A 59-year-old woman with biopsy-proven and genetically proven Anderson-Fabry disease was referred for evaluation of myocardial microvascular ischemia because of chest discomfort. Stress/rest computed tomography (CT) perfusion (CTP) was performed with a 320-row multidetector CT (Aquilion ONE ViSION; Toshiba, Tokyo, Japan) (Figure). The prospective electrocardiography-gated CTP parameters were 320×0.5 mm collimation, 200 mA and 80 kVp. The patient was ordered to avoid caffeine 24 h before adenosine triphosphate (ATP) stress test. The CTP protocol included ATP-stress dynamic myocardial perfusion imaging, rest dynamic perfusion imaging, and rest coronary CT angiography (CCTA). ATP was infused i.v. over 3 min at a rate of 0.16 mg/kg/min using an infusion pump on the opposite-side arm for contrast injection. Three minutes after the ATP infusion, 50-mL non-ionic contrast agent (370 mgI/mL) was injected at a rate of 5 mL/s, followed by a 20-mL saline flush. The dynamic perfusion image data were acquired during the diastolic phase of 15 heartbeats. CTP showed left ventricular hypertrophy, with stress imaging showing a partial-thickness area of hypoperfusion involving the anterior wall with no associated coronary stenosis on CCTA. The CTP imaging was analyzed using a workstation (ZIO station 2, ZIO soft, Tokyo, Japan), and the myocardial blood flow (MBF) was calculated with the maximum slope method. The MBF in the defect was decreased on stress CTP (131.4 mL/100 g/min).
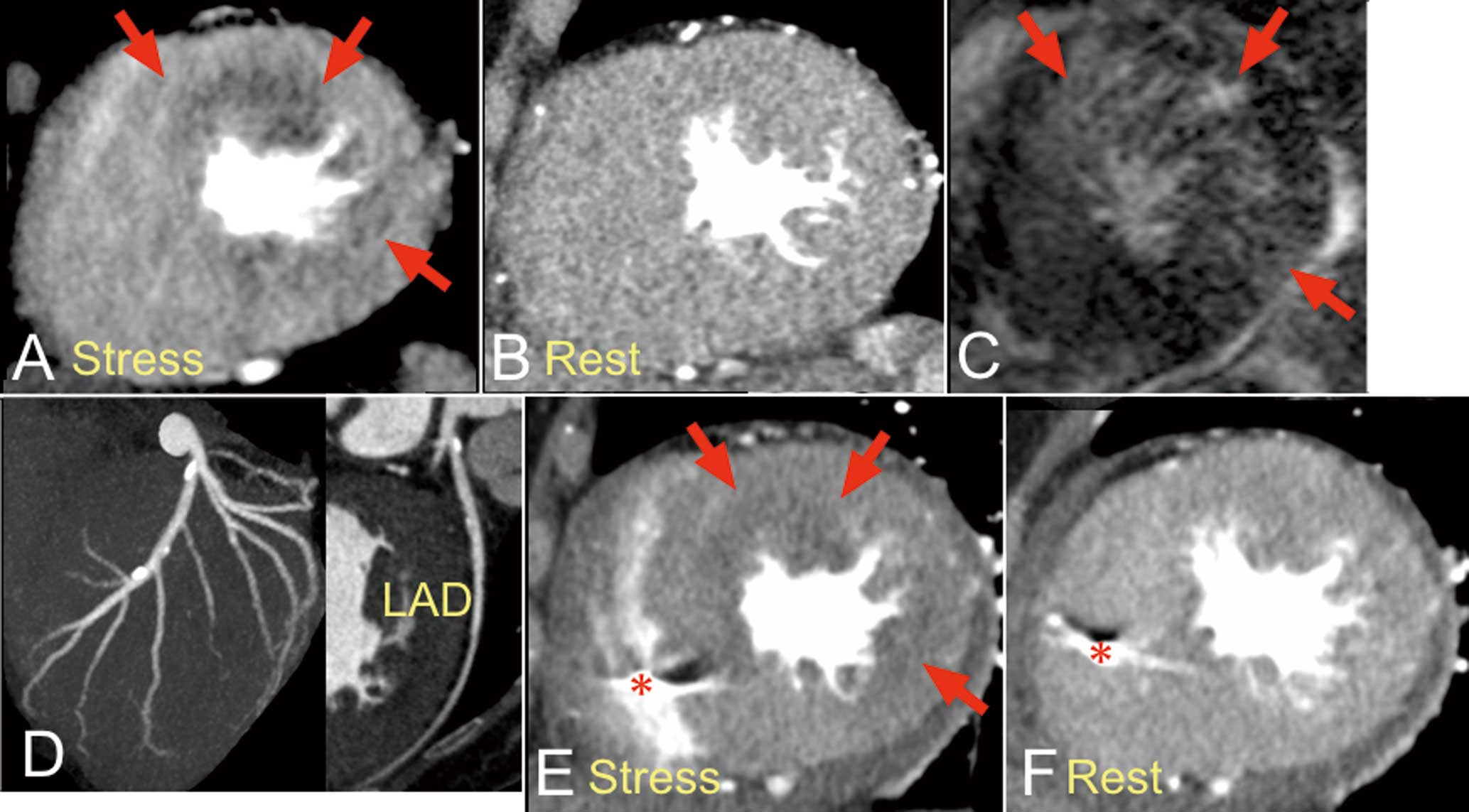
The patient began enzyme replacement therapy (ERT). After 2 years of ERT, the ischemic area became obscured on follow-up stress/rest CTP. The MBF had improved (173.0 mL/100 g/min).
Anderson-Fabry disease is an X-linked glycolipid storage disease with a deficient expression of the key enzyme a-galactosidase A.1
In the heart, progressive left ventricular hypertrophy due to glycosphingolipid deposition is one of the most common manifestations. Deposition of glycosphingolipid within smooth muscle and endothelial cells causes narrowing of the small intramural coronary arteries.2,3
ERT is standard therapy for Anderson-Fabry disease, and clears microvascular endothelial glycosphingolipid deposits.4
Integrated CTP and CCTA were reportedly associated with improved diagnostic accuracy for the detection of significant ischemia.5,6
The usefulness for the detection of microvascular ischemia, however, has not been reported. To our knowledge, this is the first patient with Anderson-Fabry disease to undergo CTP and CCTA demonstrating microvascular ischemia and the treatment response. CTP can be a useful technique for detecting microvascular ischemia. Furthermore, CTP is more advantageous over magnetic resonance imaging because CT can be used for patients with implanted permanent pacemaker.
References
- 1.
Thurberg BL, Fallon JT, Mitchell R, Aretz T, Gordon RE, O’Callaghan MW. Cardiac microvascular pathology in Fabry disease: Evaluation of endomyocardial biopsies before and after enzyme replacement therapy. Circulation 2009; 119: 2561–2567.
- 2.
Frustaci A, Russo MA, Francone M, Chimenti C. Microvascular angina as prehypertrophic presentation of Fabry disease cardiomyopathy. Circulation 2014; 130: 1530–1531.
- 3.
Heusch G. Coronary microcirculation: A neglected target of cardioprotection. Circ J 2014; 78: 1830–1831.
- 4.
Thurberg BL, Rennke H, Colvin RB, Dikman S, Gordon RE, Collins AB, et al. Globotriaosylceramide accumulation in the Fabry kidney is cleared from multiple cell types after enzyme replacement therapy. Kidney Int 2002; 62: 1933–1946.
- 5.
Rochitte CE, George RT, Chen MY, Arbab-Zadeh A, Dewey M, Miller JM, et al. Computed tomography angiography and perfusion to assess coronary artery stenosis causing perfusion defects by single photon emission computed tomography: The CORE320 study. Eur Heart J 2014; 35: 1120–1130.
- 6.
Sato A, Aonuma K. Role of cardiac multidetector computed tomography beyond coronary angiography. Circ J 2015; 79: 712–720.
