Abstract
Background:
To clarify the effects of warfarin therapy in very old patients with non-valvular atrial fibrillation (NVAF), a post-hoc analysis was performed using the data of the J-RHYTHM Registry.
Methods and Results:
A consecutive series of AF outpatients was enrolled from 158 institutions. Of 7,937 patients, 7,406 with NVAF (men, 70.8%; 69.8±10.0 years) were followed for 2 years or until an event occurred. Patients were divided into 3 age groups (<70, 70–84, and ≥85 years) and 5 subgroups according to international normalized ratio (INR; <1.6, 1.6–1.99, 2.0–2.59, 2.6–2.99, and ≥3.0). Prevalence of female sex, permanent AF, hypertension, coronary artery disease, heart failure, and history of ischemic stroke/transient ischemic attack was higher in the older groups. In the oldest group, 79.7% of patients received warfarin and their time in therapeutic range, using the Japanese target INR of 1.6–2.6, was 67.1%. Rate of thromboembolic events was lower in the age groups <70 and 70–84 years (P=0.027 and P<0.001, respectively) for patients receiving warfarin compared with those who were not. In the oldest group, the rate of thromboembolism plus major hemorrhage was lower at INR 1.6–2.59.
Conclusions:
Warfarin could have beneficial effects even in very old NVAF patients if INR is kept between 1.6 and 2.59.
Atrial fibrillation (AF) is the most common arrhythmia in subjects of advanced age and is a potent risk factor for cardiogenic embolism.1,2
The prevalence of AF in the population aged ≥80 years is approximately 7–14% in Western countries3,4
and 2–3% in Japan.5,6
The number of subjects with AF can be expected to increase further with the aging of society.4–6
According to a recent population-based study from the UK,7
the number of AF-related ischemic strokes at age ≥80 years has trebled over the last 25 years and is projected to treble again by 2050. Given that aging per se is a potent risk factor for stroke,8
prophylaxis with anticoagulation therapy is especially important for reducing AF-related ischemic stroke in elderly patients.
Editorial p ????
Although several non-vitamin K antagonist oral anticoagulants (NOAC) have been available for anticoagulation therapy in patients with non-valvular AF (NVAF), the use of NOAC in elderly patients is limited, apparently because evidence of their safety is lacking. In contrast, warfarin has been widely used in the real-world clinical setting and is more effective than aspirin in NVAF patients aged ≥75 years.9
In several guidelines for the management of AF,10,11
an international normalized ratio (INR) of prothrombin time between 2.0 and 3.0 is recommended for patients with NVAF, regardless of age. In contrast, Japanese guidelines recommend a slightly lower INR of 1.6–2.6 for elderly (≥70 years) patients with NVAF,12
based on the results of a previous study of secondary stroke prevention in NVAF patients.13
Information regarding the status and effects of anticoagulation therapy among the elderly population, however, is still limited.14
Therefore, we investigated the status of anti-thrombotic therapy, rates of ischemic and hemorrhagic events, and mortality among different age groups of NVAF patients via a post-hoc analysis of the J-RHYTHM Registry.15–17
Results of the present study should be interpreted with caution, because the data of this registry were derived from institutions that specialized in cardiology and in the management for cardiac arrhythmias. These results may not always reflect situations in a general Japanese population with NFAF.
Methods
Study Design of the J-RHYTHM Registry
The J-RHYTHM Registry was a prospective, observational nationwide study, the detailed design and baseline characteristics of which have been reported elsewhere.15,16
Briefly, the subjects were recruited from 158 institutions that specialized in cardiology. A consecutive series of outpatients with AF of any type was enrolled, regardless of the use of anti-thrombotic drugs. Anti-thrombotic drugs and dosages were selected at the discretion of the treating cardiologists. Patients with valvular AF18
were excluded from this subanalysis.
Follow-up and Definition of Endpoints
The patients were followed for 2 years or until an endpoint, whichever occurred first. The thromboembolic endpoints consisted of symptomatic ischemic stroke, transient ischemic attack (TIA), and systemic embolism. Major hemorrhage, including intracranial hemorrhage, gastrointestinal hemorrhage, and other hemorrhage requiring hospitalization, was selected as the safety endpoint. All-cause mortality and cardiovascular mortality were also determined. If any event occurred during the follow-up period, the final clinical data, including INR at the time closest to the event, were collected.15
The diagnostic criteria for each event have been described elsewhere.15,16
Age Group and INR
Patients were divided into 3 different age groups (<70, 70–84, and ≥85 years). The cut-off age of 70 years was selected according to that of the age-specific target INR in the Japanese guidelines.12
Although the cut-off age of 80 years was used in some previous studies,19,20
the highest cut-off age was arbitrarily set at 85 years in the present study, given that little information was available concerning anticoagulation status and events in very old NVAF patients aged ≥85 years.14
Consequently, the oldest group consisted of 330 NVAF patients aged ≥85 years (Table 1). The cut-off ages of 65 and 75 years were also considered as the alternative age groups according to the age criteria in the CHADS2
(1 point each for the presence of congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, and 2 points for history of stroke or TIA)21
and CHA2DS2-VASc scores (2 points for age ≥75 years and additionally 1 point each for the presence of vascular disease, age 65–74 years, and female sex category).22
In addition, patients receiving warfarin were divided into 5 subgroups according to INR (<1.6, 1.6–1.99, 2.0–2.59, 2.6–2.99, and ≥3.0). Although baseline INR was used in the main analysis of the J-RHYTHM Registry,17
INR at the time of events or at the end of the follow-up period was used in the present post-hoc analysis, because INR at the time of enrollment would not always reflect the anticoagulation status at the time of events.23
The time in therapeutic range (TTR)24
was also determined, using the target INR of 1.6–2.6 for patients aged ≥70 years and 2.0–3.0 for patients aged <70 years according to the Japanese guidelines.12
Table 1.
Baseline Patient Characteristics
| |
Overall |
<70 years |
70–84 years |
≥85 years |
P-value† |
| No. patients |
7,406 |
3,365 |
3,711 |
330 |
|
| Age (years) |
69.8±10.0 |
61.0±7.0 |
76.1±4.0 |
87.4±2.8 |
<0.001 |
| Male |
5,241 (70.8) |
2,648 (78.7) |
2,406 (64.8) |
187 (56.7) |
<0.001 |
| Type of AF |
| Paroxysmal |
2,835 (38.3) |
1,414 (42.0) |
1,326 (35.7) |
95 (28.8) |
<0.001 |
| Persistent |
1,081 (14.6) |
543 (16.1) |
496 (13.4) |
42 (12.7) |
| Permanent |
3,490 (47.1) |
1,408 (41.8) |
1,889 (50.9) |
193 (58.5) |
| Comorbidities |
| CAD |
781 (10.5) |
254 (7.5) |
483 (13.0) |
44 (13.3) |
<0.001 |
| Cardiomyopathy |
634 (8.6) |
361 (10.7) |
254 (6.8) |
19 (5.8) |
<0.001 |
| HCM |
264 (3.6) |
133 (4.0) |
123 (3.3) |
8 (2.4) |
0.249 |
| DCM |
370 (5.0) |
228 (6.8) |
131 (3.5) |
11 (3.3) |
<0.001 |
| CHD |
96 (1.3) |
66 (2.0) |
30 (0.8) |
0 (0.0) |
<0.001 |
| COPD |
131 (1.8) |
30 (0.9) |
89 (2.4) |
12 (3.6) |
<0.001 |
| Hyperthyroidism |
131 (1.8) |
82 (2.4) |
48 (1.3) |
1 (0.3) |
<0.001 |
| CHADS2 score |
| 0 |
1,157 (15.6) |
895 (26.6) |
262 (7.2) |
0 (0.0) |
<0.001 |
| 1 |
2,512 (33.9) |
1,451 (43.1) |
1,023 (27.6) |
38 (11.5) |
| 2 |
2,056 (27.8) |
676 (20.1) |
1,246 (33.6) |
134 (40.6) |
| 3 |
1,059 (14.3) |
262 (7.8) |
717 (19.3) |
80 (24.2) |
| 4 |
436 (5.9) |
62 (1.8) |
328 (8.8) |
46 (13.9) |
| 5 |
161 (2.2) |
19 (0.6) |
117 (3.2) |
25 (7.6) |
| 6 |
25 (0.3) |
0 (0.0) |
18 (0.5) |
7 (2.1) |
| Mean |
1.7±1.2 |
1.2±1.0 |
2.0±1.2 |
2.7±1.2 |
<0.001 |
| Risk factors for stroke |
| Heart failure |
2,055 (27.7) |
779 (23.2) |
1,113 (30.0) |
163 (49.4) |
<0.001 |
| Hypertension |
4,477 (60.5) |
1,835 (54.5) |
2,434 (65.6) |
208 (63.0) |
<0.001 |
| Age (≥75 years) |
2,565 (34.6) |
0 (0.0) |
2,235 (60.2) |
330 (100) |
<0.001 |
| Diabetes mellitus |
1,359 (18.3) |
584 (17.4) |
711 (19.2) |
64 (19.4) |
0.130 |
| Stroke/TIA |
1,022 (13.8) |
367 (10.9) |
589 (15.9) |
66 (20.0) |
<0.001 |
| Heart rate (beats/min) |
72.5±13.2 |
72.5±13.5 |
72.3±12.9 |
74.3±13.3 |
0.031 |
| Systolic BP (mmHg) |
126.0±16.2 |
125.1±15.8 |
126.8±16.3 |
125.4±18.1 |
<0.001 |
| Diastolic BP (mmHg) |
73.5±17.0 |
75.5±21.8 |
72.2±11.0 |
68.2±12.1 |
<0.001 |
Data given as n (%) or mean±SD. †Comparison among 3 age groups. AF, atrial fibrillation; BP, blood pressure; CAD, coronary artery disease; CHADS2, congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, and history of stroke or TIA; CHD, congenital heart disease; COPD, chronic obstructive pulmonary disease; DCM, dilated cardiomyopathy; HCM, hypertrophic cardiomyopathy; TIA, transient ischemic attack.
Data are presented as mean±SD. The statistical significance of differences in the means was analyzed using Student’s t-test or ANOVA, as appropriate. Frequencies of parameters or events were compared using chi-squared test or Fisher’s exact test, as appropriate. P<0.05 was considere to be statistically significant. All statistical analysis was performed with SPSS version 15.0 (SPSS Inc, Chicago, IL, USA).
Results
Of the 7,937 patients with AF who had been enrolled in the J-RHYTHM Registry,16
421 patients were excluded because they had valvular AF.18
Of the remaining 7,516 patients with NVAF, 110 (1.5%) were lost to follow-up. Therefore, a total of 7,406 patients with NVAF was eligible for the present analysis.17
Baseline Characteristics and Anti-Thrombotic Therapy Status
The prevalence of female sex, permanent AF, hypertension, coronary artery disease, heart failure, and history of ischemic stroke/TIA, and consequently mean CHADS2
score, were higher in the older groups than in the youngest group (Table 1). The frequency of warfarin treatment was lower in the oldest group than in the other groups. Mean INR was similar among the 3 age groups receiving warfarin, but daily warfarin dosage was significantly smaller in older groups than in younger groups. The target INR of 1.6–2.612
was achieved in 57.8% of the oldest group, and the TTR for this target INR was 67.1% in this specific age group (Table 2). The frequency of antiplatelet therapy increased with age, and any antiplatelet drug was prescribed in 34.5% of patients aged ≥85 years (Table 2).
Table 2.
Anti-Thrombotic Therapy at Enrollment
| |
Overall |
<70 years |
70–84 years |
≥85 years |
P-value† |
| Warfarin |
6,404 (86.5) |
2,822 (83.9) |
3,319 (89.4) |
263 (79.7) |
<0.001 |
| Dosage (mg/day) |
2.9±1.2 |
3.2±1.2 |
2.6±1.1 |
2.2±0.8 |
<0.001 |
| INR |
1.91±0.49 |
1.91±0.50 |
1.90±0.49 |
1.88±0.52 |
0.512 |
| <1.6 |
1,670 (26.1) |
746 (26.4) |
838 (25.2) |
86 (32.7) |
0.027 |
| 1.6–1.99 |
2,348 (36.7) |
986 (34.9) |
1,270 (38.3) |
92 (35.0) |
| 2.0–2.59 |
1,854 (29.0) |
850 (30.1) |
944 (28.4) |
60 (22.8) |
| 2.6–2.99 |
363 (5.7) |
167 (5.9) |
181 (5.5) |
15 (5.7) |
| ≥3.0 |
169 (2.6) |
73 (2.6) |
86 (2.6) |
10 (3.8) |
| TTR (%)‡ |
59.3±29.2 (n=6,064) |
42.6±27.4 (n=2,691) |
73.0±22.9 (n=3,128) |
67.1±25.9 (n=245) |
<0.001 |
| Any antiplatelet |
1,937 (26.2) |
761 (22.6) |
1,062 (28.6) |
114 (34.5) |
<0.001 |
| Aspirin |
1,675 (22.6) |
687 (20.4) |
910 (24.5) |
78 (23.6) |
<0.001 |
| Others |
433 (5.8) |
128 (3.8) |
261 (7.0) |
44 (13.3) |
<0.001 |
| Warfarin+antiplatelet |
1,358 (18.3) |
477 (14.2) |
815 (22.0) |
66 (20.0) |
<0.001 |
Data given as n (%) or mean±SD. †Comparison among 3 age groups. ‡Target INR: 2.0–3.0 (<70 years) or 1.6–2.6 (≥70 years). INR, international normalized ratio; TTR, time in therapeutic range.
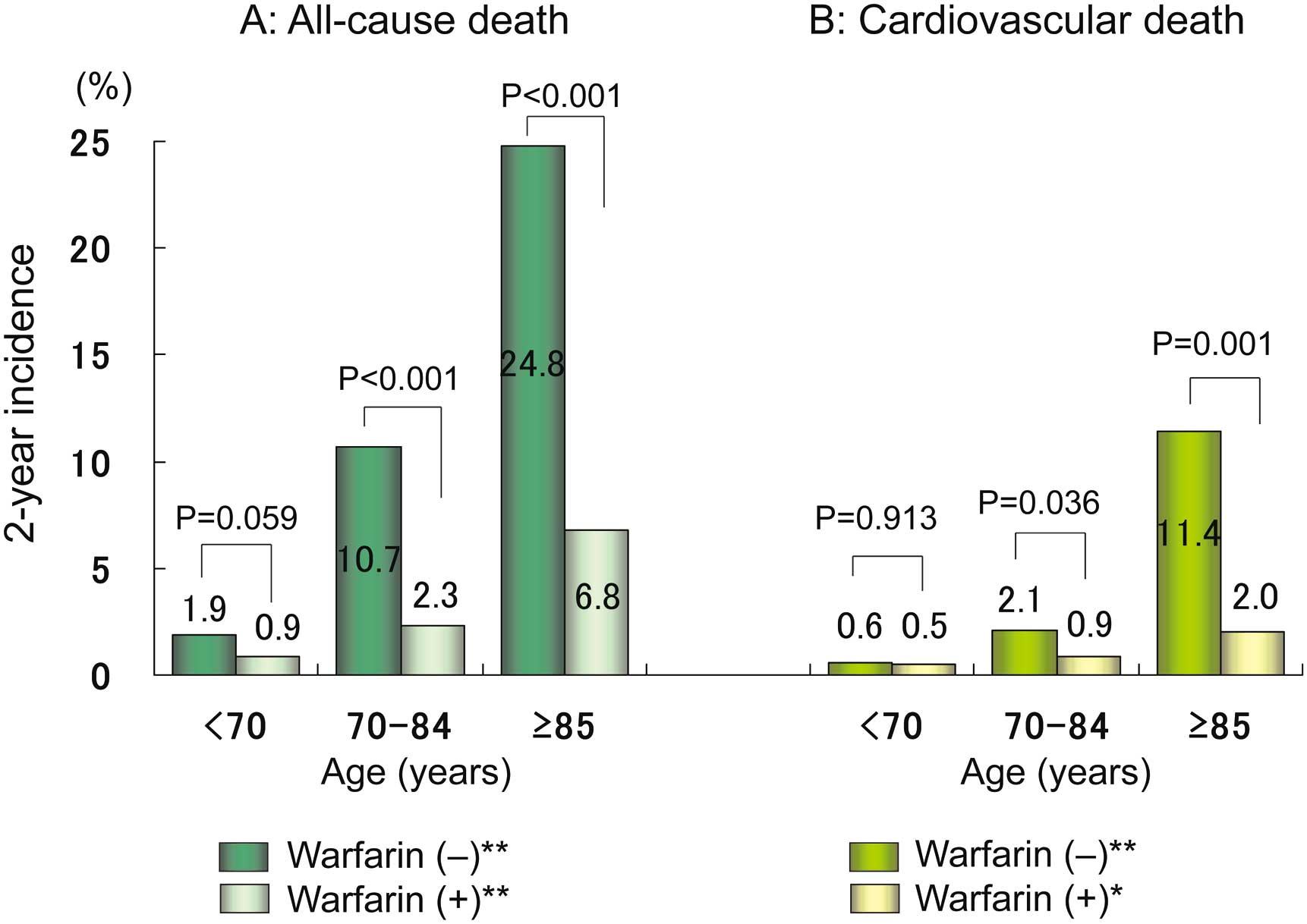
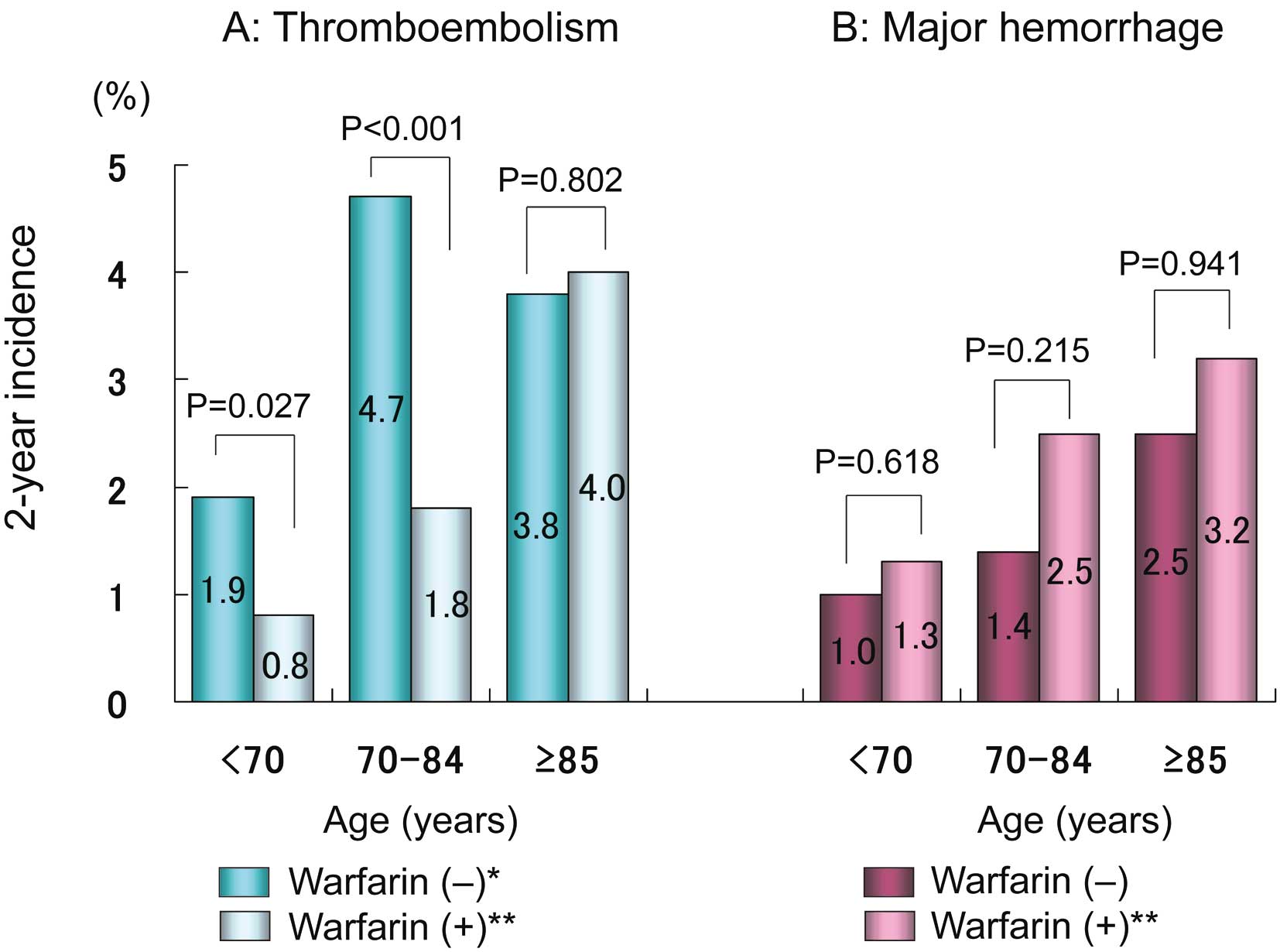
During the 2-year follow-up period, thromboembolic events occurred in 126 patients (1.7%), major hemorrhage in 140 (1.9%), and all-cause death in 195 (2.6%), including cardiovascular death in 68 (0.9%).
The incidence of thromboembolism increased with age (P<0.001 for trend) and was significantly lower in patients who were taking warfarin than in those who were not, in the groups aged <70 and 70–84 years (Figure 1A). Rate of major hemorrhage in patients taking warfarin also increased in an age-dependent manner (P<0.001 for trend) and looked to be higher compared with the non-warfarin group, but the difference did not reach statistical significance in all age groups (Figure 1B). All-cause mortality showed a remarkable age-dependent trend (P<0.001 for trend), and was markedly lower in the warfarin groups than in the non-warfarin groups aged ≥70 years (Figure 2A). Cardiovascular mortality was much higher among patients in the oldest group who were not taking warfarin compared with those in the same age group who were taking warfarin (Figure 2B).
Event rates in the alternative age groups are shown in
Figures S1,S2. Rate of thromboembolism was not significantly lower in patients who were taking warfarin than in those who were not, in the group aged <65 years (P=0.089;
Figure S1A).
Incidence Rates and INR
Rate of thromboembolic events decreased with an increase in INR in the groups aged <70 and 70–84 years, whereas it was higher at INR ≥2.6 in the oldest group aged ≥85 years (Table 3). Rate of major hemorrhage also showed a clear relationship with INR in all 3 age groups, and was much higher at INR ≥2.6 in the oldest patient group (Table 3). Consequently, the combined rates of thromboembolic and major hemorrhagic events were the lowest at INR 1.6–1.99 in groups aged 70–84 and ≥85 years (Table 3;
Figure 3). All-cause mortality was notably higher among patients in the groups aged 70–84 and ≥85 years who were not taking warfarin as well as among those in the warfarin group who had INR ≥3.0 (Table 3). Cardiovascular mortality showed a similar trend, especially in the oldest group (Table 3).
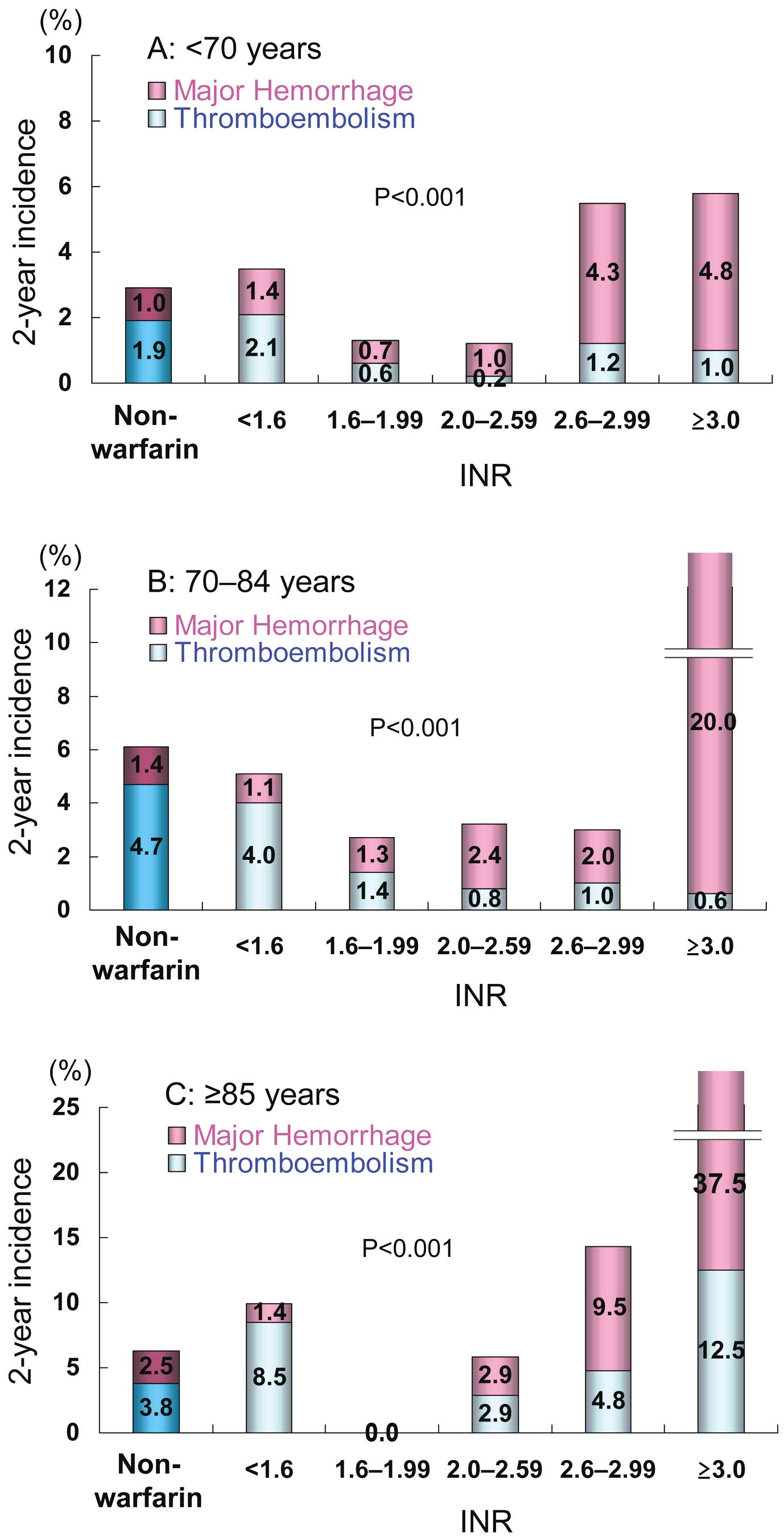
Table 3.
Two-Year Event Rates, Age, and Anticoagulation Intensity
| |
Non-warfarin |
Warfarin |
|
| INR† |
| No. patients |
|
<1.6 |
1.6–1.99 |
2.0–2.59 |
2.6–2.99 |
≥3.0 |
|
| <70 years |
619 |
571 |
974 |
926 |
161 |
105 |
|
| 70–84 years |
428 |
747 |
1,176 |
992 |
203 |
155 |
|
| ≥85 years |
79 |
71 |
81 |
69 |
21 |
8 |
|
| Thromboembolism |
|
|
|
|
|
|
P-value§ |
| <70 years |
12 (1.9) |
12 (2.1) |
6 (0.6) |
2 (0.2) |
2 (1.2) |
1 (1.0) |
0.001 |
| 70–84 years |
20 (4.7) |
30 (4.0) |
17 (1.4) |
8 (0.8) |
2 (1.0) |
1 (0.6) |
<0.001 |
| ≥85 years |
3 (3.8) |
6 (8.5) |
0 (0.0) |
2 (2.9) |
1 (4.8) |
1 (12.5) |
0.785 |
| P-value‡ |
0.032 |
0.004 |
0.229 |
0.008 |
0.530 |
0.242 |
|
| Major hemorrhage |
|
|
|
|
|
|
P-value§ |
| <70 years |
6 (1.0) |
8 (1.4) |
7 (0.7) |
9 (1.0) |
7 (4.3) |
5 (4.8) |
0.010 |
| 70–84 years |
6 (1.4) |
8 (1.1) |
15 (1.3) |
24 (2.4) |
4 (2.0) |
31 (20.0) |
<0.001 |
| ≥85 years |
2 (2.5) |
1 (1.4) |
0 (0.0) |
2 (2.9) |
2 (9.5) |
3 (37.5) |
0.002 |
| P-value‡ |
0.242 |
0.709 |
0.489 |
0.014 |
0.895 |
<0.001 |
|
| Thromboembolism+major hemorrhage |
|
|
|
|
|
|
P-value |
| <70 years |
18 (2.9) |
20 (3.5) |
15 (1.3) |
11 (1.2) |
9 (5.6) |
6 (5.7) |
<0.001 |
| 70–84 years |
26 (6.1) |
38 (5.1) |
32 (2.7) |
32 (3.2) |
6 (3.0) |
32 (20.6) |
<0.001 |
| ≥85 years |
5 (6.3) |
7 (9.9) |
0 (0.0) |
4 (5.8) |
3 (14.3) |
4 (50.0) |
<0.001 |
| P-value‡ |
0.014 |
0.022 |
0.177 |
<0.001 |
0.821 |
<0.001 |
|
| All-cause death |
|
|
|
|
|
|
P-value |
| <70 years |
12 (1.9) |
7 (1.2) |
6 (0.6) |
8 (0.9) |
3 (1.9) |
2 (1.9) |
0.163 |
| 70–84 years |
46 (10.7) |
19 (2.5) |
23 (2.0) |
13 (1.3) |
5 (2.5) |
14 (9.0) |
<0.001 |
| ≥85 years |
19 (24.1) |
3 (4.2) |
8 (9.9) |
5 (7.2) |
0 (0.0) |
1 (12.5) |
<0.001 |
| P-value‡ |
<0.001 |
0.036 |
<0.001 |
0.004 |
0.956 |
0.017 |
|
| Cardiovascular death |
|
|
|
|
|
|
P-value |
| <70 years |
4 (0.6) |
2 (0.4) |
3 (0.3) |
5 (0.5) |
2 (1.2) |
0 (0.0) |
0.240 |
| 70–84 years |
9 (2.1) |
9 (1.2) |
11 (0.9) |
4 (0.4) |
0 (0.0) |
5 (3.2) |
0.002 |
| ≥85 years |
9 (11.4) |
0 (0.0) |
2 (2.5) |
2 (2.9) |
0 (0.0) |
1 (12.5) |
0.006 |
| P-value‡ |
<0.001 |
0.307 |
0.015 |
0.347 |
0.122 |
0.207 |
|
Data given as n (%). †At the time of events or at the end of follow-up. ‡Comparison among the 3 age groups (χ2
test for trend). §Comparison among 6 groups (non-warfarin group and 5 INR subgroups) (χ2
test for trend). INR, international normalized ratio.
Event rates according to INR in the alternative age groups are listed in
Table S1. Similar trends were observed even in the alternative age groups.
Discussion
The major findings of the present study are as follows. First, very old patients aged ≥85 were characterized as a high-risk population, with a CHADS2
score of 2.7±1.2. Second, warfarin was prescribed in approximately 80% of patients aged ≥85 years, and the TTR, based on the Japanese target INR of 1.6–2.6,12
was 67.1% in these patients. This indicated that anticoagulation therapy was performed frequently in Japan, even in very old patients, and that the quality of warfarin therapy was high25
in these elderly patients. Third, the rates of thromboembolism, major hemorrhage, and mortality clearly increased with age. The efficacy of warfarin for preventing thromboembolism was evident in patients aged 65–84 years. Even in very old patients aged ≥85 years, the combined event rate of thromboembolism plus major hemorrhage remained lower at INR 1.6–2.59 than in those in the non-warfarin group. In addition, all-cause mortality was markedly lower in elderly patients receiving warfarin than in those without warfarin treatment.
Thromboembolic and Hemorrhagic Events in Elderly Patients
In the present study, the rates of thromboembolic events increased with age in both the warfarin group and the non-warfarin group. The incidence of thromboembolism was markedly reduced at INR ≥1.6, especially in the group aged 70–84 years. Although the rate of thromboembolism was similar between very old patients aged ≥85 years with and without warfarin, it remained lower at INR 1.6–2.59 as compared with the non-warfarin group. This indicates that warfarin could be effective at preventing thromboembolism at INR between 1.6 and 2.59, even in very old patients aged ≥85 years.
The Incidence of major hemorrhage also increased with age in both the warfarin and the non-warfarin group. The rate of major hemorrhage increased markedly, depending on INR, and was higher at INR ≥2.6, especially in patients aged ≥85 years. Therefore, INR needs to be controlled below 2.6 for preventing hemorrhagic complication in elderly patients, a finding that is consistent with a previous study.13
Another previous study in elderly Japanese patients with NVAF also reported similar results: the rate of major hemorrhage was not high (1.1%/patient-year) in elderly patients aged ≥80 years with INR 1.5–2.5 and TTR of 73.9%.26
Mortality and Warfarin
The present study also found that all-cause mortality clearly increased with age, as indicated by previous studies.27,28
The warfarin group had lower all-cause mortality in patients aged ≥70 years, as well as lower cardiovascular mortality in very old patients aged ≥85 years. All-cause mortality, however, was markedly higher at INR ≥3.0, especially in groups aged ≥70 years; therefore, INR should be controlled below 3.0 when warfarin is given to elderly patients aged ≥70 years. Optimal intensity of warfarin therapy could be beneficial for all-cause mortality even in very old patients with NVAF, although it should be kept in mind that elderly patients may have any comorbidity to avoid warfarin, such as malignant neoplasm, resulting in a higher mortality in elderly patients in the non-warfarin group.
Optimal Anticoagulation Intensity in Elderly NVAF Patients
The Birmingham Atrial Fibrillation Treatment of the Aged (BAFTA) study included 190 patients aged ≥85 years and compared the rates of thromboembolic and hemorrhagic events in NVAF patients aged ≥75 years between 488 patients treated with warfarin and 485 receiving aspirin.9
The annual risk of ischemic stroke was significantly lower in the warfarin group than in the aspirin group (0.8% vs. 2.5%, P=0.0004), whereas the risk of hemorrhagic events was similar between the groups.9
This finding supports the use of anticoagulants in NVAF patients aged ≥75 years, unless there are contraindications. Other studies have demonstrated that the bleeding risk of warfarin in elderly NVAF patients aged ≥80 years is acceptably low.20,26
These findings suggest that age itself should not be regarded as a contraindication to anticoagulation therapy. The present findings also indicate that warfarin therapy could reduce thromboembolism and all-cause death even in very old patients aged ≥85 years, without an increase in major hemorrhage, when INR is controlled within the age-specific target values of 1.6–2.59.
Anticoagulation Therapy in Younger NVAF Patients
The present study also provides information on anticoagulation therapy with warfarin in younger NVAF patients. Rate of thromboembolism was low even in patients not taking warfarin in the youngest age group. Although significant reduction in rate of thromboembolism was observed in the youngest group when patients were divided at 70 years, it was not significant when the cut-off age was set at 65 years. Anticoagulation therapy might be unnecessary for patients aged <65 years who have no other risk factor for ischemic stroke. In patients receiving warfarin, the combined rates of thromboembolism and major hemorrhage at INR 1.6–2.59 tended to be lower even in patients aged <65 years, but this was not statistically significant. Therefore, it would be difficult to conclude that INR 1.6–2.6 is optimal in patients aged <65 years from the present data.
Study Limitations
The present study had several limitations. First, it was performed in a single country and the registry was established only in 158 selected institutions in Japan. Given that most of the participating physicians specialized in cardiology, patient clinical background may not be able to be extrapolated to a general Japanese patient population with NVAF.29
Second, although this registry was large, analyzing a total of 7,406 patients with NVAF, the numbers of patients and those having events in each age group and in the INR subgroups were small. This might have reduced the statistical power of the present study. In particular, the number in the oldest group with INR ≥2.6 was small. Therefore, generalizing from the results of this specific subgroup to daily clinical practice should be done with great caution. Third, given that the study design was prospective but observational, the selection of anti-thrombotic drugs was not randomized. Warfarin and INR levels for individual patients were selected at the discretion of the participating physicians. Fourth, 1.5% of patients were lost to follow-up in the present study, which could have led to the underreporting of endpoints.
Conclusions
Anticoagulation therapy with warfarin was performed frequently even in very old Japanese patients with NVAF. Warfarin therapy could reduce thromboembolism and all-cause mortality without an increase in major hemorrhage, even in very old patients aged ≥85 years, if INR is kept between 1.6 and 2.59.
Acknowledgments
The current study was presented in part at ESC Congress 2014 (Barcelona, Spain, 30 August 2014). Investigators in the J-RHYTHM Registry are listed in references 15, 16, and 30. The J-RHYTHM registry was supported by a grant from the Japan Heart Foundation.
Disclosures
Co-authors have a potential conflict of interest: H.A. has received research funding from Boehringer Ingelheim, and remuneration from Bayer Healthcare, Boehringer Ingelheim, and Daiichi-Sankyo; H.I. has received research funding from Boehringer Ingelheim and Daiichi-Sankyo, and remuneration from Daiichi-Sankyo, Bayer Healthcare, and Boehringer Ingelheim; K.O. has received research funding from Boehringer Ingelheim and Daiichi-Sankyo, and remuneration from Boehringer Ingelheim, Bayer Healthcare, Daiichi-Sankyo, and Pfizer; T.Y. has received research funding from Boehringer Ingelheim and Daiichi-Sankyo, and remuneration from Boehringer Ingelheim, Daiichi-Sankyo, Bayer Healthcare, Pfizer, Bristol-Myers Squibb, and Eisai; H.O. has received lecture fees from Daiichi-Sankyo.
Supplementary Files
Supplementary File 1
Figure S1.
Two-year incidence of (A) thromboembolism and (B) major hemorrhage in alternative age groups.
Figure S2.
Two-year incidence of (A) all-cause death and (B) cardiovascular death in alternative age groups.
Table S1.
Two-year event rates, age, and anticoagulation intensity in alternative age groups
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-15-0621
References
- 1.
Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: The Framingham Study. Stroke 1991; 22: 983–988.
- 2.
Feinberg WM, Blackshear JL, Laupacis A, Kronmal R, Hart RG. Prevalence, age distribution, and gender of patients with atrial fibrillation: Analysis and implications. Arch Intern Med 1995; 155: 469–473.
- 3.
Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001; 285: 2370–2375.
- 4.
Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006; 114: 119–125.
- 5.
Ohsawa M, Okayama A, Sakata K, Kato K, Itai K, Onoda T, et al. Rapid increase in estimated number of persons with atrial fibrillation in Japan: An analysis from national surveys on cardiovascular diseases in 1980, 1990 and 2000. J Epidemiol 2005; 15: 194–196.
- 6.
Inoue H, Fujiki A, Origasa H, Ogawa S, Okumura K, Kubota I, et al. Prevalence of atrial fibrillation in the general population of Japan: An analysis based on periodic health examination. Int J Cardiol 2009; 137: 102–107.
- 7.
Yiin GS, Howard DP, Paul NL, Li L, Luengo-Fernandez R, Bull LM, et al. Age-specific incidence, outcome, cost, and projected future burden of atrial fibrillation-related embolic vascular events: A population-based study. Circulation 2014; 130: 1236–1244.
- 8.
Marinigh R, Lip GY, Fiotti N, Giansante C, Lane DA. Age as a risk factor for stroke in atrial fibrillation patients: Implications for thromboprophylaxis. J Am Coll Cardiol 2010; 56: 827–837.
- 9.
Mant J, Hobbs FD, Fletcher K, Roalfe A, Fitzmaurice D, Lip GY, et al. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): A randomised controlled trial. Lancet 2007; 370: 493–503.
- 10.
Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): Developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation 2006; 114: e257–e354, doi:10.1161/CIRCULATIONAHA.106.177292.
- 11.
Camm AJ, Lip GY, De Caterina R, Savelieva I, Atar D, Hohnloser SH, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: An update of the 2010 ESC Guidelines for the management of atrial fibrillation: Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J 2012; 33: 2719–2747.
- 12.
JCS Joint Working Group. Guidelines for pharmacotherapy of atrial fibrillation (JCS 2013): Digest version. Circ J 2014; 78: 1997–2021.
- 13.
Yasaka M, Minematsu K, Yamaguchi T. Optimal intensity of international normalized ratio in warfarin therapy for secondary prevention of stroke in patients with non-valvular atrial fibrillation. Intern Med 2001; 40: 1183–1188.
- 14.
Furusho H, Takamura M, Takata S, Sakagami S, Hirazawa M, Kato T, et al. Current status of anticoagulation therapy for elderly atrial fibrillation patients in Japan: From Hokuriku atrial fibrillation trial. Circ J 2008; 72: 2058–2061.
- 15.
Atarashi H, Inoue H, Okumura K, Yamashita T, Origasa H. Investigation of optimal anticoagulation strategy for stroke prevention in Japanese patients with atrial fibrillation: The J-RHYTHM Registry study design. J Cardiol 2011; 57: 95–99.
- 16.
Atarashi H, Inoue H, Okumura K, Yamashita T, Kumagai N, Origasa H. Present status of anticoagulation treatment in Japanese patients with atrial fibrillation: A report from the J-RHYTHM Registry. Circ J 2011; 75: 1328–1333.
- 17.
Inoue H, Okumura K, Atarashi H, Yamashita T, Origasa H, Kumagai N, et al. Target international normalized ratio values for preventing thromboembolic and hemorrhagic events in Japanese patients with non-valvular atrial fibrillation: Results of the J-RHYTHM Registry. Circ J 2013; 77: 2264–2270.
- 18.
Kodani E, Atarashi H, Inoue H, Okumura K, Yamashita T. Target intensity of anticoagulation with warfarin in Japanese patients with valvular atrial fibrillation: Subanalysis of the J-RHYTHM Registry. Circ J 2015; 79: 325–330.
- 19.
Hylek EM, Evans-Molina C, Shea C, Henault LE, Regan S. Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation 2007; 115: 2689–2696.
- 20.
Poli D, Antonucci E, Grifoni E, Abbate R, Gensini GF, Prisco D. Bleeding risk during oral anticoagulation in atrial fibrillation patients older than 80 years. J Am Coll Cardiol 2009; 54: 999–1002.
- 21.
Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: Results from the National Registry of Atrial Fibrillation. JAMA 2001; 285: 2864–2870.
- 22.
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010; 137: 263–272.
- 23.
Inoue H, Nozawa T, Hirai T, Iwasa A, Okumura K, Lee JD, et al. Accumulation of risk factors increases risk of thromboembolic events in patients with nonvalvular atrial fibrillation. Circ J 2006; 70: 651–656.
- 24.
Rosendaal FR, Cannegieter SC, van der Meer FJ, Briet E. A method to determine the optimal intensity of oral anticoagulant therapy. Thromb Haemost 1993; 69: 236–239.
- 25.
Connolly SJ, Pogue J, Eikelboom J, Flaker G, Commerford P, Franzosi MG, et al. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation 2008; 118: 2029–2037.
- 26.
Naganuma M, Shiga T, Sato K, Murasaki K, Hashiguchi M, Mochizuki M, et al. Clinical outcome in Japanese elderly patients with non-valvular atrial fibrillation taking warfarin: A single-center observational study. Thromb Res 2012; 130: 21–26.
- 27.
Gorin L, Fauchier L, Nonin E, Charbonnier B, Babuty D, Lip GY. Prognosis and guideline-adherent anti-thrombotic treatment in patients with atrial fibrillation and atrial flutter: Implications of undertreatment and overtreatment in real-life clinical practice; the Loire Valley Atrial Fibrillation Project. Chest 2011; 140: 911–917.
- 28.
Halvorsen S, Atar D, Yang H, De Caterina R, Erol C, Garcia D, et al. Efficacy and safety of apixaban compared with warfarin according to age for stroke prevention in atrial fibrillation: Observations from the ARISTOTLE trial. Eur Heart J 2014; 35: 1864–1872.
- 29.
Akao M, Chun YH, Esato M, Abe M, Tsuji H, Wada H, et al. Inappropriate use of oral anticoagulants for patients with atrial fibrillation. Circ J 2014; 78: 2166–2172.
- 30.
J-RHYTHM Registry Investigators. Determinants of warfarin use and international normalized ratio levels in atrial fibrillation patients in Japan: Subanalysis of the J-RHYTHM Registry. Circ J 2011; 75: 2357–2362.