Images in Cardiovascular Medicine
Acute Aortic Valve Regurgitation Due to Spontaneous Rupture of Fenestrated Cusp Treated With Aortic Valve Repair
2017 Volume 81 Issue 2 Pages 241-242

Details
2017 Volume 81 Issue 2 Pages 241-242
Spontaneous rupture of a fenestrated cusp is one of the causes of acute aortic valve regurgitation (AR),1 but preoperative diagnosis of spontaneous rupture of fenestrated cusp causing severe AR is difficult.
A 56-year-old man was referred for sudden onset of nocturnal dyspnea. He had no previous history of trauma and no evidence of systemic infection. Chest X-ray showed cardiomegaly and pulmonary edema. Transthoracic echocardiography indicated a mildly dilated left ventricular chamber with left ventricular ejection fraction of 55%. The aortic valve was tricuspid. The right coronary cusp (RCC) was prolapsed with eccentric regurgitation. Regurgitation volume was 64 ml; regurgitation fraction, 52%; effective orifice area, 0.36 cm2; and pressure half time, 220 ms, indicating severe AR. On transesophageal echocardiography (TEE) no enlargement of the aortic root was seen, but the free RCC margin was frail. Three-dimensional TEE confirmed that the RCC free margin on the left coronary cusp (LCC) side was frail (Figure A), causing severe AR with an eccentric jet (Figure B,C). A ruptured fibrous strand was attached to the LCC side of the RCC (Figure D,E; Movies S1,S2). This case was thus diagnosed as AR due to spontaneous rupture of fenestrated cusp. The patient underwent aortic valve repair. Intraoperative findings confirmed that the ruptured fibrous strand originated from the LCC side of the RCC (Figure F). The existing tissue defect was closed with an autologous pericardial patch, and central plication of all three cusps (Figure G). No residual AR was detected after surgery.
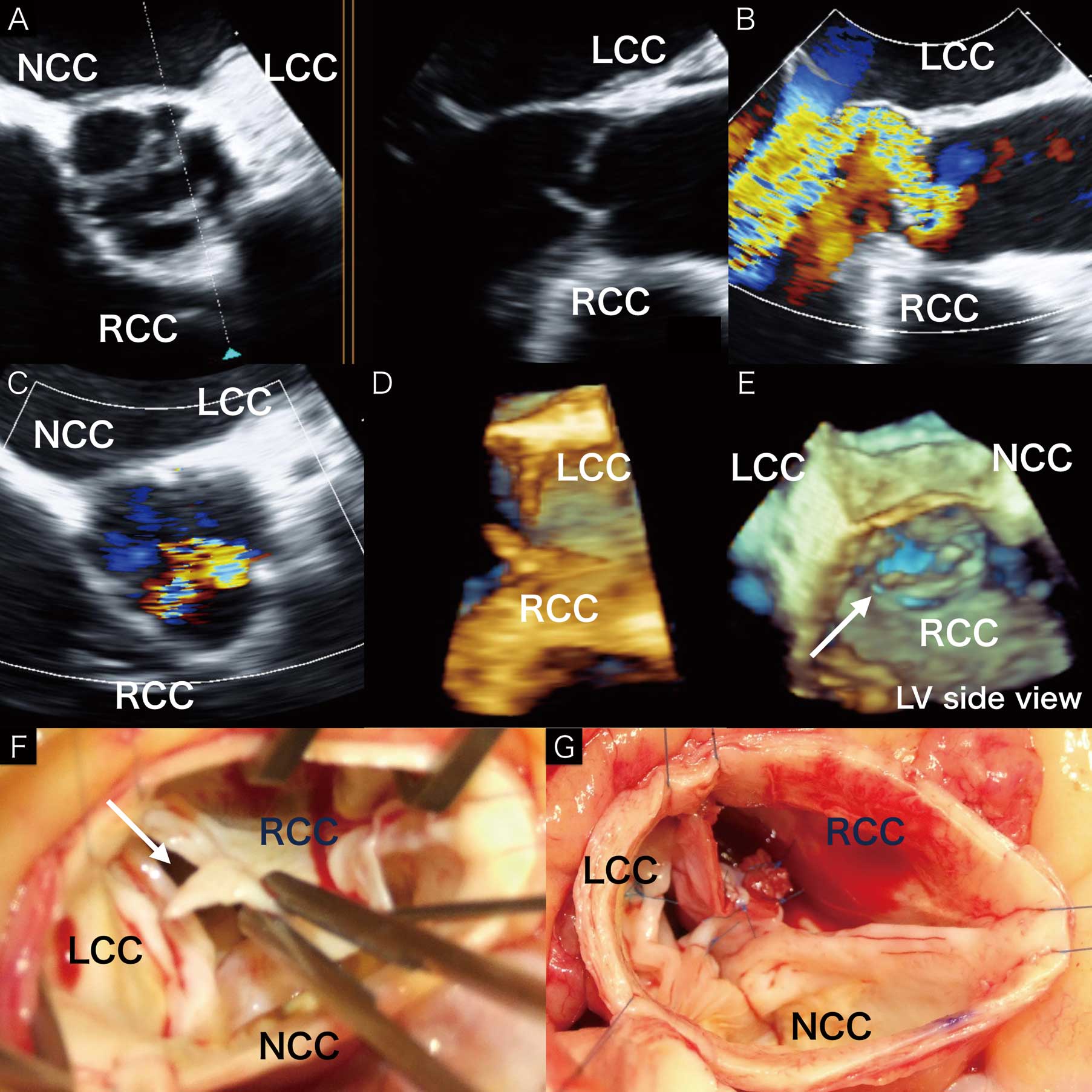
(A–E) Transesophageal echocardiography (TEE). (A) Biplanar view: (Right panel) long-axis (LAX) view showing left coronary cusp (LCC) and right coronary cusp (RCC). (B) Color Doppler LAX view indicating RCC prolapse. (C) Aortic regurgitant orifice on the LCC side of the RCC. NCC, non-coronary cusp. (D,E) Three-dimensional TEE showing a ruptured fibrous strand attached to the LCC side of the RCC (white arrow). (F,G) Operative findings. LV, left ventricle.
Aortic valve repair has become an accepted alternative to aortic valve replacement in significant AR.2 This is the first documented 3D-TEE visualization of spontaneous rupture of fenestrated cusp, successfully treated with aortic valve repair. The cause of AR should be clarified, to ensure effective aortic valve repair.
All procedures performed in studies involving human participants were in accordance with the ethics standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethics standards. Informed consent was obtained from all individual participants included in the study.
This study was partially funded by grant H9-2015 from the Sakakibara Clinical Research Grant for Promotion of Science (2015).
The authors declare no conflict of interest.
Supplementary File 1
Movie S1. Long-axis view of transesophageal echocardiography (TEE).
Supplementary File 2
Movie S2. Left vetricular side view of 3-dimensional TEE.
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-16-0959