Abstract
Background and Purpose: The concept of early chronic pancreatitis was proposed in Japan with the aim to improve the prognosis of patients with chronic pancreatitis. Endoscopic ultrasonography plays an important role in early diagnoses, but is limited by its invasiveness and poor objectivity. Hence, this study aimed to determine the usefulness of transabdominal ultrasound real-time tissue elastography as a screening method for early chronic pancreatitis.
Methods: We retrospectively examined 73 patients who underwent simultaneous ultrasound real-time tissue elastography and endoscopic ultrasonography from 2011 to 2014. The correlation between feature values (MEAN, %AREA, COMP) calculated by real-time tissue elastography and the Rosemont classification of endoscopic ultrasonography diagnostic criteria for chronic pancreatitis, and the diagnostic ability of ultrasound real-time tissue elastography to recognize “indeterminate for chronic pancreatitis” findings, which correspond to early chronic pancreatitis, were evaluated.
Main Results: Based on the Rosemont classification, 26 patients were “normal”, 16 were “indeterminate for chronic pancreatitis”, 13 were “suggestive of chronic pancreatitis”, and 18 were “consistent with chronic pancreatitis”. There were significant correlations between the feature values (MEAN, %AREA, COMP) and the Rosemont classification (p < 0.001; ρ = –0.788, 0.779, and 0.489, respectively). The area under the curve for the ability of MEAN to diagnose “indeterminate for chronic pancreatitis” was 0.889 (sensitivity, 93.8%; specificity, 76.9%).
Conclusions: The feature values calculated by ultrasound real-time tissue elastography were correlated with the Rosemont classification. Ultrasound real-time tissue elastography may be a useful screening method for early chronic pancreatitis.
INTRODUCTION
Chronic pancreatitis (CP) is an irreversible and progressive inflammatory disease in which chronic changes, such as irregular fibrosis and parenchymal destruction, develop within the pancreas. Disease progression causes persistent abdominal pain, digestive and absorptive disorders resulting from exocrine dysfunction, and diabetes mellitus due to endocrine dysfunction. As a result, the patients’ quality of life is greatly impaired2,23,28). It has also been reported that pancreatic cancer occurs frequently in patients with CP17,22,24,34). To improve the quality of life and prognosis of patients with CP, early diagnosis and therapeutic intervention are essential.
Diagnosis of CP focuses on imaging modalities, such as transabdominal ultrasonography (US), computed tomography, magnetic resonance imaging, and endoscopic retrograde cholangiopancreatography3,30,31). However, it is not easy to diagnose CP at an early stage, and several patients that are ultimately diagnosed using these imaging modalities tend to be in the advanced stages of the disease. In 2009, the Japan Pancreas Society proposed a new concept of early CP32) with the aim of improving the prognosis of patients through early medical intervention. In the diagnostic criteria of early CP, endoscopic ultrasonography (EUS) and endoscopic retrograde cholangiopancreatography are the diagnostic imaging modalities of choice. EUS provides high resolution and details of the pancreatic parenchyma and duct, which are not detectable by other imaging modalities. Therefore, the usefulness of EUS in the diagnosis of early stage CP has been recognized1,7,13). The EUS findings in early CP were chosen in consideration of the Rosemont classification, which itself is based on EUS-based criteria for the diagnosis of CP proposed in 20094). The Rosemont classification employs a combination of 11 EUS findings to classify the appearance as “consistent of CP”, “suggestive of CP”, “indeterminate for CP”, or “normal”. Early CP diagnostic criteria are based on the seven EUS findings characteristic of “indeterminate for CP” in the Rosemont classification.
Real-time tissue elastography (RTE) is an ultrasonography-based technology for determining tissue elasticity. RTE has already been clinically applied to the liver as a method for evaluating the degree of fibrosis26,33). In terms of the pancreas, the usefulness of EUS elastography has been mainly in the differential diagnosis of pancreatic lesions5,6,14,18,19,29). In addition, Itoh et al.15) reported the possibility of evaluating pancreatic fibrosis by EUS elastography, and Kuwahara et al.20) reported the usefulness of EUS elastography in the quantitative diagnosis of CP. Evaluation of the progression of CP by RTE may lead to early detection and medical intervention. If it is possible to determine the stage of CP with US, which is more convenient and less invasive than EUS, it can be a method to screen for early CP.
The aim of this study was to validate the usefulness of US-RTE as a diagnostic and screening method for early CP by evaluating the relationship between the Rosemont classification and parameters obtained by US-RTE.
MATERIALS AND METHODS
Patients
The retrospective study cohort consisted of 73 patients with pancreaticobiliary disease, who provided informed consent to undergo US-RTE and EUS simultaneously, from January 2011 to December 2014 at Hiroshima University Hospital. In this study, to avoid any confusion with obstructive pancreatitis caused by obstruction of the main pancreatic duct, patients with pancreatic neoplasms, such as pancreatic head cancer, intraductal papillary mucinous neoplasms, and ampullary carcinoma, were excluded. Based on the EUS findings, patients were classified as “normal”, “indeterminate for CP”, “suggestive of CP”, or “consistent with CP” based on the Rosemont classification. This study was approved by the Institutional Review Board of Hiroshima University Hospital (approval No. E-1194) and was conducted in compliance with the Declaration of Helsinki.
EUS procedure
EUS was performed using a 360° radial array electronic echoendoscope (GF-UE260-AL5; Olympus Medical Systems, Tokyo, Japan) with a diagnostic ultrasound system (ProsSound α10 or ProSound F75; Hitachi Aloka Medical, Ltd., Tokyo, Japan). The frequency and range of EUS were 7.5 MHz and 6–7.5 cm, respectively. Scanning was performed by gastroenterologists with at least eight years of clinical experience.
In all cases, the real-time images were stored in video format, and were assessed by three gastroenterologists for Rosemont classification. When there was a difference in opinion regarding the evaluation, the majority opinion was adopted.
US-RTE procedure
US was performed using HI VISION Ascendus (Hitachi Aloka Medical, Ltd.) with an EUP-L52 linear array probe (3.0–8.0 MHz; Hitachi Aloka Medical, Ltd.). Both the US and RTE were performed by three gastroenterologists with at least eight years of clinical experience. Patients assumed the dorsal position with both arms elevated and both legs outstretched. If the pancreas could not be visualized clearly, the patients were moved to a semi-sitting position. Scanning was performed by pressing the probe lightly against the epigastrium. Tissue elasticity images were generated using the deformation of the tissue by the abdominal aortic waves, not the pressure from the probe.
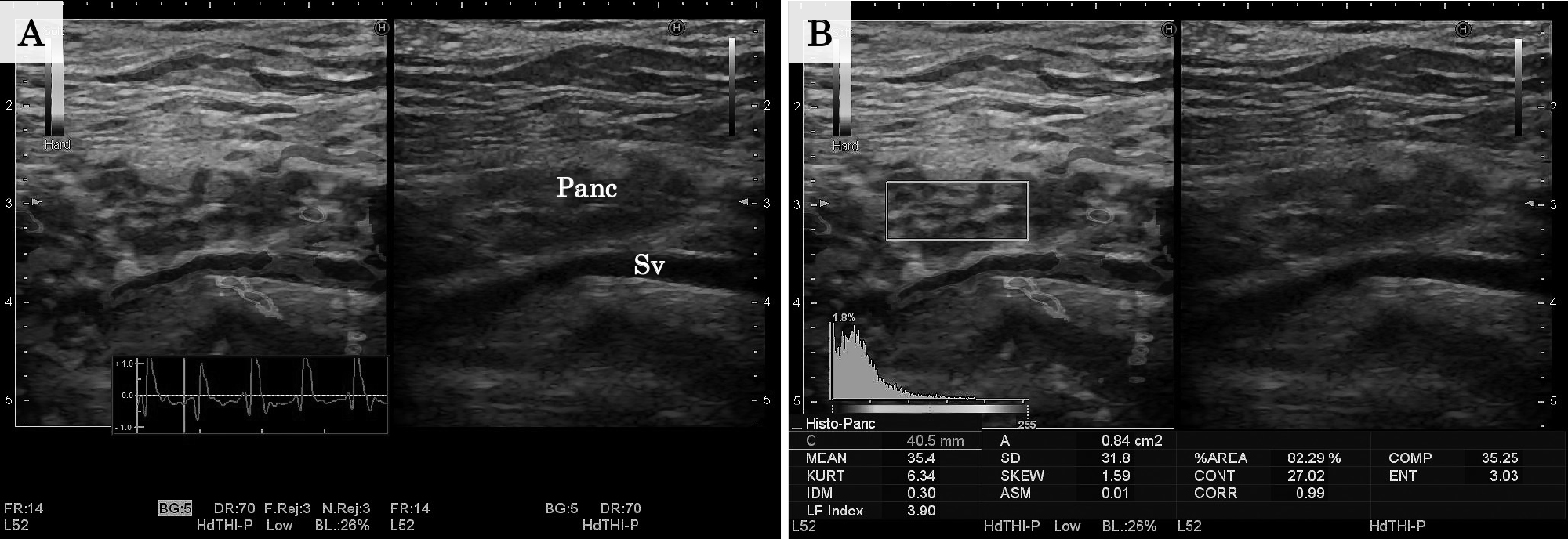
RTE was performed according to the following steps. First, the pancreas was visualized by transverse scanning of the epigastrium. Next, regions of interest were set to include the pancreas, splenic vein, and soft tissue in the peripancreatic area. The patients were asked to hold their breath, and we confirmed that tissue elasticity images had been obtained in accordance with the heartbeat. Pixel values were converted to color images within the range of zero (red) for minimum hardness to 255 (blue) for maximum hardness, which created a distribution histogram. Next, using the strain histogram measurement function, we calculated the parameters (feature values) in the pancreatic body (Figure 1). When setting the regions of interest, we avoided blood vessels and pancreatic ducts. Measurements were performed five times, and the mean values were used in the final analysis. Feature values calculated by strain histogram measurement function included the following 11 items: the mean relative strain values (MEAN), standard deviation of relative strain values, percentage of low-strain area (%AREA), complexity of the low-strain area (COMP), kurtosis of the histogram, skewness of the histogram, contrast, entropy, inverse difference moment, angular second moment, and correlation. Of these feature values, this study used the MEAN, %AREA, and COMP, which have been reported to correlate with liver fibrosis33).
Statistical analysis was performed using JMP 12.2.0 (SAS, Cary, NC, USA). Continuous variables were compared using the Wilcoxon rank sum test. The χ-squared test or Fisher’s exact test were performed for the comparison of proportions. The correlations between each feature value and the Rosemont classification were analyzed using Spearman’s rank correlation coefficient (r), where |r| ≤ 0.2 was defined as no correlation, |r| = 0.2–0.4 as a weak correlation, |r| = 0.4–0.7 as a moderate correlation, and |r| = 0.7–1.0 as a strong correlation. The ability of each feature value to diagnose CP according to the Rosemont classification was compared using receiver operating characteristic (ROC) analysis, where an area under the ROC curve (AUC) = 0.5–0.7 was defined as low accuracy, AUC = 0.7–0.9 as moderate accuracy, and AUC = 0.9–1.0 as high accuracy. The point at which the Youden index (sensitivity + specificity–1) became the maximum was used as the optimal cut-off value. Sensitivity and specificity at this point were also calculated. P-values < 0.05 were considered statistically significant.
RESULTS
Clinical characteristics of the patients
The clinical profiles of the patients are shown in Table 1. Based on the Rosemont classification, the 73 patients were classified as “normal” (n = 23), “indeterminate for CP” (n = 16), “suggestive of CP” (n = 13), and “consistent with CP” (n = 18). The clinical characteristics of the patients in each group are shown in Table 2. Compared to the “normal” group, the “indeterminate for CP” group had a significantly higher proportion of men, pancreatic enzyme level abnormality, continuous heavy drinking, and smoking (p = 0.032, 0.003, < 0.001, and 0.003, respectively). The rate of continuous heavy drinking, smoking and diabetes mellitus was significantly lower in patients “indeterminate for CP” than those “consistent with CP” (p = 0.009, 0.009 and 0.003, respectively). On the other hand, there was no significant difference in the clinical characteristics of patients “indeterminate for CP” and “suggestive of CP.”
Table 1
Clinical profiles of the 73 patients.
| Characteristics |
Values |
| Age (years) |
60 (22–87) |
| Sex (male to female) |
43:30 |
| Body mass index (kg/m2) |
20.8 (14.9–27.4) |
| Upper abdominal pain |
30 (41.1%) |
| Abnormal pancreatic enzymes level in the serum |
42 (57.5%) |
| Abnormal pancreatic exocrine function |
8/33 (24.2%) |
| Continuous heavy drinking (≥ 80 g/day of pure ethanol) |
29 (39.7%) |
| Smoking history |
31 (42.5%) |
| Diabetes |
13 (17.8%) |
| Underlying disease |
|
| Non-pancreatic disease |
13 (17.8%) |
| gallbladder polyp |
4 (5.5%) |
| others |
9 (12.3%) |
| Pancreatic disease |
60 (82.2%) |
| chronic pancreatitis |
43 (58.9%) |
| pancreatic cyst |
4 (5.5%) |
| others |
13 (17.8%) |
Data are expresses as number (percentage) or median (range).
Table 2
Clinical characteristics of the patients classified according to the Rosemont classification.
|
Normal
(n = 26) |
Indeterminate
(n = 16) |
Suggestive
(n = 13) |
Consistent
(n = 18) |
| Age (years) |
56 (34–84) |
66 (39–87) |
59 (22–74) |
61 (27–80) |
| Sex (male) |
9 (34.6%) |
11 (68.8%) |
7 (53.8%) |
16 (88.8%) |
| Body mass index (kg/m2) |
19.5 (14.9–25.6) |
21.1 (17.9–26.6) |
22.2 (16.3–25.2) |
19.8 (14.9–27.4) |
| Upper abdominal pain |
5 (19.2%) |
7 (43.8%) |
7 (53.8%) |
11 (61.1%) |
| Abnormal pancreatic enzymes level in the serum |
6 (23.1%) |
14 (87.5%) |
9 (69.2%) |
13 (72.2%) |
| Abnormal pancreatic exocrine function |
0/6 (0%) |
2/9 (22.2%) |
2/8 (25.0%) |
4/10 (40.0%) |
| Continuous heavy drinking (≥ 80 g/day of pure ethanol) |
0 (0%) |
7 (43.8%) |
6 (46.2%) |
16 (88.8%) |
| Smoking history |
1 (3.8%) |
7 (43.8%) |
7 (53.8%) |
16 (88.8%) |
| Diabetes |
2 (7.7%) |
0 (0%) |
3 (23.1%) |
8 (44.4%) |
Data are expresses as number (percentage) or median (range).
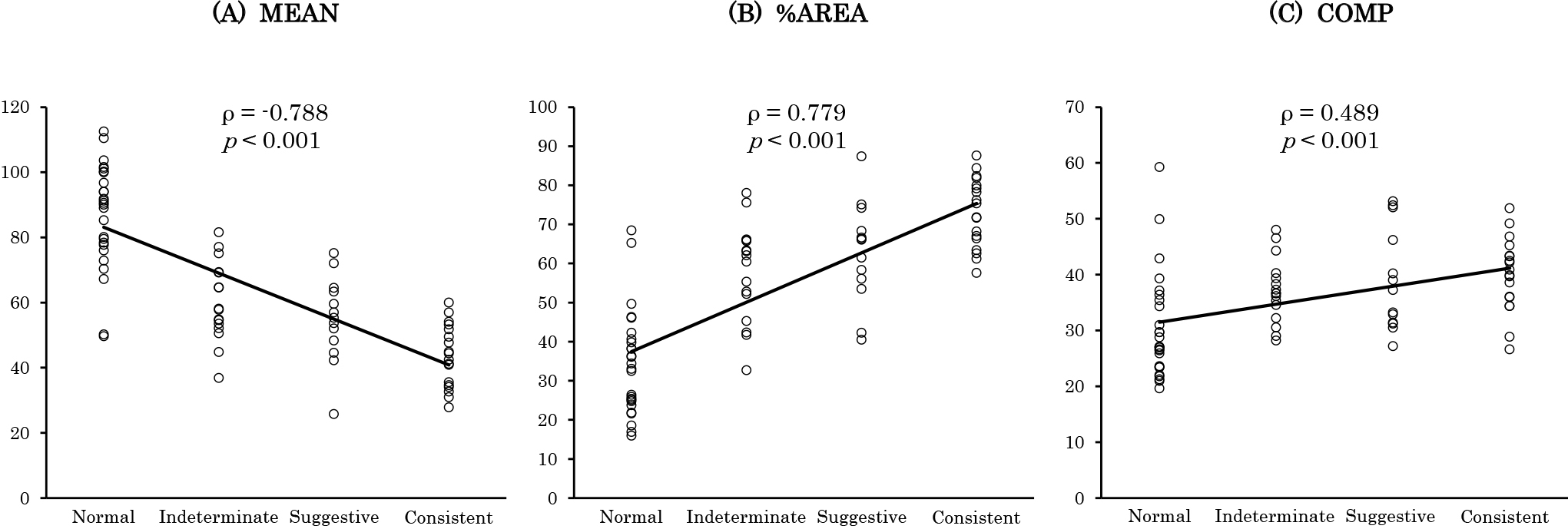
The three feature value findings according to the Rosemont classification and their correlation to the Rosemont classification are shown in Table 3 and Figure 2, respectively. The median MEAN decreased in the order of “normal”, “indeterminate for CP”, “suggestive of CP”, and “consistent with CP”, and there was a significant difference between “normal” and “indeterminate for CP”, and between “suggestive of CP” and “consistent with CP” (p < 0.001 and 0.012, respectively). The median %AREA and COMP increased in the order of “normal,” “indeterminate for CP,” “suggestive of CP,” and “consistent with CP.” There was a significant difference in %AREA between “normal” and “indeterminate for CP,” and between “suggestive of CP” and “consistent with CP” (p < 0.001 and 0.019, respectively). On the other hand, there was a significant difference in COMP only between “normal” and “indeterminate for CP” (p = 0.002). There were significant correlations between the three feature values and the Rosemont classification (p < 0.001 for all). A strong negative correlation was observed for MEAN (ρ = –0.788) while a strong positive correlation was observed for %AREA (ρ = 0.779) and a moderate positive correlation was observed for COMP (ρ = 0.489).
Table 3
Comparison of feature values by the Rosemont classification.
| Rosemont classification |
MEAN |
%AREA |
COMP |
| Normal |
90.3 (49.6–112.5) |
33.7 (15.9–68.5) |
27.0 (19.6–59.2) |
| Indeterminate |
57.9 (36.8–81.6) |
61.3 (32.7–78.0) |
36.6 (28.2–48.0) |
| Suggestive |
55.3 (25.8–75.1) |
66.1 (40.5–87.4) |
37.3 (27.2–53.1) |
| Consistent |
43.4 (27.8–60.0) |
73.6 (57.6–87.6) |
40.4 (26.6–51.9) |
Data are expresses as median (range).
CP indicates chronic pancreatitis.
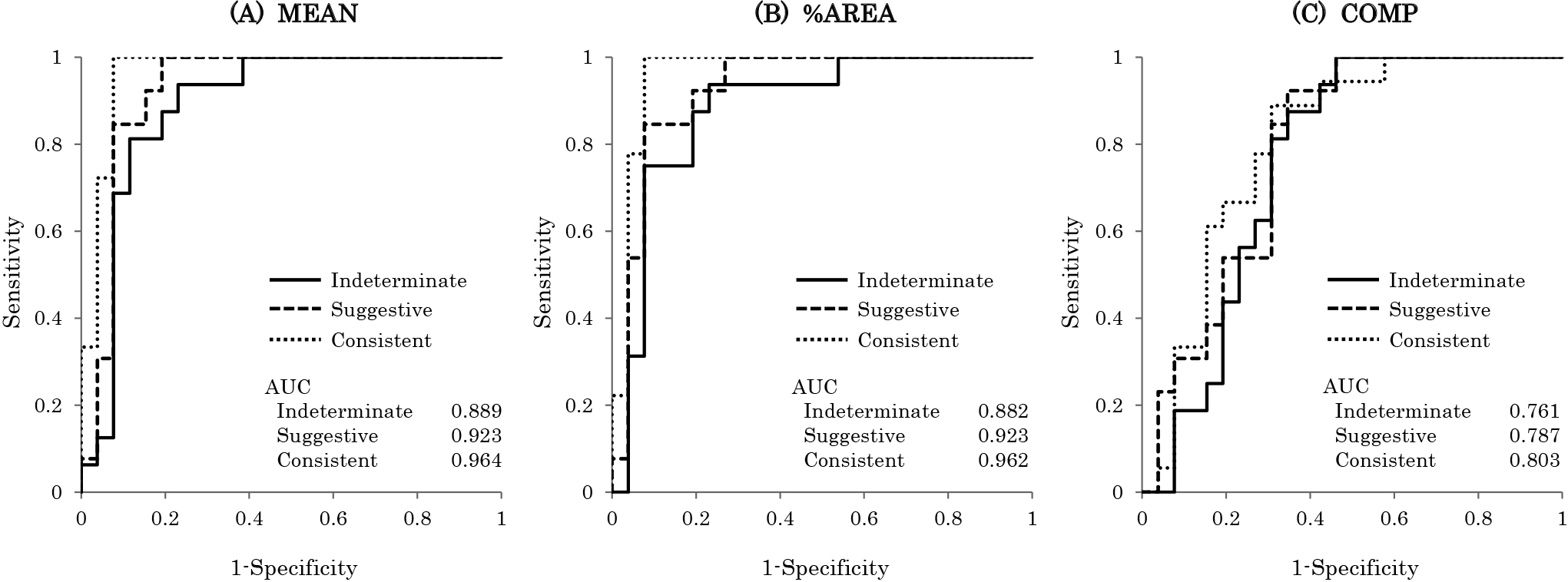
The ROC curves of the three feature values for the diagnosis of CP according to the Rosemont classification are shown in Figure 3. For the diagnosis of “indeterminate for CP,” the AUC was 0.889, 0.882, and 0.761 for MEAN, %AREA, and COMP, respectively. The optimal cut-off values with their corresponding sensitivity and specificity are summarized in Table 4. In the diagnosis of “indeterminate for CP,” the sensitivity was 93.8% and specificity was 76.9% when the cut-off MEAN value was set at 77.1.
Table 4
Cut-off values of MEAN with their corresponding sensitivity and specificity.
| Rosemont classification |
Optimal cut-off value |
Sensitivity (%) |
Specificity (%) |
| Indeterminate |
77.1 |
93.8 |
76.9 |
| Suggestive |
75.1 |
100.0 |
80.8 |
| Consistent |
60.0 |
100.0 |
92.3 |
CP indicates chronic pancreatitis.
DISCUSSION
This study demonstrated the usefulness of US-RTE as an objective and accurate tool for diagnosing CP according to the Rosemont classification. With regards to the Japan Pancreas Society diagnostic criteria32) and the European guidelines21), EUS plays a very important role in the imaging diagnosis of early CP. EUS provides excellent details of the pancreatic parenchyma and offers quantitative measures that are useful for staging the severity of structural changes, calcifications, and fibrosis. However, consistently reproducible image interpretation and interobserver agreement are poor16,36), and gold standard EUS findings for the diagnosis of early CP have not been established. In recent years, the usefulness of EUS elastography in the diagnosis of CP has been reported10,15,20), which can be a method of improving the objectivity of EUS findings. However, unlike other imaging modalities such as US, computed tomography, and magnetic resonance imaging, EUS is invasive and complications occur in about 0.3% of patients27), especially those with frequent cervical esophageal perforation9,11,27). Furthermore, EUS requires significant operator expertise and cannot be performed at all institutions. Therefore, EUS is not the initial imaging technique for diagnosing CP, and is not sufficient for screening for early CP.
In this study, we evaluated the usefulness of US-RTE as a screening method for early CP because of its noninvasive and convenient nature. There was a significant correlation between three feature values calculated with US-RTE and the diagnosis of CP according to the Rosemont classification. The MEAN value showed the highest correlation among the three feature values representing tissue elasticity. The elasticity of the pancreatic parenchyma decreased in the order of “normal”, “indeterminate for CP”, “suggestive of CP”, and “consistent with CP”. Similar results were reported in a previous EUS elastography study20). It has been reported that MEAN reflects the degree of liver fibrosis26,33), and although they used EUS elastography, Itoh et al.15) reported that MEAN had a significant correlation with the degree of pancreatic fibrosis. Some EUS findings of CP have no histopathological evidence4) and the correlation between the Rosemont classification and histopathological findings has not been elucidated35). However, the results of this study suggest that the four Rosemont classifications may correlate with the progression of fibrosis. The MEAN value of “indeterminate for CP” patients was significantly lower than those with a normal pancreas; therefore, “indeterminate for CP” is considered to be a state in which fibrosis has partially progressed.
In the ROC analysis, the diagnostic performance of “indeterminate for CP" showed a sensitivity of 93.8% and specificity of 76.9% when the cut-off MEAN value was set at 77.1. US is useful for diagnosis of advanced CP, but is limited for the diagnosis of early CP8,21). It is certainly difficult to detect minor findings of early CP by US, but US-RTE is sufficient for screening of early CP.
There has been no report on the opportunity for the diagnosis of early CP, but it is considered that early CP is often diagnosed by an examination of upper abdominal pain and abnormal pancreatic enzyme levels. According to a nationwide survey of early CP in Japan25), recurrent upper abdominal pain and abnormal pancreatic enzyme levels in the serum or urine were found in 91.4% and 81.5% of patients, respectively. For patients with these clinical signs and a history of continuous heavy drinking, imaging examination for suspicion of CP should be performed using minimally invasive US or computed tomography. The addition of US-RTE makes it possible to increase the number of patients who undergo examination by several methods, such as EUS, and are diagnosed with early CP. CP must be distinguished from several diseases, and in early cases, it must be distinguished from epigastric pain syndrome, one of the subtypes of functional dyspepsia. It has been reported that a relatively large number of early CP patients are misdiagnosed as having epigastric pain syndrome accompanied by pancreatic enzyme abnormalities12). US-RTE should provide useful information when distinguishing early CP and functional dyspepsia. In Japan, periodic medical checkups and comprehensive examinations are widespread. US-RTE may be a tool for screening for early CP during these medical examinations. Although it is essential to proceed with diagnosis after sufficient understanding of clinical signs to avoid unnecessary use of EUS and over-diagnosis, employing US-RTE as a screening method for early CP may lead to a better prognosis.
This study has some limitations. It was a retrospective study based on a relatively small number of patients. In addition, the body mass index (BMI) of the patients was relatively low (median, 20.6 kg/m2) which may have made visualization of the pancreas easier in most of these patients. The disadvantages of US are poor reproducibility, dependence on observer’s skill, and influence on the patient’s body shape and gastrointestinal gas. In this study, RTE was performed using tissue deformation by the abdominal aortic wave; therefore, there seems to have been little difference in the findings among observers. Furthermore, with regards to body shape and gastrointestinal gas, visualization of the pancreatic body and RTE were made possible by performing the examination in a semi-sitting position. Prospective studies with more patients with various BMI values are required to validate the usefulness of US-RTE as a screening method for early CP.
In conclusion, feature values (MEAN, %AREA, COMP) calculated by US-RTE were found to be correlated with the Rosemont classification. US-RTE may be a viable screening method for early CP.
REFERENCES
- 1 Albashir, S., Bronner, M.P., Parsi, M.A., Walsh, R.M. and Stevens, T. 2010. Endoscopic ultrasound, secretin endoscopic pancreatic function test, and histology: correlation in chronic pancreatitis. American Lournal of Gastroenterology 105: 2498–2503.
- 2 Amann, S.T., Yadav, D., Barmada, M.M., O’Connell, M., Kennard, E.D., Anderson, M., et al. 2013. Physical and mental quality of life in chronic pancreatitis: a case-control study from the North American Pancreatitis Study 2 cohort. Pancreas 42: 293–300.
- 3 Ammann, R.W. 1997. A clinically based classification system for alcoholic chronic pancreatitis: summary of an international workshop on chronic pancreatitis. Pancreas 14: 215–221.
- 4 Catalano, M.F., Sahai, A., Levy, M., Romagnuolo, J., Wiersema, M., Brugge, W., et al. 2009. EUS-based criteria for the diagnosis of chronic pancreatitis: the Rosemont classification. Gastrointestinal Endoscopy 69: 1251–1261.
- 5 Carrara, S., Di Leo, M., Grizzi, F., Correale, L., Rahal, D., Anderloni, A., et al. 2018. EUS elastography (strain ratio) and fractal-based quantitative analysis for the diagnosis of solid pancreatic lesions. Gastrointestial Endoscopy 87: 1464–1473.
- 6 Chantarojanasiri, T., Hirooka, Y., Kawashima, H., Ohno, E., Kuwahara, T., Yamamura, T., et al. 2017. Endoscopic ultrasound in diagnosis of solid pancreatic lesions: Elastography or contrast-enhanced harmonic alone versus the combination. Endoscopy International Open E1136–1143.
- 7 Chong, A.K., Hawes, R.H., Hoffman, B.J., Adams, D.B., Lewin, D.N. and Romagnuolo, J. 2007. Diagnostic performance of EUS for chronic pancreatitis: a comparison with histopathology. Gastrointestinal Endoscopy 65: 808–814.
- 8 Conwell, D.L., Lee, L.S., Yadav, D., Longnecker, D.S., Miller, F.H., Mortele, K.J., et al. 2014. American pancreatic association practice guidelines in chronic pancreatitis: evidence-based report on diagnostic guidelines. Pancreas 43: 1143–1162.
- 9 Das, A., Sivak Jr, M.V. and Chak, A. 2001. Cervical esophageal perforation during EUS: a nation survey. Gastrointestinal Endoscopy 53: 599–602.
- 10 Dominguez-Muñoz, J.E., Iglesias-Garcia, J., Castiñeira Alvariño, M., Regueira, M.L. and Lariño-Noia, J.E. 2015. EUS elastography to predict pancreatic exocrine insufficiency in patients with chronic pancreatitis. Gastrointestinal Endoscopy 81: 136–142.
- 11 Eloubeidi, M., Tamhane, A., Lopes, T., Morgan, D. and Cerfolio, R. 2009. Cervical esophageal perforations at the time of endoscopic ultrasound: a prospective evaluation of frequency, outcomes, and patient management. American Journal of Gastroenterology 104: 53–56.
- 12 Hashimoto, S., Futagami, S., Yamawaki, H., Kaneko, K., Kodaka, Y., Wakabayashi, M., et al. 2017. Epigastric pain syndrome accompanying pancreatic enzyme abnormalities was overlapped with early chronic pancreatitis using endosonography. Journal of Clinical Biochemistry Nutrition 61: 140–145.
- 13 Hernandez, L.V. and Catalano, M.F. 2010. EUS in the diagnosis of early-stage chronic pancreatitis. Best Practice Research Clinical Gastroenterology 24: 243–249.
- 14 Itokawa, F., Itoi, T., Sofuni, A., Kurihara, T., Tsuchiya, T., Ishii, K., et al. 2011. EUS elastography combined with the strain ratio of tissue elasticity for diagnosis of solid pancreatic masses. Journal of Gastroenterology 46: 843–853.
- 15 Itoh, Y., Itoh, A., Kawashima, H., Ohno, E., Nakamura, Y., Hiramatsu, T., et al. 2014. Quantitative analysis of diagnosing pancreatic fibrosis using EUS-elastography (comparison with surgical specimens). Jounal of Gastroenterology 49: 1183–1192.
- 16 Kalmin, B., Hoffman, B., Hawes, R. and Romagnuolo, J. 2011. Conventional versus Rosemont endoscopic ultrasound criteria for chronic pancreatitis: comparing interobserver reliability and interest agreement. Cannadian Journal of Gastroenterology 25: 261–264.
- 17 Karlson, B.M., Ekbom, A., Josefsson, S., McLaughlin, J.K., Fraumeni. Jr, J.F. and Nyren, O. 1997. The risk of pancreatic cancer following pancreatitis: an association due to confounding? Gastroenterology 113: 587–592.
- 18 Kim, S.Y., Cho, J.H., Kim, Y.J., Kim, E.J., Park, J.Y., Jeon, T.J., et al. 2017. Diagnostic efficacy of quantitative endoscopic ultrasound elastography for differentiating pancreatic disease. Journal of Gastroenterology and Hepatology 32: 1115–1122.
- 19 Kongkam, P., Lakananurak, N., Navicharern, P., Chantarojanasiri, T., Aye, K., Ridtitid, W., et al. 2015. Combination of EUS-FNA and elastography (strain ratio) to exclude malignant solid pancreatic lesions: A prospective single-blinded study. Journal of Gastroenterology and Hepatology 30: 1683–1689.
- 20 Kuwahara, T., Hirooka, Y., Kawashima, H., Ohno, E., Ishikawa, T., Kawai, M., et al. 2017. Quantitative diagnosis of chronic pancreatitis using EUS elastography. Journal of Gastroenterology 52: 868–874.
- 21 Löhr, L.M., Dominguez-Munoz, E., Rosendahl, J., Besselink, M., Mayerie, J., Lerch, M.M., et al. 2017. United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United European Gastroenterology Journal 5: 153–199.
- 22 Lowenfels, A.B., Maisonneuve, P., Cavallini, G., Ammann, R.W., Lankisch, P.G., Andersen, J.R., et al. 1993. Pancreatitis and the risk of pancreatic cancer. International Pancreatitis Study Group. The New England Journal of Medicine 328: 1433–1437.
- 23 Machicado, J.D., Amann, S.T., Anderson, M.A., Abberbock, J., Sherman, S., Conwell, D., et al. 2017. Quality of life in chronic pancreatitis is determined by constant pain, disability/unemployment, current smoking, and associated co-morbidities. American Journal of Gastroenterology 112: 633–642.
- 24 Malka, D., Hammel, P., Maire, F., Rufat, P., Madeira, I., Pessione, F., et al. 2002. Risk of pancreatic adenocarcinoma in chronic pancreatitis. Gut 51: 849–852.
- 25 Masamune, A., Kikuta, K., Nabeshima, T., Nakano, E., Hirota, M., Kanno, A., et al. 2017. Nationwide epidemiological survey of early chronic pancreatitis in Japan. Journal of Gastroenterology 52: 992–1000.
- 26 Morikawa, H., Fukuda.K., Kobayashi, S., Fujii, H., Iwai, S., Enomoto, M., et al. 2011. Real-time tissue elastography as a tool for the noninvasive assessment of liver stiffness in patients with chronic hepatitis C. Journal of Gastroenterology 46: 350–358.
- 27 Mortensen, M.B., Fristrup, C., Holm, F.S., Pless, T., Durup, J., Ainsworth, A.P., et al. 2005. Prospective evaluation of patient tolerability, satisfaction with patient information, and complications in endoscopic ultrasonography. Endoscopy 37: 146–153.
- 28 Mullady, D.K., Yadav, D., Amann, S.T., O’Connell, M.R., Barmada, M.M., Elta, G.H., et al. 2011. Type of pain, pain-associated complications, quality of life, disability and resource utilisation in chronic pancreatitis: a prospective cohort study. Gut 60: 77–84.
- 29 Rustemović, N., Kalauz, M., Grubelić Ravić, K., Iveković, H., Bilic, B., Ostojic, Z., et al. 2017. Differentiation of pancreatic masses via endoscopic ultrasound strain ratio elastography using adjacent pancreatic tissue as the reference. Pancreas 46: 347–351.
- 30 Sarner, M. and Cotton, P.B. 1984. Classification of pancreatitis. Gut 25: 756–759.
- 31 Schneider, A., Löhr, J.M. and Singer, M.V. 2007. The M-ANNHEIM classification of chronic pancreatitis: introduction of a unifying classification system based on a review of previous classifications of the disease. Journal of Gastroenterology 42: 101–119.
- 32 Shimosegawa, T., Kataoka, K., Kamisawa, T., Miyakawa, H., Itoh, T., et al. 2010. The revised Japanese clinical diagnostic criteria for chronic pancreatitis. Journal of Gastroenterology 45: 584–591.
- 33 Tatsumi, C., Kudo, M., Ueshima, K., Kitai, S., Takahashi, S., Inoue, T., et al. 2008. Noninvasive evaluation of hepatic fibrosis using serum fibrotic markers, transient elastography (FibroScan) and real-time tissue elastography. Intervirology 51: 27–33.
- 34 Thuluvath, P.J., Imperio, D., Nair, S. and Cameron, J. 2003. Chronic pancreatitis: Long-term pain relief with or without surgery, cancer risk, and mortality. Journal of Clinical Gastroenteology 36: 159–165.
- 35 Trikudanathan, G., Munigala, S., Barlass, U., Malli, A., Han, Y., Sekulic, M., et al. 2017. Evaluation of Rosemont criteria for non-calcific chronic pancreatitis (NCCP) based on histopathology—A retrospective study. Pancreatology 17: 63–69.
- 36 Wallace, M.B., Hawes, R.H., Durkalski, V., Chak, A., Mallery, S., Catalano, M.F., et al. 2001. The reliability of EUS for the diagnosis of chronic pancreatitis: interobserver agreement among experienced endosonographers. Gastrointestinal Endoscopy 53: 294–299.