Pages 1-
- Issue Supplement-3 Pa・・・
- Issue Supplement-2 Pa・・・
- Issue Supplement-1 Pa・・・
- Issue 12 Pages 675-
- Issue 11 Pages 619-
- Issue 10 Pages 563-
- Issue 9 Pages 505-
- Issue 8 Pages 453-
- Issue 7 Pages 393-
- Issue 6 Pages 347-
- Issue 5 Pages 297-
- Issue 4 Pages 245-
- Issue 3 Pages 163-
- Issue 2 Pages 63-
- Issue 1 Pages 1-
- Issue Supplement-3 Pa・・・
- Issue Supplement-2 Pa・・・
- Issue Supplement-1 Pa・・・
- Issue 12 Pages 565-
- Issue 11 Pages 521-
- Issue 10 Pages 483-
- Issue 9 Pages 419-
- Issue 8 Pages 375-
- Issue 7 Pages 319-
- Issue 6 Pages 277-
- Issue 5 Pages 231-
- Issue 4 Pages 165-
- Issue 3 Pages 109-
- Issue 2 Pages 55-
- Issue 1 Pages 1-
- Issue Supplement-3 Pa・・・
- Issue Supplement-2 Pa・・・
- Issue Supplement-1 Pa・・・
- Issue 12 Pages 449-
- Issue 11 Pages 399-
- Issue 10 Pages 361-
- Issue 9 Pages 331-
- Issue 8 Pages 293-
- Issue 7 Pages 247-
- Issue 6 Pages 197-
- Issue 5 Pages 163-
- Issue 4 Pages 117-
- Issue 3 Pages 69-
- Issue 2 Pages 41-
- Issue 1 Pages 1-
- Issue Special-Issue P・・・
- Issue Supplement-3 Pa・・・
- Issue Supplement-2 Pa・・・
- Issue Supplement-1 Pa・・・
- Issue 12 Pages 487-
- Issue 11 Pages 461-
- Issue 10 Pages 405-
- Issue 9 Pages 369-
- Issue 8 Pages 327-
- Issue 7 Pages 279-
- Issue 6 Pages 231-
- Issue 5 Pages 191-
- Issue 4 Pages 147-
- Issue 3 Pages 103-
- Issue 2 Pages 61-
- Issue 1 Pages 1-
- Issue Supplement-3 Pa・・・
- Issue Supplement-2 Pa・・・
- Issue Supplement-1 Pa・・・
- Issue 12 Pages 621-
- Issue 11 Pages 563-
- Issue 10 Pages 505-
- Issue 9 Pages 435-
- Issue 8 Pages 375-
- Issue 7 Pages 301-
- Issue 6 Pages 247-
- Issue 5 Pages 199-
- Issue 4 Pages 151-
- Issue 3 Pages 107-
- Issue 2 Pages 59-
- Issue 1 Pages 1-
- Issue Supplement-3 Pa・・・
- Issue Supplement-2 Pa・・・
- Issue Supplement-1 Pa・・・
- Issue 12 Pages 725-
- Issue 11 Pages 655-
- Issue 10 Pages 585-
- Issue 9 Pages 517-
- Issue 8 Pages 451-
- Issue 7 Pages 355-
- Issue 6 Pages 285-
- Issue 5 Pages 205-
- Issue 4 Pages 151-
- Issue 3 Pages 97-
- Issue 2 Pages 51-
- Issue 1 Pages 1-
- Issue Supplement-3 Pa・・・
- Issue Supplement-2 Pa・・・
- Issue Supplement-1 Pa・・・
- Issue 12 Pages 861-
- Issue 11 Pages 819-
- Issue 10 Pages 775-
- Issue 9 Pages 695-
- Issue 8 Pages 611-
- Issue 7 Pages 529-
- Issue 6 Pages 453-
- Issue 5 Pages 357-
- Issue 4 Pages 267-
- Issue 3 Pages 189-
- Issue 2 Pages 107-
- Issue 1 Pages 1-
- Issue Supplement-3 Pa・・・
- Issue Supplement-2 Pa・・・
- Issue Supplement-1 Pa・・・
- Issue 12 Pages 943-
- Issue 11 Pages 863-
- Issue 10 Pages 775-
- Issue 9 Pages 691-
- Issue 8 Pages 599-
- Issue 7 Pages 511-
- Issue 6 Pages 429-
- Issue 5 Pages 349-
- Issue 4 Pages 261-
- Issue 3 Pages 163-
- Issue 2 Pages 81-
- Issue 1 Pages 1-
- Issue Supplement-3 Pa・・・
- Issue Supplement-2 Pa・・・
- Issue Supplement Page・・・
- |<
- <
- 1
- >
- >|
-
Miki HASHIDA, Satoshi MAESAWA, Sachiko KATO, Daisuke NAKATSUBO, Takahi ...2024 Volume 64 Issue 4 Pages 137-146
Published: April 15, 2024
Released on J-STAGE: April 15, 2024
Advance online publication: February 15, 2024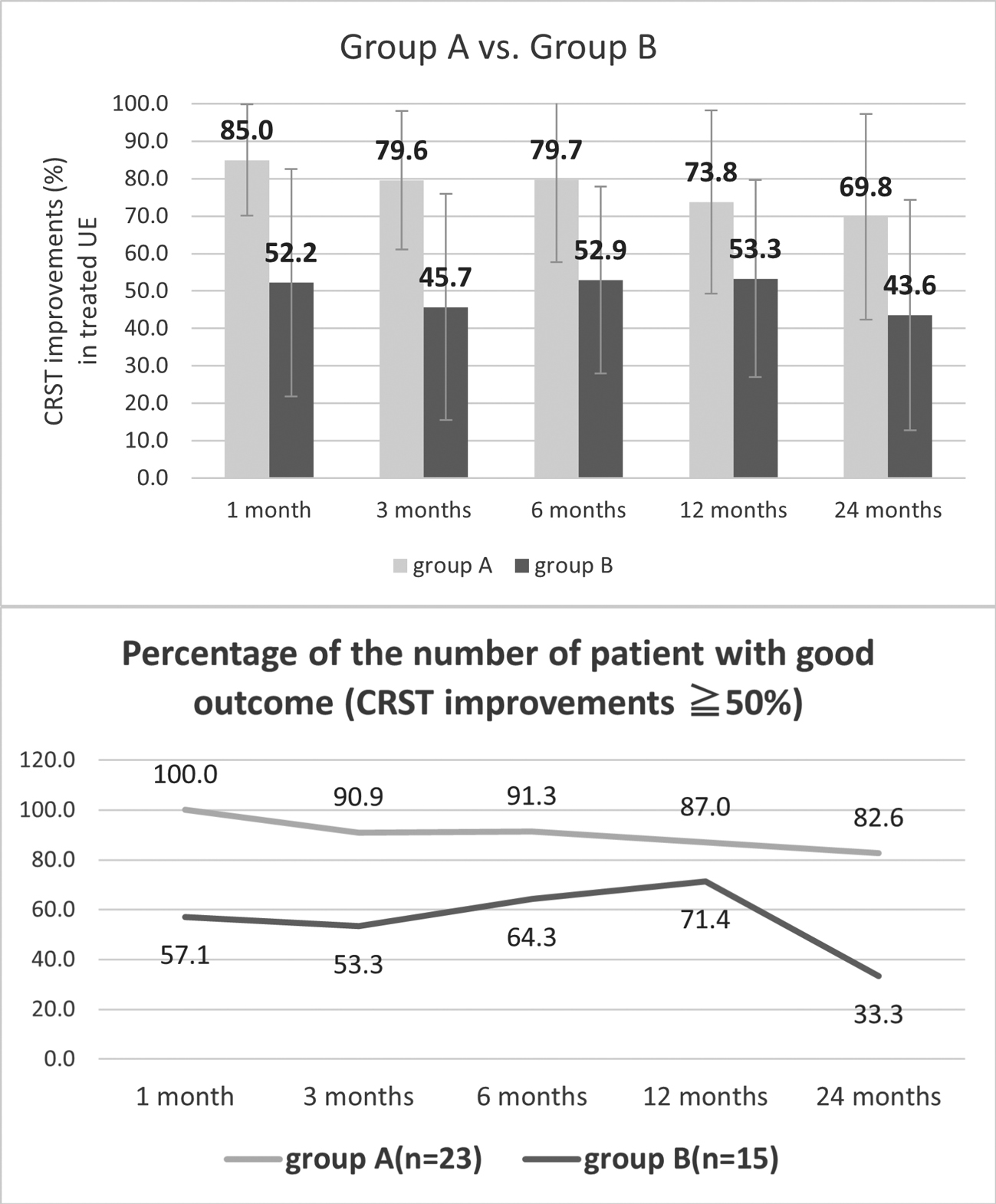 JOURNAL OPEN ACCESS
JOURNAL OPEN ACCESS
Supplementary materialMagnetic resonance-guided focused ultrasound (MRgFUS) thalamotomy is an effective treatment for essential tremor (ET). However, its long-term outcomes and prognostic factors remain unclear. This study aimed to retrospectively investigate 38 patients with ET who underwent MRgFUS thalamotomy and were followed up for >2 years. The improvement in tremor was evaluated using the Clinical Rating Scale for Tremor (CRST). Adverse events were documented, and correlations with factors, such as skull density ratio (SDR), maximum mean temperature (T-max), and lesion size, were examined. Furthermore, the outcomes were compared between two groups, one that met the cutoff values, which was previously reported (preoperative CRST-B ≤ 25, T-max ≥ 52.5°C, anterior-posterior size of lesion ≥ 3.9 mm, superior-inferior [SI] size of lesion > 5.5 mm), and the other that did not. The improvement rate was 59.4% on average at the 2-year follow-up. Adverse events, such as numbness (15.8%), dysarthria (10.5%), and lower extremity weakness (2.6%), were observed even after 2 years, although these were mild. The factors correlated with tremor improvement were the T-max and SI size of the lesion (p < 0.05), whereas the SDR showed no significance. Patients who met the aforementioned cutoff values demonstrated a 69.8% improvement at the 2-year follow-up, whereas others showed a 43.6% improvement (p < 0.05). In conclusion, MRgFUS is effective even after 2 years. The higher the T-max and the larger the lesion size, the better the tremor control. Previously reported cutoff values clearly predict the 2-year prognosis, indicating the usefulness of MRgFUS.
View full abstractDownload PDF (810K) -
Daina KASHIWAZAKI, Emiko HORI, Naoki AKIOKA, Kunitaka MARUYAMA, Shusuk ...2024 Volume 64 Issue 4 Pages 147-153
Published: April 15, 2024
Released on J-STAGE: April 15, 2024
Advance online publication: February 26, 2024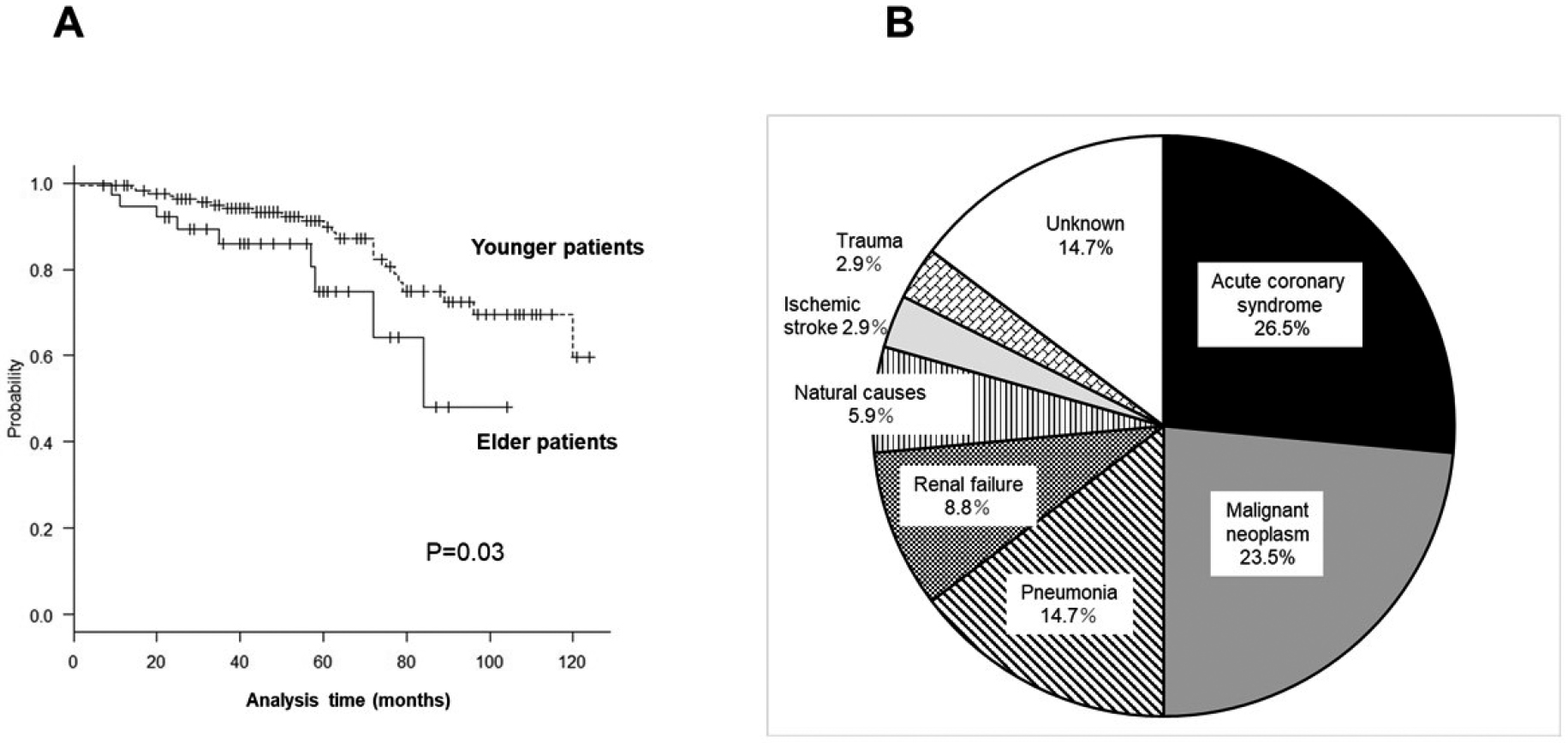 JOURNAL OPEN ACCESS
JOURNAL OPEN ACCESSAs the average life expectancy increases, neurosurgeons are likely to encounter patients aged 80 years and above with carotid stenosis; however, whether old age affects clinical post-treatment outcomes of carotid endarterectomy (CEA) or carotid artery stenting (CAS) remains inconclusive. Thus, this study aimed to evaluate the outcomes following CEA or CAS in patients aged 80 years and above. This study included older over 80 years (n = 34) and younger patients (<80 years; n = 222) who underwent CEA or CAS between 2012 and 2022. All of them were followed up for a mean of 55 months. All-cause mortality, the incidence of vascular events, ability to perform daily activities, and nursing home admission rates were assessed. During follow-up periods, 34 patients (13.3%) died due to coronary artery disease, malignancy, and pneumonia, and the incidence was significantly higher in the elderly group than in the younger group (P = 0.03; HR, 3.01; 95% CI, 1.53-5.56). The incidence of vascular events did not differ between the older group (29.5%) and the younger group (26.9%, P = 0.58); however, the incidence was significantly higher in patients with high-intensity plaques than in those without that (P = 0.008; HR, 2.83, 95%CI, 1.27-4.87). The decline in the ability to perform daily activities and increased nursing home admission rates were high in elderly patients (P < 0.01). Although the mortality rate was higher in the elderly group, subsequent vascular events were comparable to that in the younger group. The results suggest that CEA and CAS are safe and useful treatments for carotid stenosis in older patients, especially to prevent ipsilateral ischemic stroke.
View full abstractDownload PDF (297K)
-
Yuhei HOSHIKUMA, Takeshi SHIMIZU, Shingo TOYOTA, Tomoaki MURAKAMI, Tak ...2024 Volume 64 Issue 4 Pages 154-159
Published: April 15, 2024
Released on J-STAGE: April 15, 2024
Advance online publication: February 15, 2024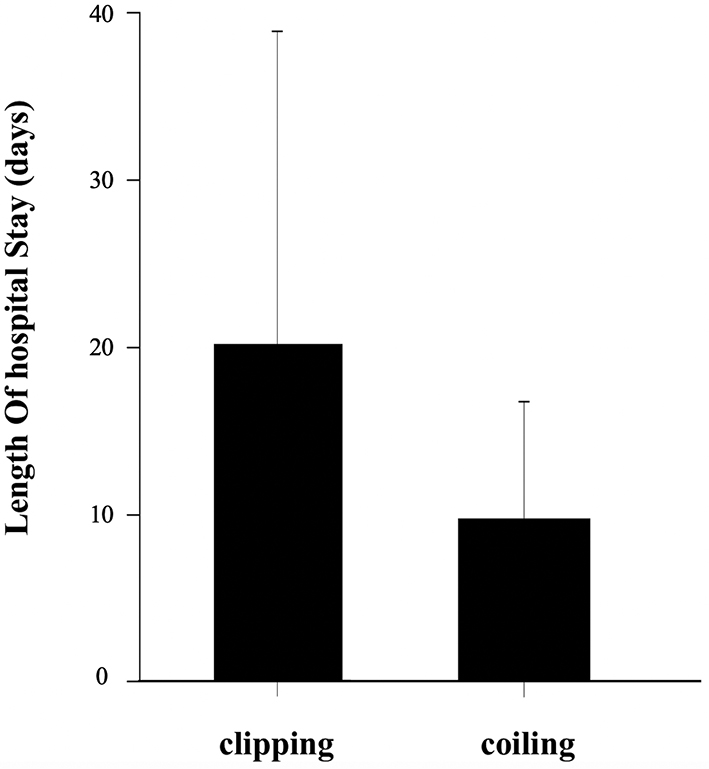 JOURNAL OPEN ACCESS
JOURNAL OPEN ACCESSTreatment strategies for unruptured intracranial aneurysms (UIAs) should be carefully considered with reference to rupture and complication rates. It is also important to minimize the length of hospital stay (LOS) and to ensure a high quality of medical care. In this study, we aim to clarify the factors that affect the LOS of patients treated for UIAs using the Inpatient Clinico-Occupational Database of the Rosai Hospital Group (ICOD-R). This was a nationwide-multicenter study based on ICOD-R data from 2000 to 2019. Patients diagnosed with UIAs who were treated with clipping or coiling were included in the study. Multivariate analysis was performed to identify the factors affecting LOS. LOS was also compared between groups classified by surgical procedure or treatment period. We identified 3294 patients on the database who underwent clipping or coiling of UIAs during the study period. Multivariate analysis revealed hospital admission during the early 2000s and the late 2010s, age, and treating institution to be significantly correlated with LOS (p < 0.05). There was a significant difference between the mean LOS of the clipping group (20.3 days) and the coiling group (9.65 days) (p < 0.001). Compared by treatment period, LOS significantly shortened over time. Our results suggest that the type of treatment, time of treatment, patient age, and the treating institution affect postoperative LOS for UIAs. Although coiling was found to lead to a lower average LOS than clipping, treatment selection should take the characteristics of each patient's aneurysm into consideration.
View full abstractDownload PDF (160K) -
Kosaku AMANO, Yuichi ODA, Yasufumi SEKI, Kaoru YAMASHITA, Kanako BOKUD ...2024 Volume 64 Issue 4 Pages 160-167
Published: April 15, 2024
Released on J-STAGE: April 15, 2024
Advance online publication: February 15, 2024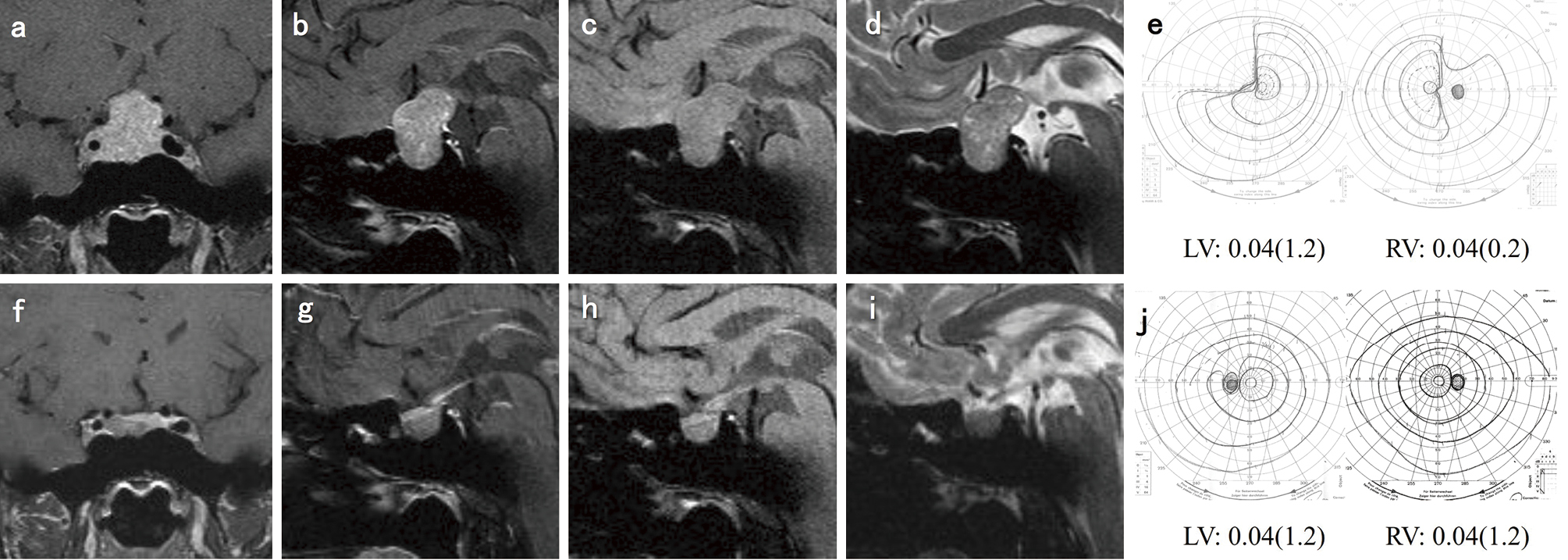 JOURNAL OPEN ACCESS
JOURNAL OPEN ACCESSProlactin-producing pituitary tumor (PRLoma) is the most prevalent functional pituitary tumor. If the tumor becomes large, vision can be impaired. In contrast to other pituitary tumors, cabergoline (CAB) is extremely effective for PRLoma and has become the first-line treatment. In this study, we examined our experience with the pharmacological and surgical management of PRLomas with visual impairment (VI) to determine whether VI could be a surgical indication. Further, we discussed the function of surgery in situations where the gold standard of PRLoma treatment was CAB administration. Of the 159 patients with PRLomas (age, 13-77 [mean = 36.3] years; men, 29; women, 130) at Tokyo Women's Medical University Hospital from 2009 to 2021, 18 (age, 15-67 [mean = 35.8] years; men, 12; woman, 6) had VI (subjectively, 12; objectively, 6). They started CAB treatment immediately (maximum dose: 0.5 to 6 mg/week; average: 2.17 mg/week). VI improved in 16 patients (88.9%) but did not improve in 2 (11.1%) requiring surgeries. One of the two patients had a parenchymal tumor resistant to CAB, and the other had a cystic tumor due to intratumoral bleeding. Consequently, CAB is the first-line treatment for PRLomas with VI because of its significantly high rate of improvement. However, close and rigorous surveillance is necessary for cases resistant to CAB, and the correct decision is required regarding surgical interventions at proper timing and appropriate surgical approaches considering the purpose of surgery.
View full abstractDownload PDF (1089K) -
Yoshiro ITO, Hisayuki HOSOO, Aiki MARUSHIMA, Yuji MATSUMARU, Eiichi IS ...2024 Volume 64 Issue 4 Pages 168-174
Published: April 15, 2024
Released on J-STAGE: April 15, 2024
Advance online publication: February 15, 2024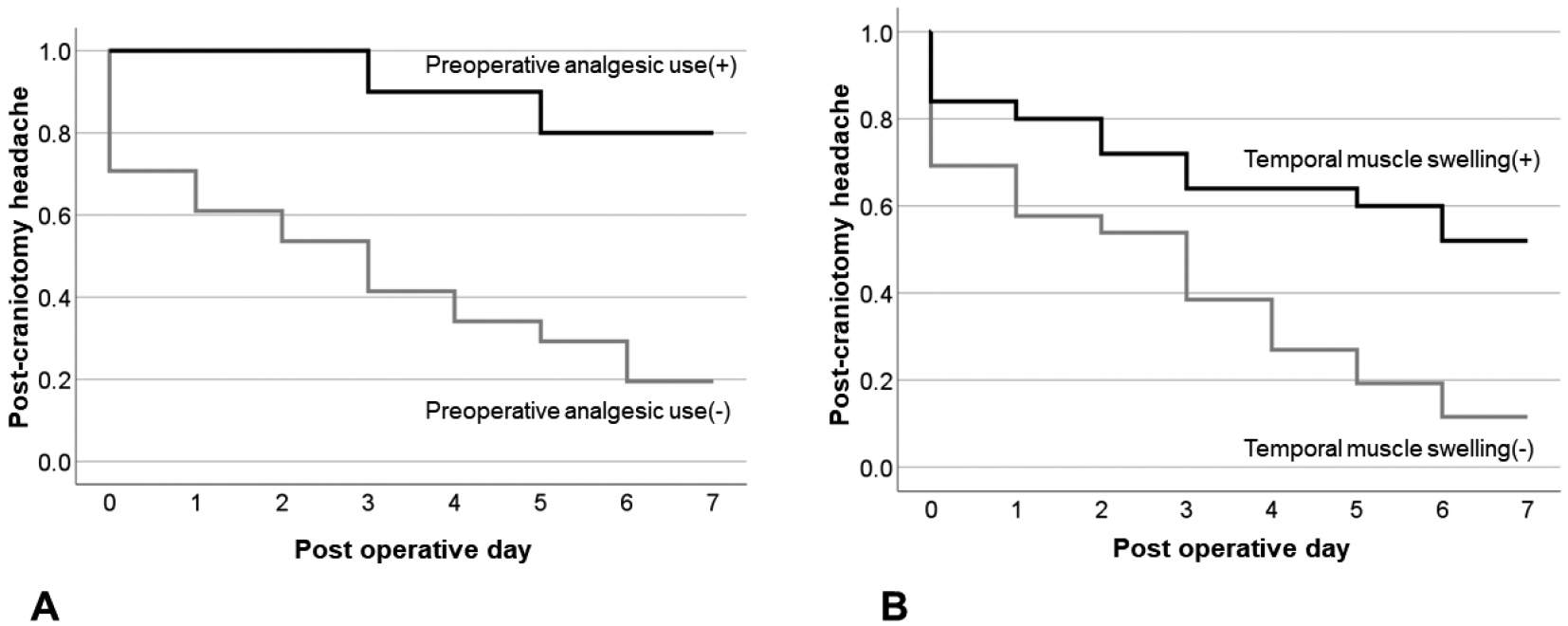 JOURNAL OPEN ACCESS
JOURNAL OPEN ACCESS
Supplementary materialImmediate postcraniotomy headache frequently occurs within the first 48 h after surgery. The mechanisms underlying immediate postcraniotomy headache are not yet fully understood, and effective treatments are not yet established. This study aimed to identify the factors associated with immediate postcraniotomy headache in patients who underwent clipping surgery with frontotemporal craniotomy and to examine the effects of these factors on postcraniotomy headache. A total of 51 patients were included in this study. Immediate postcraniotomy headache was defined as pain with numerical rating scale score ≥4 on postoperative day 7. Sixteen patients (31.4%) had immediate postcraniotomy headache. The headache-positive group had a higher incidence of preoperative analgesic use (50.0% vs. 5.7%, respectively, p < 0.001), increased temporal muscle swelling ratio (137.0%±30.2% vs. 112.5%±30.5%, respectively, p = 0.01), and higher postoperative analgesic use (12.9±5.8 vs. 6.7±5.2, respectively, p < 0.001) than the headache-negative group. The risk factors independently associated with immediate postcraniotomy headache were preoperative analgesic use and temporal muscle swelling by >115.15% compared with the contralateral side in the receiver operating characteristic analysis. Postcraniotomy headache was significantly more common in patients with preoperative analgesic use and temporal muscle swelling than in those without (p < 0.001 and p = 0.002, respectively). Altogether, patients with immediate postcraniotomy headache had greater preoperative analgesic use, greater temporal muscle swelling ratio, and higher postoperative analgesic use than those without. Thus, temporal muscle swelling is a key response to immediate postcraniotomy headache.
View full abstractDownload PDF (326K)
-
2024 Volume 64 Issue 4 Pages EC7-EC8
Published: April 15, 2024
Released on J-STAGE: April 15, 2024
JOURNAL OPEN ACCESSDownload PDF (55K)
- |<
- <
- 1
- >
- >|