Abstract
Background:
This study aimed to clarify the incidence of takotsubo syndrome (TTS) after the Great East Japan earthquake (GEJ-E) between inland and coastal areas.
Methods and Results:
Consecutive hospitalized patients with TTS were registered between 2009 and 2016 in Iwate Prefecture. Patients were divided into 2 groups, by whether they lived inland or in the coastal area (both max. seismic intensity, 6−). The incidence of TTS was calculated using the standardized incidence ratio (SIR) before and after the earthquake. The long-term prognosis of the 2 groups was compared by Kaplan-Meier analysis. A total of 112 patients with TTS were registered from the acute coronary syndrome records of each hospital (n=4,163); 9 patients with TTS were registered within 2 months of the earthquake. A significant monthly variation was observed in March and April 2011 compared with the other months (P=0.029). At 2 years after the earthquake, the SIR was significantly increased in the coastal area (P<0.01), but decreased after ≥3 years. There were no significant differences in the long-term prognosis between the 2 groups (P=0.20).
Conclusions:
The incidence of TTS was increased in the acute phase after the GEJ-E, particularly in the coastal area. The magnitude of the tsunami damage is presumed to be a factor in the increased incidence of TTS, even though the seismic intensity in both areas was comparable.
Takotsubo syndrome (TTS) is a disorder known to be triggered by several stresses.1–5
The stresses that have been associated with TTS can be primarily divided into 2 categories: physical stress or mental stress. Natural disasters can be a type of mental stress and are known to trigger the onset of TTS.6–8
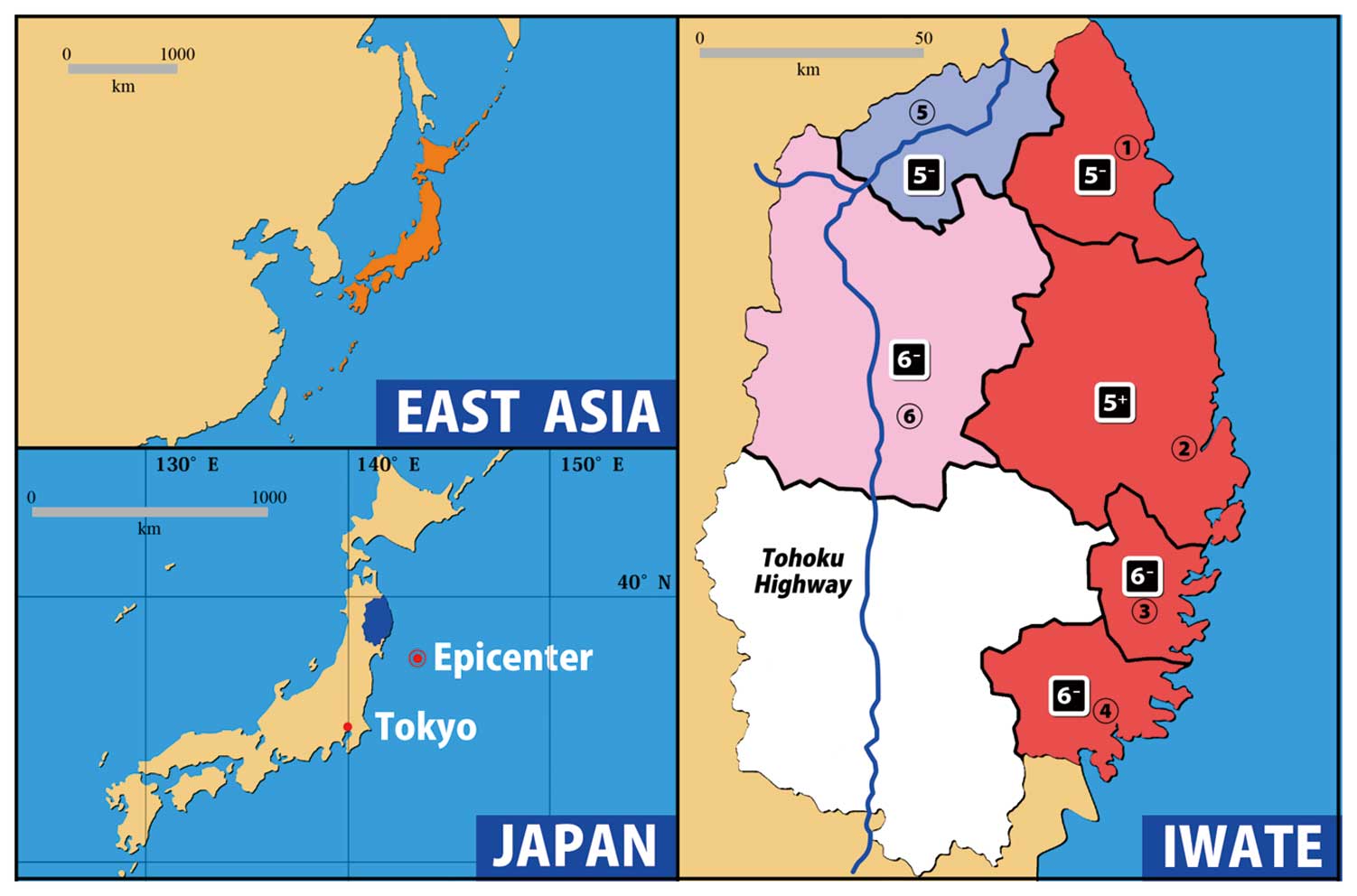
The Great East Japan earthquake (GEJ-E) disaster and massive tsunami, which occurred at 14:46 hours on March 11, 2011, was a magnitude 9.0 earthquake with an epicenter off the coast of Sanriku. The maximum seismic intensity of the earthquake was 7 in Kurihara, Miyagi Prefecture, and the tsunami reached up to ≥9.3 m in Soma, Miyagi Prefecture. A total of 19,630 people died, 2,569 were recorded as missing, 6,230 were injured, and 115,8976 homes were damaged on March 1, 2018. The earthquake has been reported as having a large impact on the development and treatment of various cardiovascular diseases.9–17
At first, the GEJ-E disaster was also thought to have increased the number of cases of TTS, but a short-term report from Miyagi Prefecture in 2013 indicated that there was no obvious increase.18
Even nearly 10 years after the disaster, people are still living in temporary housing, and there are concerns that the effects of the disaster may have led to chronic stress. A previous study reported that the incidence of acute heart failure was increased for a long time after the GEJ-E disaster.19
However, no studies have compared the incidence of TTS in coastal and inland areas and the long-term course of TTS after the GEJ-E disaster.
Editorial p ????
This study aimed to investigate (1) the incidence and long-term evolution of TTS in Iwate Prefecture before and after the GEJ-E disaster, and (2) compare its effect on the incidence and long-term prognosis of people living in inland and coastal areas.
Methods
Study Patients
Consecutive hospitalized TTS patients were registered between 2009 and 2016 at Iwate Medical University and its 5 associated hospitals (Figure 1): Memorial Heart Center, Iwate Medical University and Iwate Prefectural Ninohe, Kuji, Miyako, Kamaishi, and Ofunato hospitals. The over 40-year-old population in each of the target medical regions is shown in the
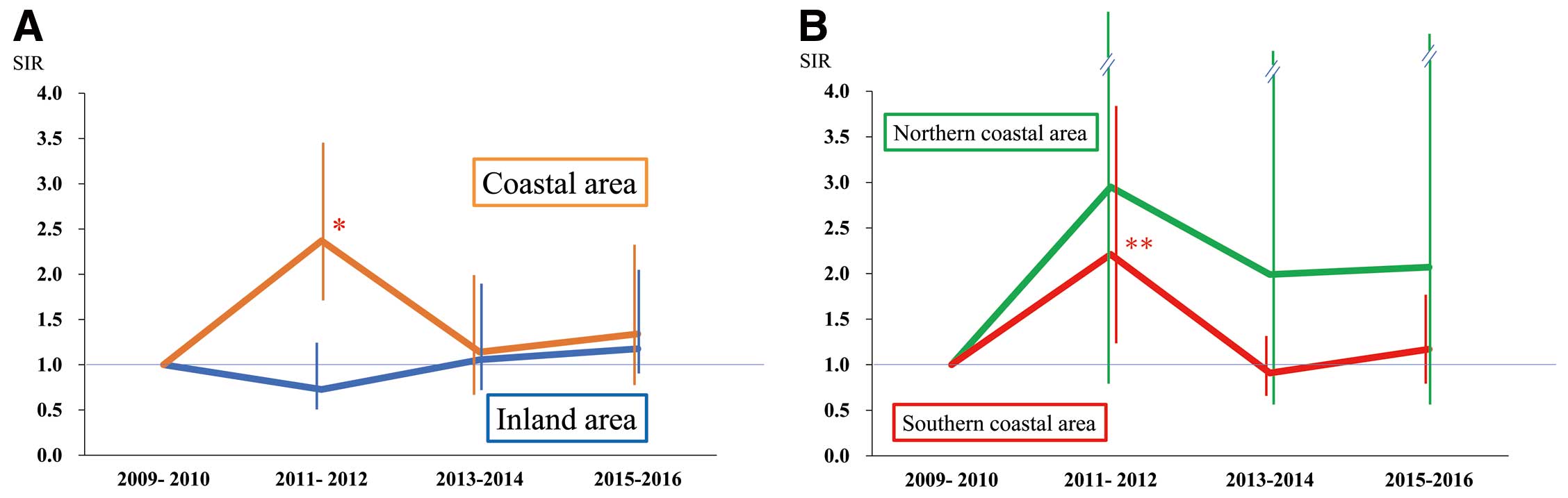
Supplementary Table. Patients were divided into groups by residence: inland (max. seismic intensity 6−) or coastal area (max. seismic intensity, 6−). Serial changes in the incidence of TTS between the 2 groups were calculated using the standardized incidence ratio (SIR) before and after the earthquake. Moreover, the coastal area was divided into the southern area where the tsunami damage was severe and the northern area where the damage was less severe (http://www.bousai.go.jp/kaigirep/chousakai/tohokukyokun/1/pdf/3-2.pdf). Specifically, the Miyako, Kamaishi, and Ofunato medical districts were defined as the southern area, and the Kuji medical district was defined as the northern area. On that basis, SIRs were compared between the 2 coastal subgroups. Moreover, the long-term prognosis of both groups was compared using a Kaplan-Meier analysis.
The Mayo clinic definition of TTS was used in this study,20
as follows. (1) Acute cardiac lesion with chest pain or dyspnea. (2) No coronary artery stenosis lesion considered to be an acute coronary syndrome but not consistent with abnormal wall motion. (3) New ST-T anomalies on ECG. (4) Acute left ventricular systolic abnormality with spontaneous recovery in ≈1 week with no or minimal elevation of myocardial deviation enzymes.
Statistical Analysis
The data are presented as the mean±standard deviation. Continuous values that were not normally distributed were compared between the coastal and inland areas using a Mann-Whitney U test. The categorical data of the 2 groups were compared using a chi-square contingency test. A P value <0.05 was considered statistically significant. Statistical analyses were performed using the Statistical Package for the Social Sciences for Windows version 21.0 (IBM Corp., Chicago, IL, USA).
We examined the incidence of new-onset TTS in the study area from the year of the disaster (January 1, 2011) to the end of 2016 (December 31, 2016). The SIRs during the disaster year of 2011 and the post-disaster years from 2012 to 2016 were determined from the number of observed cases relative to the number of expected cases calculated by the age-adjusted incidence rates for the 2 years before the disaster (2009–2010).
Continuous variables are expressed as the mean±SD. The significance of the temporal data from the predicate year to 2016 was analyzed using a one-way analysis of variance or Cochran-Armitage test.
Results
Outline of All TTS Patients in Iwate Prefecture
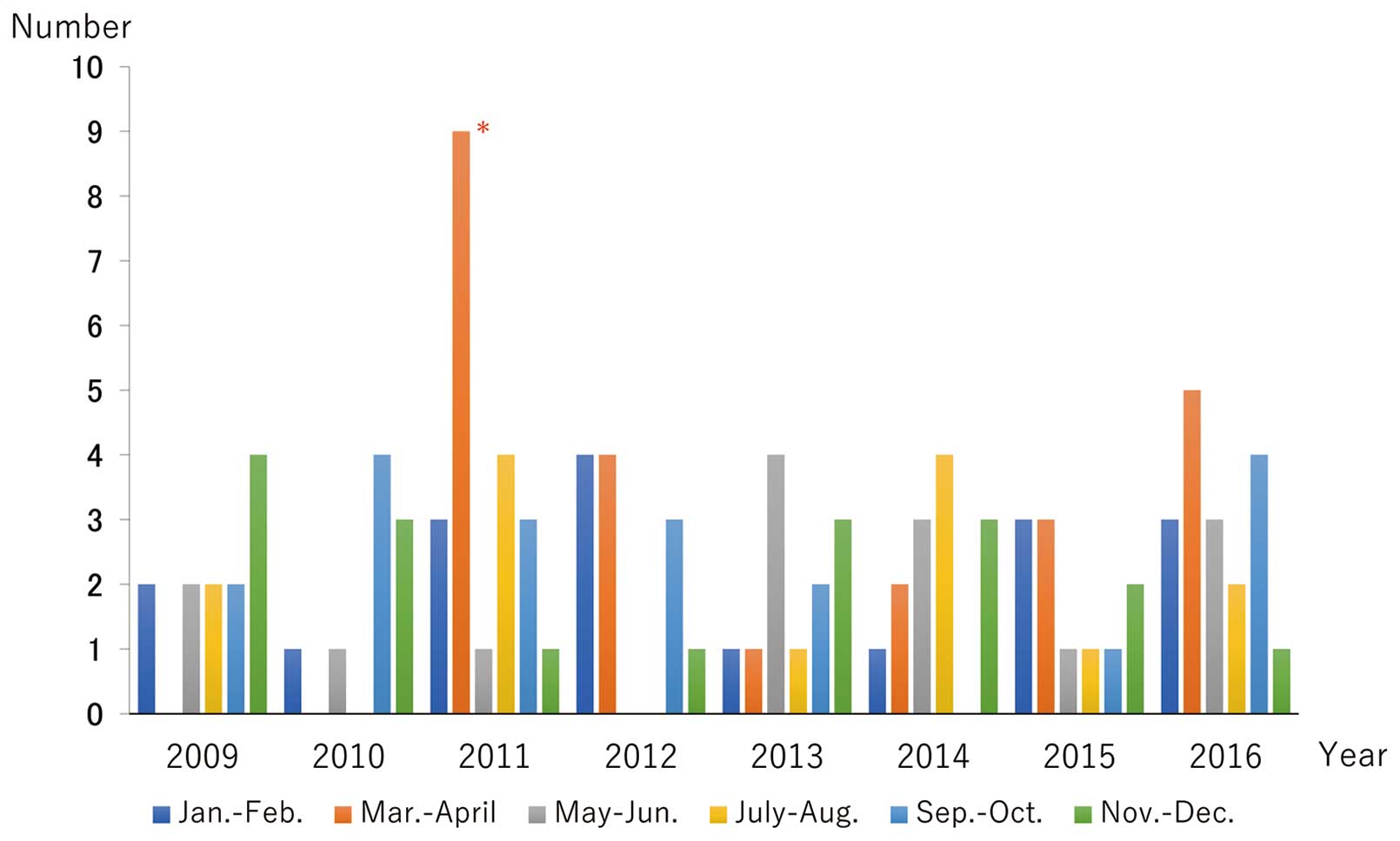
A total of 112 patients with TTS (male, 25; female, 87) were found in the acute coronary syndrome records of the included hospitals (n=4,163). The baseline clinical characteristics of the patients are shown in
Table. The average age was 75.3 years; 9 patients were diagnosed with TTS within 2 months of the earthquake (March and April). A significant monthly variation in March and April 2011 was observed compared with other months (Figure 2; P=0.029).
Table.
Baseline Clinical Characteristics of the Patients Included in the Current Study
| |
All patients
(n=112) |
Costal area
(n=57) |
Inland area
(n=55) |
P value |
| Age (years) |
75.3±12.0 |
75.2±12.6 |
75.4±11.4 |
0.921 |
| Male/female |
25/87 |
13/44 |
12/43 |
0.900 |
| BMI (kg/cm2) |
21.9±3.7 |
21.6±3.4 |
22.1±4.0 |
0.501 |
| Hypertension (%) |
70 (62.5) |
37 (60.8) |
33 (66.7) |
0.420 |
| Dyslipidemia (%) |
31 (27.7) |
14 (24.6) |
17 (30.9) |
0.651 |
| Diabetes mellitus (%) |
24 (21.4) |
13 (22.8) |
11 (20) |
0.681 |
| Smoking (%) |
8 (7.1) |
2 (3.5) |
6 (10.9) |
0.280 |
| Mental stress (%) |
33 (29.5) |
11 (19.3) |
21 (38.1) |
0.061 |
| Physical stress (%) |
41 (36.6) |
23 (40.4) |
18 (32.7) |
0.212 |
| SBP (mmHg) |
141.1±30.4 |
137.4±33.5 |
143.6±28.5 |
0.358 |
| Body temperature (℃) |
36.3±1.6 |
36.6±1.0 |
36.1±1.9 |
0.198 |
| WBC (/μL) |
9,363±4,377 |
10,377±4,833 |
8,366±3,702 |
0.016 |
| Peak CK (IU/L) |
674±1,737 |
539±1,009 |
813±2,274 |
0.417 |
| CRP (mg/dL) |
3.7±7.3 |
2.4±5.3 |
4.9±8.8 |
0.094 |
| CRE (mg/dL) |
0.87±0.78 |
0.99±0.76 |
0.74±0.79 |
0.097 |
| Templen classification |
| Apical type |
89 |
41 |
48 |
0.909 |
| Midventricular type |
3 |
1 |
2 |
|
| Basal type |
2 |
1 |
1 |
|
| Focal type |
7 |
4 |
3 |
|
| LVEF (TTE) (%) |
45.0±12.3 |
43.9±12.6 |
45.9±12.0 |
0.155 |
| In-hospital death (%) |
8 (7.1) |
6 (10.5) |
2 (3.6) |
0.160 |
11 patients did not have a Templen classification. BMI, body mass index; CK, creatinine kinase; CPR, C-reactive protein; CRE, creatinine; LVEF, left ventricular ejection fraction; SBP, systolic blood pressure; TTE, transthoracic echocardiography; WBC, white blood cell.
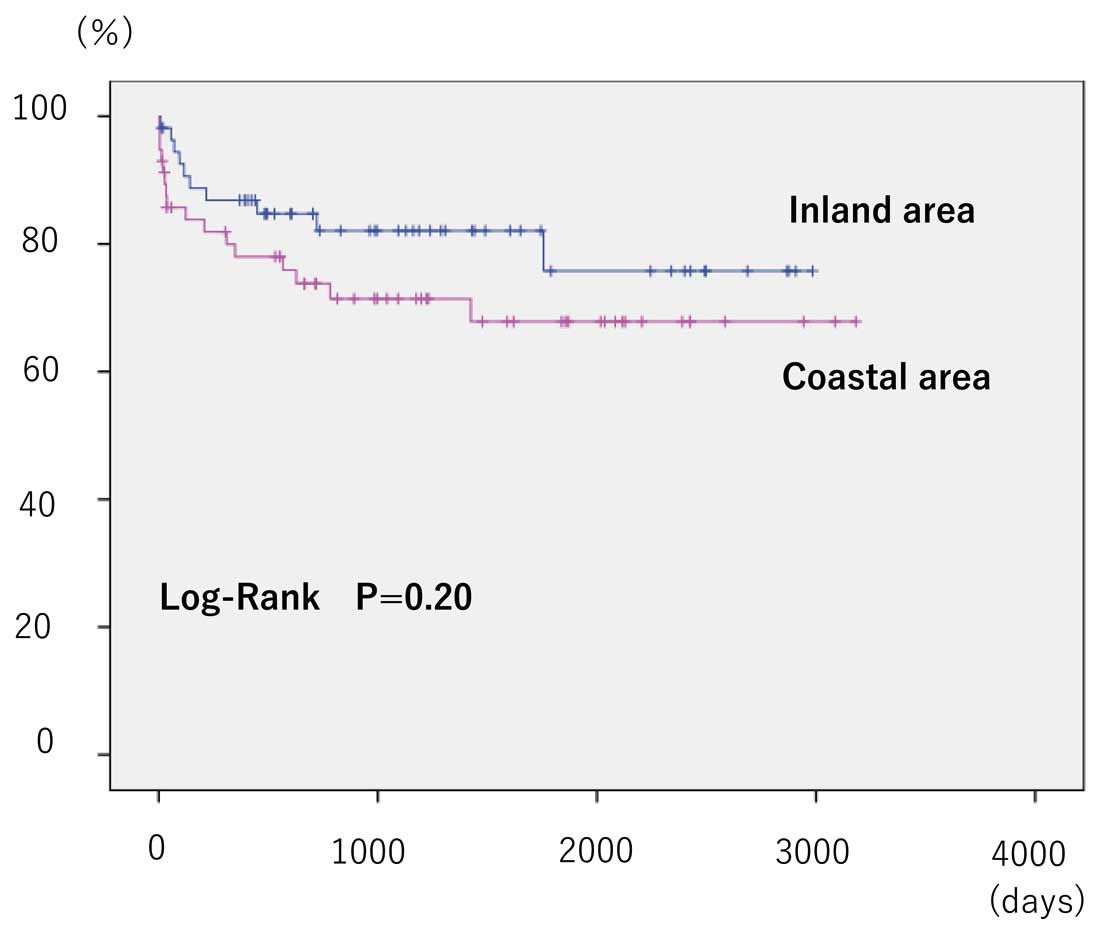
There were no significant differences in the baseline clinical characteristics of the 2 groups, except for white blood cell (Table). At 2 years after the earthquake, the SIR was significantly increased in the coastal area compared with the pre-earthquake period (2.37; 95% confidence interval (CI): 1.54–3.50; P<0.01). However, this decreased after ≥3 years (Figure 3A). In contrast, after 2 years, the SIR was not significantly increased in the inland area. Furthermore, the SIR after the GEJ-E in the northern coastal area showed no significant increase in the incidence of TTS compared with the pre-earthquake period, but the SIR in the southern coastal area showed a significant increase compared with the pre-earthquake period (Figure 3B). There were no significant differences between the 2 groups in the long-term prognosis (Figure 4; P=0.20).
Discussion
To the best of our knowledge, this is the first study to clarify the increased incidence of TTS after the GEJ-E disaster. The present study results can be summarized as follows. First, the GEJ-E disaster significantly increased the incidence of TTS in Iwate Prefecture, especially in March 2011, when the disaster occurred. Second, there was a significant increase for 2 years in the incidence of TTS based on the SIRs along the coast compared with the inland area. Finally, there was no significant difference between the 2 groups in the long-term prognosis.
Comparison With Previous Studies
Few studies have reported on a large number of cases of earthquake-related TTS.6,21
After the New Zealand earthquake, there were reports of an increase in the incidence of TTS.6,22
After the Niigata-Chuetsu earthquake, the monthly incidence of TTS was reported to have increased from 0.55 cases/month before the earthquake to 13 cases/month after the earthquake, a 24-fold increase.21
Regarding the GEJ-E disaster, Aoki et al reported the incidence of various acute cardiovascular diseases in the 15 weeks after the disaster.18
They reported that an increase was observed in heart failure, pulmonary thromboembolism, and infective endocarditis, but not in acute myocardial infarction or TTS. Further investigation of this is required because of their controversial finding.
Factors Affecting the Incidence of TTS After the GEJ-E Disaster
In the present study, there was a significant increase in the incidence of TTS in the coastal area compared with the inland area. Even though there was no difference between inland and coastal seismic intensity, there was an increase in the incidence of TTS in the coastal areas, which could be due to the magnitude of the tsunami damage. We speculate that the increased incidence of TTS was not only due to the intensity of the earthquake but also to the emotional and psychological stress caused by the loss of homes and family members, and living in temporary shelters. Although stresses such as power outages and food shortages occurred in the inland area, there were fewer collapsed houses (1,845 houses) and missing persons (5). On the other hand, in the coastal area there were extremely high levels of psychological stress from collapsed houses (24,232 houses) and loss of family members (4,672 dead and 1,117 missing). Interestingly, after the Niigata-Chuetsu earthquake, there was a high incidence of TTS on the northeast side near the epicenter, but almost no incidence on the southwest side of the epicenter. Although the earthquake shook the northeast and southwest sides to the same degree, the number of collapses was greater on the northeast side. Our data comparing the northern and southern coastal areas showed that the SIR was significantly increased in the latter, where tsunami damage was greater. It is likely that the degree of damage may be responsible for the increase in TTS incidence.
Differences in the Incidence of TTS and Other Acute Cardiac Diseases After the GEJ-E Disaster
In our long-term study of acute decompensated heart failure before and after the GEJ-E disaster, the SIR increased to 1.67 in 2011 in the area hardest hit by the tsunami. Although the SIR decreased temporarily to 1.25 in the year after the earthquake (2012), the 2013 and 2014 SIRs were 1.38 and 1.55, respectively, with a prolonged increase in the number of acute decompensated heart failure cases.19
Moreover, a similar trend was observed in patients with acute myocardial infarction.11
However, a different trend in the course of TTS was observed in this study. For acute heart failure and myocardial infarction, both direct acute and subsequent chronic factors may be involved in the development of cardiovascular disease after natural disasters. In other words, the direct effects of earthquakes, such as shaking and a tsunami, and environmental factors after a disaster, such as the subsequent reconstruction process, may influence the development of acute heart failure and myocardial infarction. On the other hand, TTS may be influenced by a few chronic indirect effects, but primarily by the acute direct effects of earthquakes, such as shaking or tsunami.
Study Limitations
First, we did not review the number of patients transported to hospitals south of central Iwate Prefecture with TTS. Nevertheless, we believe that the incidence of TTS on the coast is accurate, as we reviewed data from before and after the disaster. Second, this study was retrospective and only included a relatively small number of cases. A system that collects information from all prefectures in Japan is required so that the effect of natural disasters can be verified in the future. Third, it is unclear if the TTS patients in this study were directly damaged by the tsunami. There is a report of increased TTS after the Niigata-Chuetsu earthquake, but it has not been verified whether these patients were actually physically injured (such as by collapsing houses etc.) by the earthquake. Further studies are needed to clarify the relationship between direct damage and TTS occurrence. Finally, although we tried to determine the Templen classification by a central core laboratory in this study, that classification was not performed because coronary angiography and left ventriculography were discarded in some cases due to the retrospective nature of the study.
Conclusions
The incidence of TTS was increased in the acute phase after the GEJ-E, especially in the southern coastal area. The magnitude of the tsunami damage is presumed to be a factor that increased the incidence of TTS, even though the seismic intensity of each area was almost the same.
Acknowledgments
The authors are deeply grateful to the following: Fumiaki Takahashi, PhD (Medical Statistician, Iwate Medical University), Ms. Yumiko Okuyama (Research Nurse, Cardiovascular Research Center, Iwate Medical University), Ms. Kayoko Fujiwara (Secretary, Cardiovascular Research Center, Iwate Medical University), Tatsuya Shinke (Image Technician, Cardiovascular Research Center, Iwate Medical University), Tsubasa Sakaoto, MD, and Kenta Sasaki, MD (supplementary data collection, Ofunato Hospital).
Disclosures
Y. Morino, M.N. are members of
Circulation Journal’s Editorial Team.
IRB Information
Iwate Medial University approval no. H29-151. The first two authors contributed equally to this work.
Data Availability
The deidentified participant data will not be shared.
Supplementary Files
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-20-1044
References
- 1.
Ghadri JR, Wittstein IS, Prasad A, Sharkey S, Dote K, Akashi YJ, et al. International expert consensus document on takotsubo syndrome (Part I): Clinical characteristics, diagnostic criteria, and pathophysiology. Eur Heart J 2018; 39: 2032–2046.
- 2.
Ghadri JR, Ruschitzka F, Luscher TF, Templin C. Takotsubo cardiomyopathy: Still much more to learn. Heart 2014; 100: 1804–1812.
- 3.
Khalid N, Ahmad SA, Shlofmitz E, Chhabra L. Pathophysiology of takotsubo syndrome. In: StatPearls. Treasure Island (FL), 2020.
- 4.
Ghadri JR, Sarcon A, Diekmann J, Bataiosu DR, Cammann VL, Jurisic S, et al. Happy heart syndrome: Role of positive emotional stress in takotsubo syndrome. Eur Heart J 2016; 37: 2823–2829.
- 5.
Kato K, Lyon AR, Ghadri JR, Templin C. Takotsubo syndrome: Aetiology, presentation and treatment. Heart 2017; 103: 1461–1469.
- 6.
Chan C, Elliott J, Troughton R, Frampton C, Smyth D, Crozier I, et al. Acute myocardial infarction and stress cardiomyopathy following the Christchurch earthquakes. PLoS One 2013; 8: e68504.
- 7.
Pannarale G, Torromeo C, Acconcia MC, Moretti A, De Angelis V, Tanzilli A, et al. Two cases of acute chest discomfort and the Central Italy earthquake. Oxf Med Case Reports 2017; 2017: omx005.
- 8.
Modena MG, Pettorelli D, Lauria G, Giubertoni E, Mauro E, Martinotti V. Gender differences in post-traumatic stress. Biores Open Access 2017; 6: 7–14.
- 9.
Itoh T, Nakajima S, Tanaka F, Nishiyama O, Matsumoto T, Endo H, et al. Impact of the Japan earthquake disaster with massive Tsunami on emergency coronary intervention and in-hospital mortality in patients with acute ST-elevation myocardial infarction. Eur Heart J Acute Cardiovasc Care 2014; 3: 195–203.
- 10.
Niiyama M, Tanaka F, Nakajima S, Itoh T, Matsumoto T, Kawakami M, et al. Population-based incidence of sudden cardiac and unexpected death before and after the 2011 earthquake and tsunami in Iwate, northeast Japan. J Am Heart Assoc 2014; 3: e000798.
- 11.
Nakamura M, Tanaka K, Tanaka F, Matsuura Y, Komi R, Niiyama M, et al. Long-term effects of the 2011 Japan earthquake and tsunami on incidence of fatal and nonfatal myocardial infarction. Am J Cardiol 2017; 120: 352–358.
- 12.
Bazoukis G, Tse G, Naka KK, Kalfakakou V, Vlachos K, Saplaouras A, et al. Impact of major earthquakes on the incidence of acute coronary syndromes: A systematic review of the literature. Hellenic J Cardiol 2018; 59: 262–267.
- 13.
Tanaka F, Makita S, Ito T, Onoda T, Sakata K, Nakamura M. Relationship between the seismic scale of the 2011 northeast Japan earthquake and the incidence of acute myocardial infarction: A population-based study. Am Heart J 2015; 169: 861–869.
- 14.
Hao K, Takahashi J, Aoki T, Miyata S, Ito K, Sakata Y, et al. Factors influencing the occurrence of cardiopulmonary arrest in the Great East Japan Earthquake disaster. Int J Cardiol 2014; 177: 569–572.
- 15.
Hao K, Takahashi J, Ito K, Miyata S, Sakata Y, Nihei T, et al. Emergency care of acute myocardial infarction and the great East Japan earthquake disaster. Circ J 2014; 78: 634–643.
- 16.
Yamaki T, Nakazato K, Kijima M, Maruyama Y, Takeishi Y. Impact of the Great East Japan Earthquake on acute myocardial infarction in Fukushima prefecture. Disaster Med Public Health Prep 2014; 8: 212–219.
- 17.
Takegami M, Miyamoto Y, Yasuda S, Nakai M, Nishimura K, Ogawa H, et al. Comparison of cardiovascular mortality in the Great East Japan and the Great Hanshin-Awaji Earthquakes: A large-scale data analysis of death certificates. Circ J 2015; 79: 1000–1008.
- 18.
Aoki T, Takahashi J, Fukumoto Y, Yasuda S, Ito K, Miyata S, et al. Effect of the Great East Japan Earthquake on cardiovascular diseases: Report from the 10 hospitals in the disaster area. Circ J 2013; 77: 490–493.
- 19.
Nakamura M, Tanaka F, Komi R, Tanaka K, Onodera M, Kawakami M, et al. Sustained increase in the incidence of acute decompensated heart failure after the 2011 Japan earthquake and tsunami. Am J Cardiol 2016; 118: 1374–1379.
- 20.
Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): A mimic of acute myocardial infarction. Am Heart J 2008; 155: 408–417.
- 21.
Sato M, Fujita S, Saito A, Ikeda Y, Kitazawa H, Takahashi M, et al. Increased incidence of transient left ventricular apical ballooning (so-called ‘Takotsubo’ cardiomyopathy) after the mid-Niigata Prefecture earthquake. Circ J 2006; 70: 947–953.
- 22.
Watson GM, Chan CW, Belluscio L, Doudney K, Lacey CJ, Kennedy MA, et al. Comparing the variants of takotsubo syndrome: An observational study of the ECG and structural changes from a New Zealand tertiary hospital. BMJ Open 2019; 9: e025253.