Abstract
Background:
In heart failure patients, chronic hyperactivation of sympathetic signaling is known to exacerbate cardiac dysfunction. In this study, the cardioprotective effect of vidarabine, an anti-herpes virus agent, which we identified as a cardiac adenylyl cyclase inhibitor, in dogs with pacing-induced dilated cardiomyopathy (DCM) was evaluated. In addition, the adverse effects of vidarabine on basal cardiac function was compared to those of the β-blocker, carvedilol.
Methods and Results:
Vidarabine and carvedilol attenuated the development of pacing-induced systolic dysfunction significantly and with equal effectiveness. Both agents also inhibited the development of cardiac apoptosis and fibrosis and reduced the Na+-Ca2+
exchanger-1 protein level in the heart. Importantly, carvedilol significantly enlarged the left ventricle and atrium; vidarabine, in contrast, did not. Vidarabine-treated dogs maintained cardiac response to β-AR stimulation better than carvedilol-treated dogs did.
Conclusions:
Vidarabine may protect against pacing-induced DCM with less suppression of basal cardiac function than carvedilol in a dog model. (Circ J 2016; 80: 2496–2505)
Beta-adrenergic receptor (β-AR)-mediated signaling is hyperactivated in heart failure (HF) patients.1
Although the sympathetic nervous system is quite important in the maintenance of blood perfusion in various organs during acute HF, long-term hyperactivation of β-AR signaling exacerbates the development of left ventricular dysfunction and arrhythmia, which results in further deterioration of cardiac function.2
Consistently, β-AR blocking agents (β-blockers) have been demonstrated to prevent the development of cardiac dysfunction and improve prognosis of HF patients.3,4
They have one major adverse property, however; a negative inotropic effect, which can exacerbate HF. For this reason, it is recommended that treatment with β-blockers for patients with severe systolic dysfunction (eg, dilated cardiomyopathy; DCM) is initiated at low doses and increased by gradual increments under careful observation. Even when these recommendations are followed, some patients are intolerant to β-blockers.1,5
Thus, there is a great need for the development of a novel anti-sympathetic drug that does not suppress basal cardiac function and thus can be administered safely to patients with severe HF.
β-Adrenergic receptor stimulation first induces adenylyl cyclase (AC) activation, then increases intracellular cAMP concentration. The AC is composed of several isoforms,6
each of which is expressed in a tissue-specific manner. AC type 5 (AC5) is one of the dominant isoforms in the heart.7–9
Interestingly, our previous reports have suggested that AC5 does not contribute to maintaining basal cardiac function, though it does play a major role in exacerbating cardiac dysfunction due to its pathological activation of β-AR signaling. AC5 deficiency in mice caused no significant change in baseline hemodynamic parameters compared with the wild-type mice.10
In contrast, AC5 deficiency was protective against the development of HF induced by transverse aortic banding and chronic isoproterenol infusion.11,12
The protein expression levels of AC5 are upregulated in the failing heart.12,13
These findings indicate that AC5 accelerates the development of HF without affecting basal cardiac functions. Thus, we presumed that pharmacological inhibition of AC5 would offer protection against the development of HF without suppressing basal cardiac function, a desirable quality for HF therapy.
Previously, we discovered that vidarabine, 9-β-D-arabinofuranosyladenine, which is approved by the Food and Drug Administration (FDA) as an anti-herpes virus agent,14
inhibits cardiac AC activity.15
Vidarabine has higher selectivity for AC5 activity than for type 2 or 3 AC, both of which are more abundantly expressed in non-cardiac tissue.15
We reported that vidarabine improves cardiac function and survival time in a mouse HF model induced by myocardial infarction and chronic isoproterenol infusion.16
In addition, in healthy mice, acute treatment with vidarabine did not affect basal cardiac function.16
Similarly, vidarabine did not affect cardio-hemodynamic or electrophysiological variables in anesthetized healthy dogs.17
To further evaluate the usefulness of vidarabine for the treatment of severe HF, we used a canine model of pacing-induced DCM, which has been well-characterized in previous studies.18–20
Chronic rapid ventricular pacing causes a progressive and reliable model of DCM in dogs, pigs and sheep. This model shows a progression of functional, structural, and neurohormonal changes, similar to that associated with DCM in humans.19
In the present study, we assessed the effectiveness of vidarabine against this canine model of pacing-induced DCM. We also compared the therapeutic and adverse effects of vidarabine with those of carvedilol, one of the most commonly used β-blockers, by evaluating the degree to which cardiac responses to sympathetic activation were preserved during each type of therapy.
Methods
Instrumentation
Eighteen female beagles underwent surgical implantation of a pacing wire on the right ventricle, as described previously.21
The study was approved by the Animal Care and Use Committee of the College of Bioresource Science, Nihon University and performed by the Department of Veterinary Medicine, College of Bioresource Science of Nihon University, Japan.
Experimental Protocol
Figure 1
shows the schematic diagrams of our experimental procedure. All dogs underwent baseline hemodynamic recordings before the initiation of pacing (Day 0). Subsequently, HF was induced by rapid right ventricular pacing at a rate of 250 beats/min for 3 weeks. And then, after tachycardia pacing was decreased to 240 beats/min to limit mortality,22
vidarabine (24 mg·kg–1·day–1
i.v., n=6) or carvedilol (1 mg·kg–1·day–1
p.o., n=6) was administered for 7 days. Treatment was continued for another 3 days during which tachycardia pacing was suspended. Finally (Day 31), dogs were euthanized under general anesthesia, and their hearts were removed and sectioned for histological and biochemical examination.
Hemodynamic Studies
We collected hemodynamic data at several time points, as shown in
Figure 1. Cardiac function was evaluated by transthoracic echocardiography with the animals in a conscious state. The left ventricular internal diameter at diastole (LVIDd) and systole, the interventricular septal thickness at diastole, the left ventricular posterior wall thickness at diastole, the left ventricular fractional shortening (LVFS), and the ejection fraction were obtained through M mode echocardiogram. Left atrium diameter (LAD) was divided by the aortic root diameter taken from the same frame to obtain an LAD index. The cardiac output (CO) was calculated according to the pulsed Doppler echocardiogram method.23
The blood pressure was measured by the oscillometric method. Concomitantly, glomerular filtration rate (GFR) using urinary inulin clearance was measured for evaluation of renal function.24
All hemodynamic measurements were performed 30 min after cessation of pacing.
Histological Analyses
Left atrium and ventricle samples were used for histological analysis. Apoptosis in the tissue sections was examined by terminal dUTP nick end-labeling (TUNEL) staining. Interstitial fibrosis was evaluated by Sirius red staining.
Western Blot Analysis
Western blot analysis was performed, as previously described.25
In brief, homogenized tissue samples were separated on a 6% to 15% SDS-polyacrylamide gel and blotted onto polyvinylidene fluoride (PVDF) membranes. The membranes were then reacted with primary antibodies. The expression level of each protein was quantified by laser densitometry.
Cardiac Response to Isoproterenol Infusion
An isoproterenol challenge test was performed 10 days after the administration of the treatment agent (Day 31) using the method reported by Nikolaidis et al, with minor modifications.18
Isoproterenol was administered intravenously at a dosage of 0.02, 0.04 or 0.08 μg·kg–1·min–1
for 10 min. At the end of the dosage period, cardiac function was evaluated in a steady state.
Blood Measurements
Blood measurements were performed 10 days after administration of the treatment agent (Day 31). Plasma concentrations of alanine aminotransferase, aspartate aminotransferase, urea nitrogen, and creatinine were measured.
Statistical Analysis
All data are expressed as the mean±SEM. The differences in each parameter were analyzed by 1-way or 2-way analysis of variance, followed by post-hoc testing (Tukey-Kramer test). A value of P<0.05 was considered statistically significant.
Please refer to the Supplementary section for more detailed Methods information.
Results
Vidarabine Prevented Systolic Dysfunction in the Canine Pacing-Induced DCM Model
Chronic tachycardia pacing results in the progression of HF with a severe decrease in systolic function and enlargement of the left ventricle, as seen in human DCM.18
In the present study, 3 weeks of tachycardia pacing led to severe declines in LVFS, CO, and mean arterial pressure, and remarkable increases in the LVIDd and LAD indices, as
Figure 2
shows.

At this point in the experiment (Day 21), we initiated treatment with either vidarabine or carvedilol, and evaluated cardiac function at the 2 time points. We first assessed cardiac function after 7 days of concomitant treatment and tachycardia pacing (Day 28).26
Next, to assess whether the beneficial effects of the treatments were maintained during recovery from HF, we evaluated cardiac function 3 days after cessation of tachycardia pacing (Day 31). After cessation of tachycardia pacing, the tachycardia-induced DCM model shows recovery from cardiac dysfunction and chamber dilation.27,28
The hemodynamic characteristics of this recovery period are thought to resemble those achieved through appropriate medical therapy in patients with chronic HF.27
As shown in
Figure 3
and
Table S1, compared with placebo, vidarabine was associated with a significantly (P<0.01) greater degree of LVFS and a lower LAD index on Day 28; these significant (P<0.01) differences were preserved on Day 31. In addition, CO increased gradually after the initiation of vidarabine treatment and was significantly (P<0.01) higher after vidarabine treatment (Day 31) than it had been before (Day 21). Likewise, carvedilol was associated with a significantly (P<0.01) greater degree of LVFS on Day 28 compared with placebo, and this effect was preserved on Day 31. Yet carvedilol significantly (P<0.01) increased the LVIDd and LAD indices on Days 28 and 31 compared with their values before treatment (Day 21). In addition, carvedilol treatment led to a significantly (P<0.01) greater LAD index on Day 28 and significantly (P<0.05) greater LVIDd and LAD indices on Day 31 compared with the placebo- and vidarabine-treated groups. In the placebo-treated group, GFR, which is an index of renal function, tended to decline at Day 28. Under vidarabine or carvedilol treatment, however, GFR remained significantly (P<0.05) higher at the same time point. These results indicate that either vidarabine or carvedilol treatment can prevent the decline of systolic function during HF, enabling the maintenance of a significantly higher level of systolic function during the recovery period, in a canine pacing-induced DCM model. Interestingly, while carvedilol treatment enlarged the left ventricle and atrium, vidarabine did not induce such cardiac remodeling. In addition, vidarabine significantly increased CO, while carvedilol did not cause a significant change in this parameter.

We examined whether vidarabine or carvedilol treatment suppressed apoptosis and fibrosis in the left ventricle and atrium tissues in the canine pacing-induced DCM model. Myocardial apoptosis was evaluated by TUNEL staining, and cardiac interstitial fibrosis was evaluated by Sirius red staining. Both vidarabine and carvedilol treatment significantly (P<0.01) prevented myocardial apoptosis in both the left ventricle (Figure 4A) and the atrium (Figure 4B). To examine the changes in the molecules that are involved in apoptosis signaling, we examined the protein level of Bax, which is a promoter of apoptosis.25
A previous report has shown that chronic tachycardia pacing induces cardiomyocyte apoptosis, with an increasing level of Bax protein expression.29
In this study, Bax protein expression significantly (P<0.01) decreased in the left ventricle of vidarabine- and carvedilol-treated dogs compared with the placebo-treated group (Figure 4C). In addition, vidarabine and carvedilol treatment significantly (P<0.01) suppressed cardiac fibrosis in the left ventricle (Figure 5A) and atrium (Figure 5B) compared with the placebo-treated group.

Cardiac function is regulated by the intracellular Ca2+
concentration, which is modulated by the Ca2+-handling proteins located in the sarcoplasmic reticulum and the sarcolemmal membrane, including sarcoplasmic reticulum Ca2+-ATPase (SERCA2a), phospholamban (PLN), Na+-Ca2+
exchanger-1 (NCX1), and ryanodine receptor-2 (RYR2).30
Changes in the expression levels of these proteins in failing myocytes have been reported to result in abnormal intracellular Ca2+
homeostasis and cardiac dysfunction.31,32
We then examined the effect of vidarabine treatment on expression of calcium-handling proteins, as shown in
Figure 6. Although the protein levels of SERCA2a, PLN and RYR2 were not different among the treatment groups, the protein expression of NCX1 was significantly lower in the vidarabine- and carvedilol-treated groups compared with the placebo-treated group (P<0.01). These results indicate that the suppression of NCX1 expression by vidarabine or carvedilol might be one of the mechanisms underlying the cardioprotective effect of these agents against pacing-induced DCM.

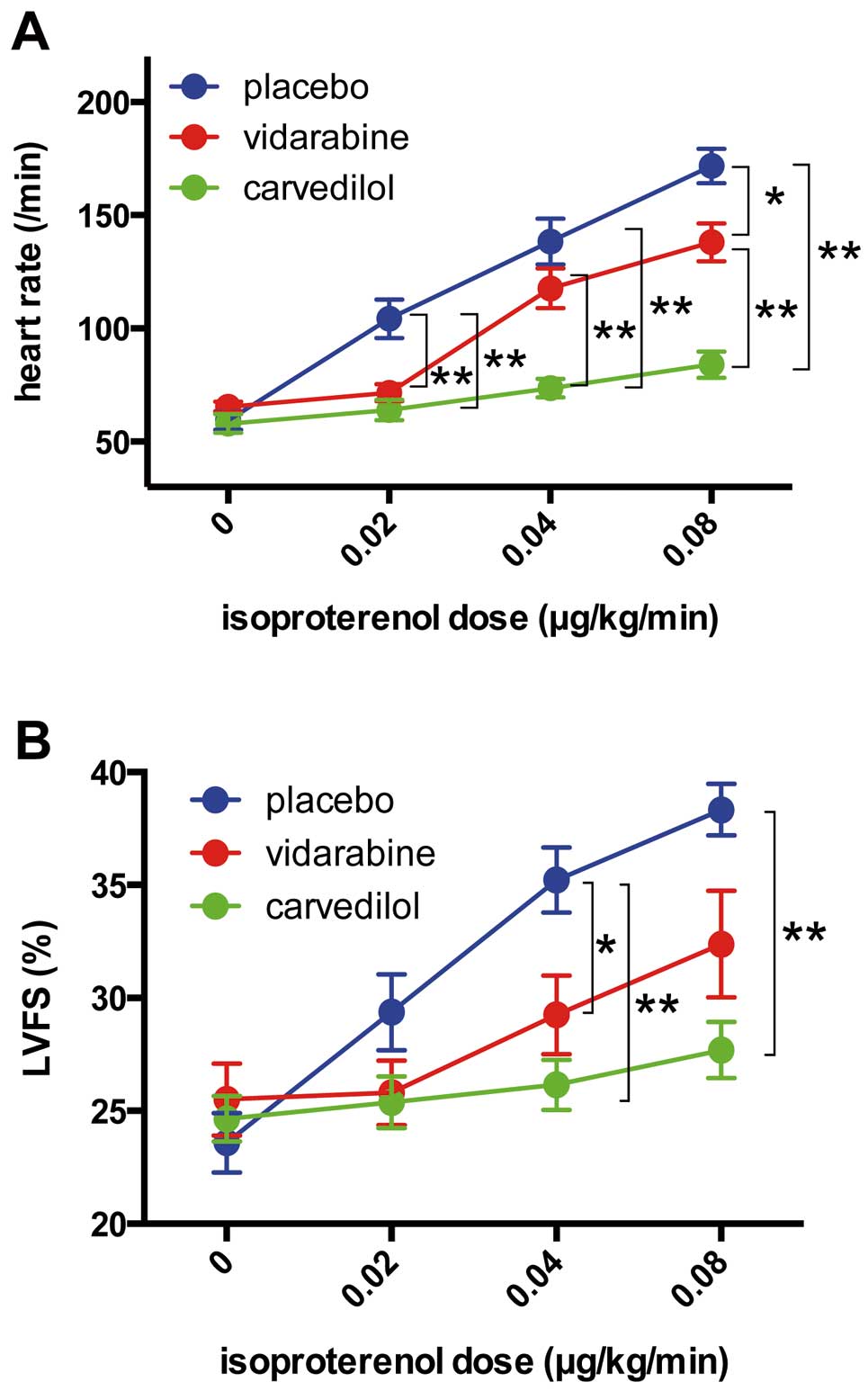
To evaluate the adverse effects of these agents on cardiac function, we examined the suppressive effect of vidarabine and carvedilol on positive chronotropic and inotropic responses to isoproterenol infusion. Although the positive chronotropic response to isoproterenol infusion was significantly (P<0.05) attenuated by both vidarabine and carvedilol compared with the placebo (Figure 7A), it remained significantly (P<0.01) higher in vidarabine-treated dogs than in carvedilol-treated dogs (Figure 7A). Similarly, during a 0.08 μg·kg–1·min–1
isoproterenol infusion, the inotropic response was significantly (P<0.01) attenuated in the carvedilol-treated group, but not in the vidarabine-treated group, compared with the placebo-treated group (Figure 7B).
Vidarabine Did Not Affect Plasma Parameters Related to Liver and Kidney Dysfunction
We evaluated the effect of vidarabine on plasma parameters related to liver and kidney dysfunction. As shown in
Table S2, there were no differences in the plasma concentrations of alanine aminotransferase, aspartate aminotransferase, urea nitrogen, and creatinine between the vidarabine and placebo groups after 10 days infusion of vidarabine (24 mg·kg–1·day–1) (Day 31).
Discussion
In this study, we demonstrated that vidarabine prevented the progression of cardiac systolic dysfunction and suppressed myocardial apoptosis and cardiac interstitial fibrosis in a canine pacing-induced DCM model. Previously, we reported that vidarabine prevented the development of HF in a mouse model with myocardial infarction and chronic isoproterenol infusion.16
In this study, as a next step, we evaluated the effects of vidarabine in a large-animal DCM model. In addition, we compared the therapeutic and adverse effects of vidarabine on cardiac function with those of carvedilol, the first-line drug for DCM.33
Our results indicated that vidarabine and carvedilol protect the heart with equal effectiveness against the development of pacing-induced DCM. Importantly, however, vidarabine caused less adverse effects on cardiac function compared with carvedilol.
Previous reports have shown that the expression levels of calcium-handling proteins are altered in dogs with pacing-induced DCM.34,35
The protein expression of NCX1 is increased after the development of HF,31,32,34
and this upregulation is related to impairment of cardiac contractile function.36
In addition, β-blocker treatment suppresses cardiac upregulation in a canine HF model.32
Based on these findings, normalization of the expression levels of calcium-handling proteins by β-blockers has been recognized as one mechanism underlying the beneficial effect of β-blockers in HF therapy.32,35
In this study, vidarabine and carvedilol attenuated the expression of NCX1, which plays a crucial role in the regulation of intracellular Ca2+
concentration, with equal effectiveness.30
The downregulation of NCX1 expression by vidarabine and carvedilol might be one of the mechanisms underlying the cardioprotective effects of these agents against pacing-induced DCM.
We previously reported that vidarabine treatment suppressed cardiac AC activity in mice.16
We evaluated forskolin-stimulated AC activity in the left ventricle of pacing-induced DCM dogs (Day 31). The AC activity in the heart of vidarabine-treated dogs was approximately 30% lower than that in placebo-treated dogs, although the differences did not achieve statistical significance (P=0.10; data not shown). Previous reports showed that cardiac AC activity was decreased in HF model animals.12,18
As the cardiac dysfunction was improved in vidarabine-treated dogs (Figure 3), the difference of HF severity between placebo- and vidarabine-treated groups might attenuate the difference of cardiac AC activity between these groups.
Interestingly, although carvedilol caused enlargement of the left ventricle and atrium, presumably as a result of the exacerbation of cardiac dysfunction,37–39
vidarabine did not cause this type of cardiac remodeling. In addition, the cardiac response to isoproterenol was preserved at a significantly higher level after treatment with vidarabine compared with carvedilol. In the previous study, β-blockade therapy resulted in cardiac dilation due to its negative inotropic effect in patients with chronic HF.37–39
In addition, Bozkurt et al reported that the slope of the velocity of circumferential fiber shortening to left ventricular end-systolic wall stress, a load-independent index of left ventricular contractility, worsened after the initiation of carvedilol despite improvement in left ventricular ejection fraction,40
suggesting that carvedilol therapy exerts a negative inotropic effect during the initiation period, and therefore that carvedilol may cause cardiac enlargement after the initiation of high-dose therapy (1 mg·kg–1·day–1). Vidarabine therapy (24 mg·kg–1·day–1), in contrast, although it is sufficient to attenuate cardiac dysfunction, apoptosis and fibrosis to a degree similar to that of carvedilol therapy, did not cause cardiac enlargement. Additionally, the vidarabine-treated group exhibited higher levels of cardiac response to sympathetic stimulation than the carvedilol-treated group did. Although long-term observation is needed to evaluate whether the maintenance of this response is beneficial or harmful for prognosis, it can be said that, during the period of this study, vidarabine treatment was as useful as carvedilol treatment in protecting against pacing-induced DCM with less adverse effects on cardiac function.
In this study, although both vidarabine and carvedilol treatment improved the LVFS, only vidarabine treatment significantly increased the CO (Figures 3F,G). A previous report showed that mitral regurgitation (MR) may develop in the evolution of HF in the pacing-induced DCM model.41
The severity of MR assessed by the MR jet area/left atrium area ratio was significantly greater in carvedilol-treated dogs compared with vidarabine-treated dogs on Day 28 (P<0.01; data not shown). Based on these findings, we speculated that greater MR is one of the reasons for the absence of the CO increase in carvedilol-treated dogs.
While recommending β-blockers for patients with DCM, the American Heart Association (AHA) guidelines warn healthcare professionals about their adverse effects, including negative inotropic effect, bradycardia and hypotension.33
To avoid the worsening of HF by adverse effects of β-blockers on cardiac function, it is recommended that therapy for patients with severe systolic dysfunction is initiated at low doses and gradually increased under careful monitoring for adverse signs.1,33
Because carvedilol yields improvement of cardiac function in a dose-related manner,42
however, this complicated initiation protocol increases the time required to obtain the beneficial effects of carvedilol.
In this study, we administered vidarabine at a dose of 24 mg·kg–1·day–1
and carvedilol at a dose of 1.0 mg·kg–1·day–1. This dose of carvedilol is equivalent to a final maintenance dose, which is recognized as the optimal dose for obtaining the maximum beneficial effect of carvedilol.3,4
The dose of vidarabine used in the present study, meanwhile, is 1.6-fold the maximum daily dose for herpes viral infection.14
A recent study found that no significant effects on hemodynamic and electrophysiological parameters were caused by 10 min of intravenous administration of vidarabine (100 mg/kg).17
Our results demonstrate that vidarabine (24 mg·kg–1·day–1) and carvedilol (1.0 mg·kg–1·day–1) prevented pacing-induced systolic dysfunction and development of apoptosis and fibrosis with equal effectiveness. In addition, vidarabine did not cause cardiac enlargement. These results indicate that vidarabine (24 mg·kg–1·day–1) can be initiated safely and that complicated initiation protocols, such as that recommended for β-blockers, may not be necessary, even for patients with severe cardiac dysfunction.
Vidarabine is FDA-approved and has been used as an anti-herpes virus drug for many decades.14
There have been no reports, however, about its possible adverse effects on liver and kidney function in HF patients. In our canine model with pacing-induced DCM, enzymes related to liver and kidney function, including alanine aminotransferase, aspartate aminotransferase, urea nitrogen and creatinine,43
were not significantly changed 10 days after the initiation of vidarabine treatment (24 mg·kg–1·day–1). In addition, GFR, the index of kidney function, was also preserved at its baseline level in the vidarabine- and carvedilol-treated groups, while that in the placebo-treated group decreased during progression of HF. Although the effect of long-term vidarabine administration needs to be examined, the present study results suggest the short-term safety of vidarabine (24 mg·kg–1·day–1) continuous therapy in a canine pacing-induced DCM model with regard to liver and kidney function.
Study Limitations
In this study, we observed the effects of 7 and 10 days’ treatment of each agent (vidarabine and carvedilol). These periods might be too short to fully examine the beneficial effect of both agents.3,4,40
In addition, in this study, carvedilol therapy was initiated at a relatively high dose (1.0 mg·kg–1·day–1) and caused cardiac enlargement, indicating that the high-dose initiation of carvedilol therapy may cause an adverse effect in this HF model. Relatively low-dose initiation followed by a stepwise increase might prevent the adverse effect. Importantly, in contrast, high-dose initiation of vidarabine therapy did not cause such an adverse effect and showed similar preventive effects compared with carvedilol therapy against the development of HF in this model.
In order to evaluate cardiac function, we used the LVFS in this study. However, LVFS is known as a load-dependent index. Our results showed no significant differences in mean arterial pressure and heart rate between the 3 groups. In contrast, it is noteworthy that carvedilol-treated dogs showed an increased LVIDd on Day 28 and 31 compared with Day 21 (Figure 3D), which was not seen in the other groups. In addition, as mentioned previously, significantly more severe MR was observed in carvedilol-treated dogs on Day 28 compared with vidarabine-treated dogs. These findings indicate that the left ventricular preload may be increased in the carvedilol-treated dogs. Therefore, it is possible that we have overestimated the cardiac function of the carvedilol-treated group. Importantly, even if we consider this point, we may be able to conclude that the preventive effect of vidarabine treatment against the pacing-induced cardiac systolic dysfunction was at least equal to that of carvedilol treatment.
Conclusions
In conclusion, vidarabine prevented pacing-induced systolic dysfunction and development of apoptosis and fibrosis to a degree similar to that achieved by carvedilol in a canine pacing-induced DCM model. Importantly, vidarabine did not cause cardiac enlargement. In addition, the response of cardiac function to sympathetic activation was maintained at a higher level in the vidarabine-treated group than in the carvedilol-treated group. These findings indicate that, compared with carvedilol, vidarabine may be a safer, yet equally cardioprotective anti-sympathetic agent against the development of HF in patients with severe cardiac dysfunction.
Acknowledgments
The authors thank Naoko Doi for her excellent technical assistance.
Sources of Funding
This study was supported, in part, by the Japan Society for the Promotion of Science (JSPS) KAKENHI Grant (16K08501 to T.F., 16H05300, 16K15205 to Y.I.); the Ministry of Education, Culture, Sports, Science and Technology (MEXT) KAKENHI Grant (22136009 to Y.I.); the Japan Agency for Medical Research and Development (AMED) (66890005, 66890011, 66890001, 66890023 to Y.I.) and a Grant for Strategic Research Promotion of Yokohama City University (T.F.).
Disclosure
All authors declare no conflicts of interest.
Supplementary Files
Supplementary File 1
Methods
Table S1.
Effects of vidarabine or carvedilol treatment on the parameters of left ventricular function and systemic hemodynamics
Table S2.
Plasma parameters in dogs 10 days after treatment
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-16-0736
References
- 1.
Bristow MR. Adrenergic receptor blockade in chronic heart failure. Circulation 2000; 101: 558–569.
- 2.
El-Armouche A, Eschenhagen T. Beta-adrenergic stimulation and myocardial function in the failing heart. Heart Fail Rev 2009; 14: 225–241.
- 3.
Packer M, Bristow MR, Cohn JN, Colucci WS, Fowler MB, Gilbert EM, et al. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure: U.S. Carvedilol Heart Failure Study Group. N Engl J Med 1996; 334: 1349–1355.
- 4.
Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, Mohacsi P, et al. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med 2001; 344: 1651–1658.
- 5.
Ko DT, Hebert PR, Coffey CS, Sedrakyan A, Curtis JP, Krumholz HM. Beta-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA 2002; 288: 351–357.
- 6.
Ishikawa Y, Homcy CJ. The adenylyl cyclases as integrators of transmembrane signal transduction. Circ Res 1997; 80: 297–304.
- 7.
Ishikawa Y, Katsushika S, Chen L, Halnon NJ, Kawabe J, Homcy CJ. Isolation and characterization of a novel cardiac adenylylcyclase cDNA. J Biol Chem 1992; 267: 13553–13557.
- 8.
Katsushika S, Chen L, Kawabe J, Nilakantan R, Halnon NJ, Homcy CJ, et al. Cloning and characterization of a sixth adenylyl cyclase isoform: Types V and VI constitute a subgroup within the mammalian adenylyl cyclase family. Proc Natl Acad Sci U S A 1992; 89: 8774–8778.
- 9.
Espinasse I, Iourgenko V, Defer N, Samson F, Hanoune J, Mercadier JJ. Type V, but not type VI, adenylyl cyclase mRNA accumulates in the rat heart during ontogenic development: Correlation with increased global adenylyl cyclase activity. J Mol Cell Cardiol 1995; 27: 1789–1795.
- 10.
Okumura S, Kawabe J, Yatani A, Takagi G, Lee MC, Hong C, et al. Type 5 adenylyl cyclase disruption alters not only sympathetic but also parasympathetic and calcium-mediated cardiac regulation. Circ Res 2003; 93: 364–371.
- 11.
Okumura S, Takagi G, Kawabe J, Yang G, Lee MC, Hong C, et al. Disruption of type 5 adenylyl cyclase gene preserves cardiac function against pressure overload. Proc Natl Acad Sci U S A 2003; 100: 9986–9990.
- 12.
Okumura S, Vatner DE, Kurotani R, Bai Y, Gao S, Yuan Z, et al. Disruption of type 5 adenylyl cyclase enhances desensitization of cyclic adenosine monophosphate signal and increases Akt signal with chronic catecholamine stress. Circulation 2007; 116: 1776–1783.
- 13.
Hu CL, Chandra R, Ge H, Pain J, Yan L, Babu G, et al. Adenylyl cyclase type 5 protein expression during cardiac development and stress. Am J Physiol Heart Circ Physiol 2009; 297: H1776–H1782.
- 14.
Whitley RJ, Alford CA, Hirsch MS, Schooley RT, Luby JP, Aoki FY, et al. Vidarabine versus acyclovir therapy in herpes simplex encephalitis. N Engl J Med 1986; 314: 144–149.
- 15.
Iwatsubo K, Minamisawa S, Tsunematsu T, Nakagome M, Toya Y, Tomlinson JE, et al. Direct inhibition of type 5 adenylyl cyclase prevents myocardial apoptosis without functional deterioration. J Biol Chem 2004; 279: 40938–40945.
- 16.
Iwatsubo K, Bravo C, Uechi M, Baljinnyam E, Nakamura T, Umemura M, et al. Prevention of heart failure in mice by an antiviral agent that inhibits type 5 cardiac adenylyl cyclase. Am J Physiol Heart Circ Physiol 2012; 302: H2622–H2628.
- 17.
Wada T, Nakamura Y, Cao X, Ohara H, Izumi-Nakaseko H, Ando K, et al. Antiviral drug vidarabine possessing cardiac type 5 adenylyl cyclase inhibitory property did not affect cardiohemodynamic or electrophysiological variables in the halothane-anesthetized dogs. J Toxicol Sci 2016; 41: 115–122.
- 18.
Nikolaidis LA, Poornima I, Parikh P, Magovern M, Shen YT, Shannon RP. The effects of combined versus selective adrenergic blockade on left ventricular and systemic hemodynamics, myocardial substrate preference, and regional perfusion in conscious dogs with dilated cardiomyopathy. J Am Coll Cardiol 2006; 47: 1871–1881.
- 19.
Houser SR, Margulies KB, Murphy AM, Spinale FG, Francis GS, Prabhu SD, et al. Animal models of heart failure: A scientific statement from the American Heart Association. Circ Res 2012; 111: 131–150.
- 20.
Woitek F, Zentilin L, Hoffman NE, Powers JC, Ottiger I, Parikh S, et al. Intracoronary cytoprotective gene therapy: A study of VEGF-B167 in a pre-clinical animal model of dilated cardiomyopathy. J Am Coll Cardiol 2015; 66: 139–153.
- 21.
Ishikawa Y, Sorota S, Kiuchi K, Shannon RP, Komamura K, Katsushika S, et al. Downregulation of adenylylcyclase types V and VI mRNA levels in pacing-induced heart failure in dogs. J Clin Invest 1994; 93: 2224–2229.
- 22.
Hanna N, Cardin S, Leung TK, Nattel S. Differences in atrial versus ventricular remodeling in dogs with ventricular tachypacing-induced congestive heart failure. Cardiovasc Res 2004; 63: 236–244.
- 23.
Lewis JF, Kuo LC, Nelson JG, Limacher MC, Quinones MA. Pulsed Doppler echocardiographic determination of stroke volume and cardiac output: Clinical validation of two new methods using the apical window. Circulation 1984; 70: 425–431.
- 24.
Nishida M, Uechi M, Kono S, Harada K, Fujiwara M. Estimating glomerular filtration rate in healthy dogs using inulin without urine collection. Res Vet Sci 2012; 93: 398–403.
- 25.
Okumura S, Fujita T, Cai W, Jin M, Namekata I, Mototani Y, et al. Epac1-dependent phospholamban phosphorylation mediates the cardiac response to stresses. J Clin Invest 2014; 124: 2785–2801.
- 26.
Reiken S, Gaburjakova M, Gaburjakova J, He Kl KL, Prieto A, Becker E, et al. Beta-adrenergic receptor blockers restore cardiac calcium release channel (ryanodine receptor) structure and function in heart failure. Circulation 2001; 104: 2843–2848.
- 27.
Shinagawa K, Shi YF, Tardif JC, Leung TK, Nattel S. Dynamic nature of atrial fibrillation substrate during development and reversal of heart failure in dogs. Circulation 2002; 105: 2672–2678.
- 28.
Cha TJ, Ehrlich JR, Zhang L, Shi YF, Tardif JC, Leung TK, et al. Dissociation between ionic remodeling and ability to sustain atrial fibrillation during recovery from experimental congestive heart failure. Circulation 2004; 109: 412–418.
- 29.
Moe GW, Naik G, Konig A, Lu X, Feng Q. Early and persistent activation of myocardial apoptosis, bax and caspases: Insights into mechanisms of progression of heart failure. Pathophysiology 2002; 8: 183–192.
- 30.
Marks AR. Calcium cycling proteins and heart failure: Mechanisms and therapeutics. J Clin Invest 2013; 123: 46–52.
- 31.
Mishra S, Sabbah HN, Rastogi S, Imai M, Gupta RC. Reduced sarcoplasmic reticulum Ca2+ uptake and increased Na+-Ca2+ exchanger expression in left ventricle myocardium of dogs with progression of heart failure. Heart Vessels 2005; 20: 23–32.
- 32.
George I, Sabbah HN, Xu K, Wang N, Wang J. Beta-adrenergic receptor blockade reduces endoplasmic reticulum stress and normalizes calcium handling in a coronary embolization model of heart failure in canines. Cardiovasc Res 2011; 91: 447–455.
- 33.
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013; 128: e240–e327, doi:10.1161/CIR.0b013e31829e8776.
- 34.
Lu L, Mei DF, Gu AG, Wang S, Lentzner B, Gutstein DE, et al. Exercise training normalizes altered calcium-handling proteins during development of heart failure. J Appl Physiol (1985) 2002; 92: 1524–1530.
- 35.
Mochizuki M, Yano M, Oda T, Tateishi H, Kobayashi S, Yamamoto T, et al. Scavenging free radicals by low-dose carvedilol prevents redox-dependent Ca2+ leak via stabilization of ryanodine receptor in heart failure. J Am Coll Cardiol 2007; 49: 1722–1732.
- 36.
Schillinger W, Janssen PM, Emami S, Henderson SA, Ross RS, Teucher N, et al. Impaired contractile performance of cultured rabbit ventricular myocytes after adenoviral gene transfer of Na(+)-Ca(2+) exchanger. Circ Res 2000; 87: 581–587.
- 37.
Ikram H, Chan W, Bennett SI, Bones PJ. Haemodynamic effects of acute beta-adrenergic receptor blockade in congestive cardiomyopathy. Br Heart J 1979; 42: 311–315.
- 38.
Ikram H, Fitzpatrick D. Double-blind trial of chronic oral beta blockade in congestive cardiomyopathy. Lancet 1981; 2: 490–493.
- 39.
Ikram H, Fitzpatrick D, Crozier IG. Therapeutic controversies with use of beta-adrenoceptor blockade in heart failure. Am J Cardiol 1993; 71: 54c–60c.
- 40.
Bozkurt B, Bolos M, Deswal A, Ather S, Chan W, Mann DL, et al. New insights into mechanisms of action of carvedilol treatment in chronic heart failure patients--a matter of time for contractility. J Card Fail 2012; 18: 183–193.
- 41.
Maniu CV, Patel JB, Reuter DG, Meyer DM, Edwards WD, Rihal CS, et al. Acute and chronic reduction of functional mitral regurgitation in experimental heart failure by percutaneous mitral annuloplasty. J Am Coll Cardiol 2004; 44: 1652–1661.
- 42.
Bristow MR, Gilbert EM, Abraham WT, Adams KF, Fowler MB, Hershberger RE, et al. Carvedilol produces dose-related improvements in left ventricular function and survival in subjects with chronic heart failure: MOCHA Investigators. Circulation 1996; 94: 2807–2816.
- 43.
Ambrosy AP, Dunn TP, Heidenreich PA. Effect of minor liver function test abnormalities and values within the normal range on survival in heart failure. Am J Cardiol 2015; 115: 938–941.