Abstract
We explored the associations of job strain with sleep and alertness of shift working
female nurses and nursing assistants. Participants (n=95) were recruited from the Finnish
Public Sector Study, from hospital wards that belonged to the top or bottom quartiles on
job strain. Participants’ own job strain was at least as high in high-strain group or low
in low-strain group as the ward’s average. The study included three-week measurements with
sleep diary and actigraphy. Psychomotor Vigilance Test (PVT) was performed during one
pre-selected morning and night shift and a day off. Sleep efficiency before morning shifts
was lower in the high-strain than low-strain group (p=0.03). Low-strain group took more
often (72 vs. 45%; p<0.01) and longer naps (62 vs.
35 min; p=0.01) before the first night shift than
high-strain group. Difficulties initiating sleep were more common in high-strain group,
especially after evening shifts (p<0.01). High-strain
group had more often at least one lapse in PVT during the night shift
(p=0.02). Average sleep duration (06:49h) and efficiency
(89%) did not differ between these groups. In conclusion, high job strain is associated
with difficulties initiating sleep and reduced psychomotor vigilance in night shifts.
Shift working contributed to impaired sleep in both high and low job strain group.
Individual and organization-based actions are needed to promote sufficient sleep in shift
working nurses, especially with high job strain.
Introduction
Nursing work is stressful1),
affectively intense, decision-rich2), typically includes numerous interruptions3) and carries a risk for medical
errors4). There is
substantial evidence to suggest that long-term exposure to stress may adversely affect not
only nurses health, increasing the risk of various diseases, such as coronary heart
disease5) and
depression6) and the risk
for disability pensioning7) but
also put patients at risk8).
Impaired recovery and compromised sleep may be important mediators between stress and
illnesses9). For shift
workers, long-term stress may increase the probability of a co-manifestation of several
individual health risk factors, such as sedentary lifestyle, high blood pressure and
cholesterol levels, that predispose to chronic disease10).
Psychosocial stress, in general, is assumed to have a negative effect on sleep11, 12) but relatively little research exists on
work-related stress and sleep13) when sleep is measured not merely with subjective methods.
Psychosocial stress can potentially lead to impaired sleep through direct and indirect
pathways. Heightened arousal with elevated cortisol secretion increases difficulties in
initiating sleep14) and sleep
fragmentation15). Long-term
psychosocial stress may also lead to health risk behaviors, such as smoking, physical
inactivity and unhealthy diet10), which in turn affect negatively on sleep.
The hypothesis that work-related stress, such as job strain -a condition of high job
demands combined with low control at work16) -causes sleep disruption17) and adversely affects sleep18) has been supported by cross-sectional
questionnaire studies of daytime workers19). For example, in an earlier study the prevalence of disturbed
sleep was 30% among the high-strain workers based on the Karasek’s model versus 5% in the
low-strain group20). Work
stress produces significant psycho-physiological activation and especially a high level of
work-rumination is a strong predictor of sleep complaints19). It is possible that job strain impairs sleep more
among shift workers that are exposed to the additional causes of insomnia due to working in
shifts. Shift work is closely tied up with shortened or disturbed sleep in morning and night
shifts, problems to fall asleep in connection with quick returns -that is to say a morning
shift after an evening shift- and problems to wake up too early during the day
sleep21,22,23).
Assessing psychosocial work environment in the most precise and unbiased way is a major
challenge in psychosocial working conditions research24). We face this challenge by using a hospital ward level
estimation of job strain to reduce subjectivity bias that may arise for example from
negative affectivity24). Also,
integrating research on job stressors and working times is needed25), since studies of job strain are mainly conducted
among daytime workers19).
To our knowledge, there are no studies that have measured both exposure to job strain and
sleep quantity in shift work. Despite extensive research among nursing staff, we found no
earlier research reporting shift-specific sleep lengths or sleep disturbances according to
job stress. We used daily actigraphic measures to estimation of sleep length and quality in
different shifts during one natural shift cycle of 3 wk. We hypothesized that a) sleep
quantity, quality and alertness are impaired by shifts among female nursing personnel and
that b) these impairments are exacerbated among those who are exposed to job strain.
Methods
Study sample
The participants were recruited from The Finnish Public Sector Study survey 2008
respondents (N=52 891, response rate 72%). From this sample, native Finnish speaking
female health care professionals (hence referred to as “nurses” for brevity) with night
shift work were identified (n=5,615) (Fig. 1). The present sample included participants from 5 hospitals or health care
districts and 4 cities in Southern Finland. The nurses were from 59 wards, which had an
average of 37 employees.

An invitation letter was sent to the workplace of nurses fulfilling the following
inclusion criteria (n=422): night shift work, age 30–58 yr, native Finnish speaker, Body
Mass Index (BMI) under 35 kg/m2, and at least 3 years work experience in the
same ward. Age limits were set to ensure exposure to working life and to minimize the
probability of retiring. Volunteers with coronary heart disease, insulin-treated diabetes
mellitus, and pregnant or breast feeding mothers were excluded. The participants were not
screened for sleep disorders. The main reasons for exclusion were changing ward or
workplace (n=22) or quitting night shift work (n=21) after the 2008 survey.
Job strain was determined with three questions on job demand (JD) i.e. pace and pressure
of work tasks and nine questions on job control (JC) i.e. individual autonomy over work
timing and methods26) using a
5 -point Likert -type scale ranging from 1 (strongly disagree) to 5 (strongly agree)
derived from Karasek’s Job Content Questionnaire (JCQ)16). As described elsewhere26), the high (HJS) and low (LJS) job strain groups
were divided by grouping the wards with at least 5 respondents on the JD and JC scales at
the ward level, using median split to identify HJS (high demands and low control) and LJS
(low demands and high control) wards. With these cut-off points, we identified nurses from
these wards who belonged to the HJS- or LJS-groups based on their individual mean scores
of JD and JC. To increase contrast between job strain groups, the nurses belonging to the
quartile with the least strain in the HJS-group and the most strain in the LJS-group were
excluded. The mean values for job demands/job control were 4.56/3.20 in the HJS-group and
2.64/4.11 in the LJS-group (Mean Difference 1.92/–0.90, p<0.01). The
reliability coefficients for JCQ for the invited (n=422) were good (Cronbach’s α=0.87 for
JD and α=0.80 for JC).
The representativeness of the 95 participants was tested by comparing them to the 422
invited. There were no statistical differences (p-values >0.11) in
responses on the 2008 survey between participated and invited on age, education level,
work experience, number of children, BMI, habitual sleep length, sleep need, or sleep
disturbances. More participants were from the LJS-group than the HJS-group
(p<0.01) and fewer from the two major health care districts
(p<0.01).
The study was approved by the Ethical Committee of the Hospital district of Helsinki and
Uusimaa. Written informed consent was obtained from each participant. The participants
were compensated for travelling expenses and paid 50 Euros compensatory allowance for
participation.
Background variables
The study included an Internet questionnaire featuring questions about work shifts and
work conditions and typical coping strategies in stressful situations. The background
variables were education level, physical activity (times per week, at least 30 min/d,
during past 3 months), BMI, number of children, smoking, alcohol consumption, medication
use, stressful life events during past 12 months27), morningness-eveningness questionnaire28) and Beck Depression Inventory
(BDI-II)29). There was no
missing data in the Internet questionnaires, as answering to all questions was
required.
Participants
Of the 95 participants, 42 (44%) were in the HJS-group and 53 (56%) in the LJS-group. The
participants worked most often in medical-surgical wards (45%, n=43) and intensive care or
emergency units (15%, n=14). Their mean age was 47.2 yr (range 31–59), with no significant
difference between the job strain groups. Shift work experience, family care-giving
responsibility, stressful life-events, chronotype, BMI, smoking, alcohol or caffeine
consumption (Table 1), medication use or measurement season showed no stress group differences
either. Two of the participants in HJS-group scored points typical for clinical depression
according to the BDI-II compared to none in LJS-group (p=0.19). The
proportion of nurses was higher in the LJS-group (81%) than in the HJS-group (60%,
p=0.02). The participants in the LJS-group were physically more active
than the HJS-group (p<0.01).
Table 1.
Descriptive statistics
|
High Job Strain n=42 |
|
Low Job Strain n=53 |
p-value1 |
DF |
t-value |
| Mean |
SD |
Mean |
SD |
| Age (yr) |
47.7 |
(6.4) |
|
46.7 |
(7.5) |
0.52 |
93 |
0.64 |
| BMI (kg/m2) |
26.7 |
(4.1) |
|
25.6 |
(4.0) |
0.20 |
93 |
1.29 |
| Shift work experience (yr) |
18.7 |
(7.9) |
|
16.9 |
(7.6) |
0.27 |
90 |
1.11 |
| Caffeine doses per 24 h |
4.6 |
(1.9) |
|
4.0 |
(1.9) |
0.14 |
93 |
1.51 |
|
% |
(n) |
|
% |
(n) |
p-value2 |
|
| Education |
|
|
|
|
|
0.02 |
|
Nurse3 |
60 |
(25) |
|
81 |
(43) |
|
| Nursing assistant4 |
40 |
(17) |
|
19 |
(10) |
|
| Physical activity5 |
|
|
|
|
|
<0.01 |
|
<3 × week |
29 |
(12) |
|
6 |
(3) |
|
| ≥3 × week |
71 |
(30) |
|
94 |
(50) |
|
| Family care-giving responsibility6 |
|
|
|
|
|
0.51 |
|
Yes |
62 |
(21) |
|
69 |
(31) |
|
| No |
38 |
(13) |
|
31 |
(14) |
|
| Stressful life event7 |
|
|
|
|
|
0.34 |
|
Yes |
66 |
(27) |
|
75 |
(39) |
|
| No |
34 |
(14) |
|
25 |
(13) |
|
| Cigarette smoking |
|
|
|
|
|
0.98 |
|
Yes |
19 |
(8) |
|
19 |
(10) |
|
| No |
81 |
(34) |
|
81 |
(43) |
|
| Alcohol consumption |
|
|
|
|
|
0.85 |
|
Never/seldom |
45 |
(19) |
|
47 |
(25) |
|
| Regularly8 |
55 |
(23) |
|
53 |
(28) |
|
| Chronotype |
|
|
|
|
|
0.90 |
|
Morning-type |
45 |
(19) |
|
51 |
(27) |
|
| Evening-type |
55 |
(23) |
|
49 |
(26) |
|
1Independent samples t-test, 2Pearson
χ2, 3Nurse, midwife, public health nurse, X-ray nurse,
deaconess-nurse, 4Nursing assistant, practical nurse, nursery nurse,
mental nurse, 5 ≥30 min/d, during past 3 months, 6Children
under 18 yr, 7During the past year, 8 ≥2 times/month, 24 g
alcohol per time.
During the three-week field study, the participants’ sleep-wake rhythm was measured by
actigraphy (Actiwatch AW7, Cambridge Neurotechnology Ltd, Cambs, UK) and a sleep diary.
The actigraph was continuously worn on the non-dominant wrist, except at moments of
hygiene concern at the work place. Actigraphy data were scored using 1 min epochs and
analyzed with Actiwatch Activity and Sleep Analysis 7-software (Cambridge Neurotechnology
Ltd, Cambs, UK).
The Internet questionnaire included questions about habitual sleep length and amount of
sleep needed to feel rested on a continuous scale, and frequency (never/seldom, quite
seldom, quite often or often/frequently) of difficulties in initiating sleep, difficulties
in maintaining good sleep, and excessive daytime sleepiness during the past four weeks.
Sleep efficiency (SE) was measured by actigraphy and calculated from the ratio of the time
asleep to the time in bed. The limit of reduced SE was set to be <85%30). Sleep was classified
insufficient if there was a 20% discrepancy between the actual sleep amount and the
subjective evaluation of sleep need.
In the sleep diary the participants kept a record of times at which they went to sleep
and got up, and their working hours. The nurses reported self-evaluated sleep latency,
being awake during the night, ease of waking up, number of and duration of naps, the
amount of alcohol or caffeinated drinks and use of sleep promoting medication.
The actigraphy data collection lasted on average 20.6 d (range 8–25 d) covering 95% of
intended measurements. The sleep diaries were filled in with 95% of values.
Psychomotor vigilance test (PVT)31) was done during pre-selected, controlled work shifts: (i) a
morning shift after at least two earlier morning shifts, (ii) a night shift after a
morning or evening shift and (iii) the second consecutive day off. PVT was installed on HP
ipaq 514 mobile phone (Hewlett-Packard Company, Palo Alto, CA, USA). A 5-min version of
the PVT was done in (i) the morning shift between 12–15 and in the evening between 19–21,
(ii) before night shift between 19–21, and at work between 02–04 and (iii) on a day-off
between 12–15 o’clock. To minimize the effect of learning, the nurses were instructed to
practice the PVT three times32) before the first test day. Answering was done by pressing
the zero button. Reaction times >500 milliseconds were regarded as lapses. PVT tests
were completed in 97% of planned tests.
Work shifts
The data on work hours and work shifts during the field measurement period was obtained
from realized rosters (n=88), or without the roster (n=7), from the sleep diary. The
three-week rosters included on average 6 morning, 3 evening, 2 night, and 1 extended
shifts. The nurses in the HJS-group had on average one morning shift more and one extended
shift less than the nurses in the LJS-group (7 vs. 6, p=0.01 and 0 vs. 1,
p=0.02). The morning shifts were mainly timed 7:00–15:00, the evening
shifts 14:00–22:00 and night shifts 21:00–07:00. There was no statistical difference
between job strain groups in total number of work hours, number of work shifts or night
shifts during the field measurements.
Statistical analysis
Statistical analyses were conducted by PASW 18.0 (Chicago, IL, USA). Pearson Chi-square
test (χ2), Student’s t-test, Fisher’s exact test, one-way
analysis of variance (ANOVA) or Mann-Whitney U-test were used to compare job strain group
differences in individual and job characteristics depending on the variable and the
normality of the distribution of the variable. Age and education level were used as
covariates. A p-value <0.05 indicates statistically significant result
throughout the study.
Results
Sleep length
Analyses adjusted for age showed that the HJS- and LJS-groups did not differ with respect
to the self-reported habitual sleep length.
The actigraphy data showed that the main sleep period lasted, on average, 06:46 h in the
HJS-group and 06:51 h in the LJS-group on average (Table 2) with no group differences in connection with different shifts or the
pre-selected shifts.
Table 2.
Sleep length and efficiency by actigraphy in connection with different work
shifts
|
Sleep length (h) |
Reduced sleep efficiency (<85%) |
| High Job Strain |
Low Job Strain |
p -value1 |
High Job Strain% (n) |
Low Job Strain% (n) |
p-value2 |
| Mean |
Range |
Mean |
Range |
| 3 weeks |
06:46 |
04:52–07:51 |
06:51 |
04:54–08:22 |
0.76 |
17 (7) |
9 (5) |
0.36 |
| Before morning shifts |
05:49 |
04:10–07:03 |
06:05 |
04:02–07:42 |
0.15 |
21(9) |
6 (3) |
0.03 |
| Quick returns3 |
05:22 |
03:19–07:31 |
05:50 |
03:53–08:17 |
0.06 |
17 (6) |
15 (7) |
1.00 |
| After evening shifts4 |
06:13 |
03:58–08:10 |
06:41 |
04:34–08:48 |
0.08 |
20 (8) |
11 (6) |
0.26 |
| After night shifts |
04:12 |
02:03–06:14 |
04:35 |
00:13–07:40 |
0.11 |
19 (8) |
10 (5) |
0.24 |
| After days off |
07:20 |
05:28–09:30 |
07:20 |
05:35–09:32 |
0.85 |
14 (6) |
21 (11) |
0.59 |
1Mann-Whitney U-test, 2Fisher’s exact test,
3Between evening and morning shift (n=84; HJS n=37, LJS n=47),
4Includes double shifts (morning and evening shift).
Sleep efficiency (SE) was more often reduced (<85%) before morning shifts in the
HJS-group than LJS-group (21 vs. 6%, p=0.03) but not on average or in
connection with other work shifts, quick returns (Table 2) or the pre-selected shifts. The average SEs were similar in both stress
groups (HJS 89%, range 82–94% vs. LJS 89% range 84–95%) and SE varied very little in
connection with different work shifts, being highest after night shifts (HJS 88%, range
81–94% vs. LJS 90%, range 79–96%).
The proportion of nurses with insufficient sleep was 38% in the HJS-group and 25% in the
LJS-group, but the difference did not to reach statistical significance
(p=0.15). The proportion of nurses’ who often had difficulties
initiating sleep when working shifts, was higher in the HJS-group than in the LJS-group
(p<0.01). Within shift categories this difference was observed in
connection with evening shifts (p=0.01). Furthermore, the proportion of
nurses having difficulties initiating sleep after waking up during the night was larger in
the HJS-group than the LJS-group (p=0.03). The occurrence of any sleep
disturbance at least 2–4 times a week was somewhat higher in the HJS-group, than in the
LJS-group, but the difference did not reach statistical significance
(p=0.15) (Table 3). No other stress group differences were found in sleep disturbances.
Table 3.
Insufficient sleep and sleep disturbances
|
High Job Strain |
Low Job Strain |
p-value1 |
| % |
(n) |
% |
(n) |
| Insufficient sleep2 |
38 |
(16) |
25 |
(13) |
0.15 |
| Any sleep disturbance |
|
2–4 times/wk |
76 |
(32) |
62 |
(33) |
0.15 |
| ≥5 times/wk |
31 |
(13) |
25 |
(13) |
0.49 |
| Often difficulties in initiating sleep |
|
All shifts |
76 |
(32) |
42 |
(22) |
<0.01 |
| Before morning shifts |
36 |
(16) |
25 |
(13) |
0.44 |
| After evening shifts |
64 |
(27) |
30 |
(16) |
0.01 |
| After night shifts |
24 |
(10) |
19 |
(10) |
0.19 |
| After days off |
7 |
(3) |
9 |
(5) |
0.60 |
| Often difficulties in initiating sleep after waking
up |
|
All shifts |
76 |
(32) |
55 |
(29) |
0.03 |
| Before morning shifts |
48 |
(20) |
32 |
(17) |
0.45 |
| After evening shifts |
45 |
(19) |
28 |
(15) |
0.26 |
| After night shifts |
62 |
(26) |
43 |
(23) |
0.32 |
| After days off |
19 |
(8) |
13 |
(7) |
0.78 |
1Pearson χ2, 2Actual sleep amount ≤80% of
subjective sleep need.
Approximately two thirds of the participants never used sleep promoting medication. The
use of medication was lower during the past three months (HJS 12 vs. LJS 5%,
p=0.08) than during the three-week field measurements (21 vs. 12%,
p=0.27).
Napping
Napping was very common; according to the sleep diaries, 93% (n=88) of the nurses took at
least one nap and 22% (n=21) took naps at least twice a week. Total sleep length per 24 h
increased only with few minutes with naps included (HJS 06:52 h vs. LJS 07:00h, p=0.30).
Shift-specific sleep lengths of main sleep periods showed no significant difference
between nappers and non-nappers; nappers slept on average 5 minutes longer before morning
shifts and 15 minutes longer after night shifts than non-nappers.
Napping before the first night shift was common, and the proportion of nappers was higher
in the LJS- than in the HJS-group (72 vs. 45%, p<0.01). The average nap duration before
night shift was shorter in the HJS-group than in the LJS-group (35 vs. 62 min, p=0.01).
The frequencies or durations of naps showed no other statistical differences between the
stress groups (Table 4). Less than one third (29%, n=18) of those who had at least two consecutive
night shifts, took naps between two consecutive night shifts. Taking naps during the night
shift was exceptional, as only 4% had slept on duty at least once.
Table 4.
The proportions of nappers and average durations of naps according to sleep
diary
|
Napping frequency |
Nap duration (min) |
| High Job Strain |
Low Job Strain |
p-value1 |
High Job Strain |
Low Job Strain |
DF |
t-value |
p-value |
| % |
(n) |
% |
(n) |
Mean |
SD |
Mean |
SD |
| Nappers2 |
91 |
(38) |
94 |
(50) |
0.70 |
37 |
(42) |
45 |
(31) |
93 |
–1.12 |
0.263 |
| After morning shift |
67 |
(28) |
59 |
(31) |
0.52 |
18 |
(31) |
17 |
(24) |
93 |
0.24 |
0.813 |
| Before 1st night shift |
45 |
(19) |
72 |
(38) |
<0.01 |
35 |
(59) |
62 |
(68) |
– |
– |
0.014 |
| On a day off |
67 |
(28) |
64 |
(34) |
0.80 |
21 |
(29) |
29 |
(35) |
93 |
–1.05 |
0.303 |
1Pearson χ2, 2At least once during 3-wk
measurement, 3Independent samples t-test,
4Mann-Whitney U-test.
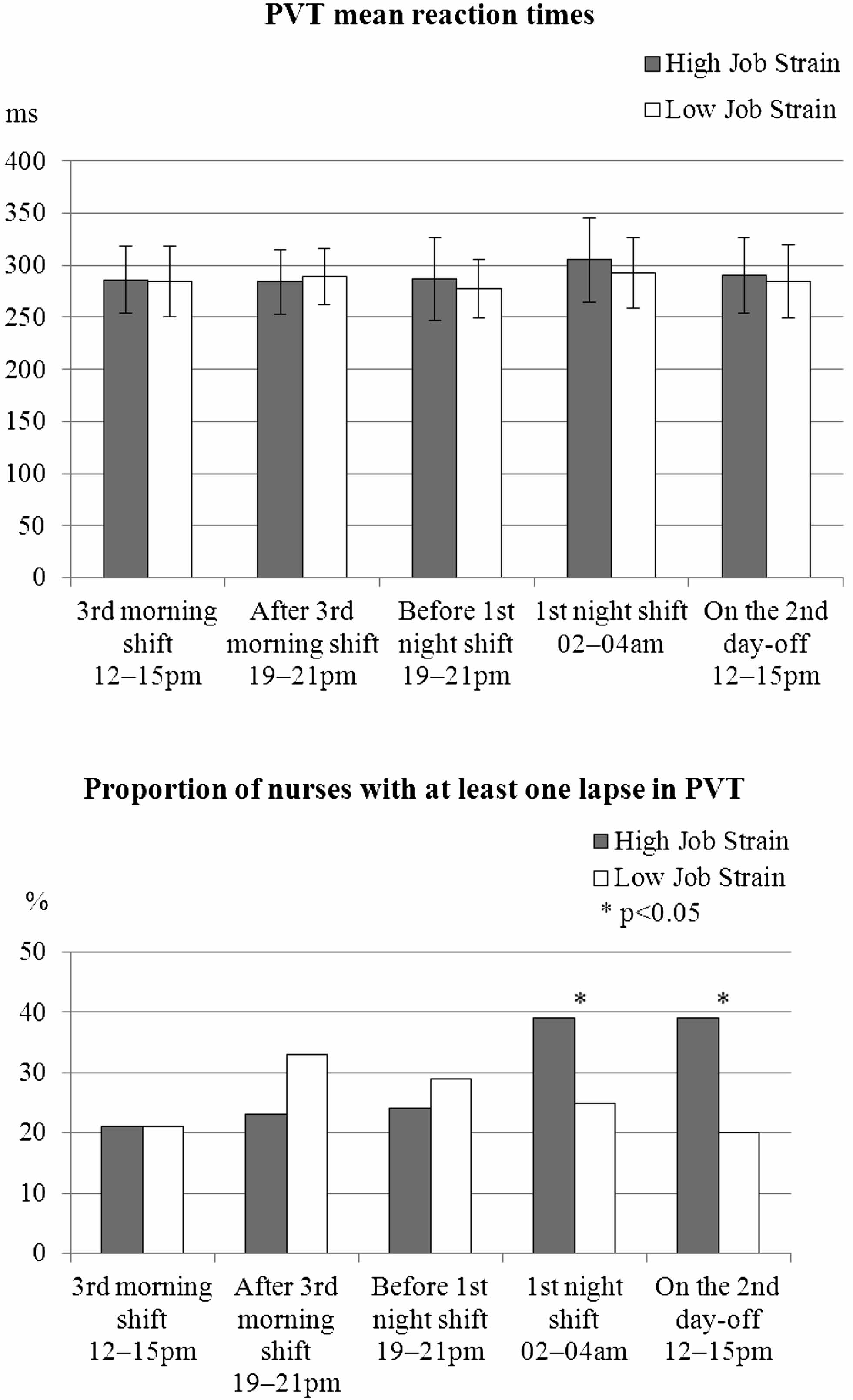
The proportion of nurses with at least one PVT lapse in the night shift was higher in the
HJS-group than in the LJS-group (40 vs. 26%, p=0.02, controlled with
education). There were no other statistically significant differences in the occurrence of
lapses in PVT tests on workdays. However, the day off test showed a higher proportion of
nurses with at least one lapse in the HJS-group (39 vs. 20%, p=0.03)
(Fig. 2), but the difference was not statistically significant with education as a
covariate. Mean PVT reaction times were similar in both job strain groups. Napping before
or during the night shift before PVT test had no effect on the results.
We repeated analyses with age and education level as covariates with no essential change
in the results.
Discussion
This is the first study to examine the relationship of exposure to job strain on
shift-specific sleep quantity and quality, and alertness among shift working health care
personnel. The results showed that job strain was associated with increased difficulties in
initiating sleep in relation to all work shifts and especially after evening shifts. Reduced
sleep efficiency was more common in the high-strain group before morning shifts. Job strain
was related with higher amount of PVT lapses during the night shift and less and shorter
naps before the night shift. Contrary to our hypothesis there were no general differences in
sleep length or sleep efficiency according to job strain indicating that the additional
burden of job strain becomes visible only in specific shift combinations.
We found job strain-related increases in sleep complaints in situations where shift workers
typically face insomnia: sufficient napping before a night shift, daytime sleep after a
night shift -or while going to sleep after evening shifts21,22,23). Few studies have investigated the effect of evening shifts
on sleep33). Sleep difficulties
after evening shifts are probably due to work rumination19) and inability to relax after a shift ending too close to
sleep14). In addition to
the earlier results19,20,21), in this data difficulties in initiating sleep after waking
up were also more common in the HJS-group.
In concordance with our hypothesis and earlier evidence17, 34), shortened sleep and mild sleep disturbances were highly
prevalent among shift workers. The participants’ sleep measured with actigraphy was on
average half an hour shorter than all shift working nurses in Finnish Public Sector Study
(n=7,023) and almost an hour shorter than a survey of Finnish women shows (7:37h)34). The total sleep amount increased
only by a few minutes with self-reported naps added to the average sleep length, likewise to
the study of Ruggiero et al.35). About 30% of the nurses had an insufficient sleep length,
which is similar to the study of Åkerstedt, Ingre, Broman & Kecklund36).
Job strain is associated with disturbances in the sleep-wake pattern. Our results in both
job strain groups are in line with the findings of shift working: night shifts and morning
shifts are particularly obstructing for sufficient sleep36,37,38). Also, in this study the sleep length was longer after the
evening shift than after the morning or night shift. Participants’ sleep after night shifts
was less than five hours, which is in agreement with research showing sleep shortening by
1–4 h after a night shift22,
39). Approximately
six hours of sleep before a morning shift is comparable with earlier research reporting
2–4 h shortening of sleep38)
before early morning shifts.
Job strain induced additional sleep complaints to these shift workers mainly after evening
shifts and in napping before the first night shift. However, there were no significant
differences in total sleep length, sleep efficiency or napping between the groups. After
evening shifts, the difference in sleep length between the job strain groups was less than
30 min while sleep curtailment for all participants after night shifts was almost three
hours compared to days off. We thus conclude that the role of work strain on the sleep of
shift workers is probably of lower significance than the effect of shift working in
general.
Job strain affected napping; there was a significant difference between the job strain
groups in taking naps before the first night shift. In this data, two thirds took a nap
before the first night shift. Earlier research has shown 56% of nurses and nursing
assistants in a similar shift system nap before first night shift40). Among midwifes 40% of the night shifts were
preceded with a nap41).
Approximately one third of shift workers nap between the consecutive night shifts33, 36) but there are no earlier studies of the effect of
job strain on napping. According to Härmä et al.40), non-napping nurses before a night shift had more
insomnia symptoms. It is presumable work-related stress with difficulties in falling asleep
is associated with poorer ability to nap before first night shift. Also non-optimal time for
falling asleep may affect to ability to nap. Even then, majority of nurses in our data used
naps to prepare themselves for the first night shift, probably from the experiences of
severe sleepiness in the first night shift.
In previous studies of dayworkers42), high mental distress frequently was associated with reduced
sleep efficiency. However, in study of shift workers, the shortened sleep of shift workers
was often compensated for by high sleep efficiency43).The sleep efficiencies in this study were above 85% which
is an indication of a consolidated sleep. The proportions of reduced SE did not differ
between the stress groups in connection with the other work shifts except for morning
shifts. Moreover, actigraphy measurement of sleep length measurement slightly overestimates
total sleep time44). This
strengthens the observation that shift working nurses suffer from insufficient sleep and the
actual sleep durations are likely to be even shorter than reported in the present study. The
12% use of sleep promoting medication in the LJS-group equals the sleep medication use
reported in a population study of Scandinavian females45). One fifth of the HJS-group used sleep medication during
the field measurements, which equals to other study among the nursing staff46). We suggest that nurses may use
sleep promoting medication to avoid cumulative stress and sleep deprivation.
There is lack of research of alertness in connection with work stress. In our data, the
occurrence of at least one lapse in PVT was higher in high than low-strain nurses in the
night shift. Importantly, these night shift tests were conducted in circadian rhythm and
recovery controlled pre-selected shift arrangements, where sleepiness was pronounced in the
HJS-group only. During night shift, especially the high-strain nurses might benefit from
planned naps, which suppress sleepiness47, 48). However, job strain was not associated with other PVT
scores. A recent study35) found
no differences between night shift and day shift nurses in a standard 10-min PVT either.
As a whole, the associations of job strain with sleep in shift working health care staff
were fewer than predicted based on earlier results21,22,23). In this group of shift workers, the additional burden of job
strain on sleep and alertness becomes evident only in specific shift combinations. The
effects of job strain on sleep may be emphasized among day workers19) and workers with extended work hours49).
Strengths and limitations of the study
The strengths of this field study nested in on-going epidemiological study among nursing
staff are: firstly, the measure of exposure to job stressors was based on a mean score
from the same ward. This was likely to result in reduced effect of subjectivity on the
measure and therefore in a less biased estimate of the environmental job strain.
Secondly, we used both actigraphy and sleep diary data to estimate the habitual sleep
length, whereas many earlier studies only have sleep diary data38). Furthermore, the three-week actigraphy
measurement period was of longer duration in this study than in most other studies, where
such measurements have lasted mainly up to 7 nights.
The participants formed a homogenous sample of employees, which can be considered as a
clear strength of the study. Our participants were highly very similar in aspects other
than job strain: they were all relatively healthy shift working females who, for example,
had similar amount of work hours and only two of them scored points typical for clinical
depression. Thus, it is not likely that there were non-measured confounding factors
between the groups. There was a significant difference between the stress groups in
education level that had no confounding effect on sleep results.
There are some limitations in our study as well. The study sample of nursing employees
was likely to result in reduced variance of job strain and power to establish clear cut
between groups in sleep and alertness. High and low job strain groups did not differ in
their level of stress as much as high and low stress groups typically do in studies of the
general population or mixed occupational groups. Among nursing staff, the concept of low
strain is relative, when for example majority of nurses in both groups had to often hurry
at work.
Although we used exposure data from a prospective data set the design of analyzing the
effect of job strain on sleep was cross-sectional, prohibiting us to draw conclusions
regarding causality. Job Content Questionnaire was used to assess job strain at one time
point, preventing us to follow changes in exposure to environmental job strain or capture
the past pattern of exposure other than the participants had been working in the same ward
for at least three years. Using the average job strain level of a ward may be a potential
weakness if the atmosphere in the workplace is affected by influential individuals in the
ward.
Polysomnography would have been an ideal method to detect changes in sleep, as stress has
been shown to affect sleep architechture i.e. amount of slow wave sleep and REM sleep and
number of awakenings50). We
used a 5-min PVT instead of a 10-min PVT for practical reasons in the workplaces. Although
the 5-min test is a viable alternative to the standard 10 min test, it may be less
sensitive to detect sleepiness51). Nevertheless, the job strain group difference came up in
the night shift, but the test might be too short to detect sleepiness in day-time tests. A
useful addition to the data gathered would have been the social support aspects of the JCQ
as well as personality factors to shift work tolerance. Also, it would have been useful to
utilize the voluntary or involuntary nature of naps.
One third of the contacted individuals declined to participate in the study and only 24%
of the employees fulfilling the inclusion criteria participated. We had no personal
contact with potential study participants, which meant that we could not verify whether
the nurses were actually reached or not. Also, the considerable time commitment that the
study required has likely reduced the participation rate. On the other hand, the
participated nurses represented the invited nurses and the field data collected was of
very good quality; only a few (4%) participants refused or failed to follow through with
the field measurements. More volunteers were from the LJS-group, and it is probable that
most affected individuals were unwilling to participate52), which may have diluted the differences observed
between the stress groups.
In future nested studies, it would be important to obtain a personal contact to potential
study participants to enhance the participation rate. Apparently, when measuring the level
of low job strain in health care staff or other homogenous samples, the concept of low
strain is relative and the differences between high and low stress groups are likely to be
rather limited. Therefore, larger sample sizes would be needed to detect group level
differences in job strain. Quitting night shift work was common in this cohort of nursing
professionals and it would be advantageous to study that group too.
Sufficient sleep is important to all shift workers due to its implications to alertness,
recovery and health. More longitudinal studies exploring the effects of job strain on
sleep and irregular working times are needed, because impaired sleep is associated with
severe consequences like occupational injuries, reduced patient safety, and increased risk
of development of several chronic diseases. Ability to control over own work times and
sufficient recovery time between work shifts are useful in reducing occupational stress
and related health outcomes53).
Conclusions
High job strain is associated with difficulties initiating sleep and reduced psychomotor
vigilance in night shifts. Shift working contributed to impaired sleep in both high and low
job strain group. Individual and organization-based actions are needed to promote good and
sufficient sleep in shift working nurses, especially with high job strain.
Acknowledgements
This study was funded by The Academy of Finland (projects 124473, and 132944), The Work
Environment Fund (project 107156), The SalWe Research Program for Mind and Body (TEKES -the
Finnish Funding Agency for Technology and Innovation, grant 1104/10), the EU New OSH ERA and
ERA-AGE2 Research Programmes. Mika Kivimäki is supported by a professorial fellowship from
the Economic and Social Research Council, UK.
We thank Elise Koskenseppä for participant recruitment, Nina Lapveteläinen and Riitta Velin
for arrangements for the field measurements, and Hanna Kaisa Hyvärinen and Jaana Pentti for
statistical support.
References
- 1) Lim J, Bogossian F, Ahern K (2010) Stress and coping in Australian nurses: a
systematic review. Int Nurs Rev 57, 22–31.
- 2) Lothschuetz Montgomery K, Geiger-Brown J (2010) Is it time to pull the plug
on 12-hour shifts?: Part 2. Barriers to change and executive leadership strategies. J Nurs
Adm 40, 147–9.
- 3) Geiger-Brown J, Trinkoff AM (2010) Is it time to pull the plug on 12-hour
shifts? Part 1. The evidence. J Nurs Adm 40, 100–2.
- 4) Arimura M, Imai M, Okawa M, Fujimura T, Yamada N (2010) Sleep, mental health
status, and medical errors among hospital nurses in Japan. Ind Health 48,
811–7.
- 5) Kivimäki M, Nyberg ST, Batty GD, Fransson EI, Heikkilä K, Alfredsson L,
Bjorner JB, Borritz M, Burr H, Casini A, Clays E, De Bacquer D, Dragano N, Ferrie JE,
Geuskens GA, Goldberg M, Hamer M, Hooftman WE, Houtman IL, Joensuu M, Jokela M, Kittel F,
Knutsson A, Koskenvuo M, Koskinen A, Kouvonen A, Kumari M, Madsen IE, Marmot MG, Nielsen
ML, Nordin M, Oksanen T, Pentti J, Rugulies R, Salo P, Siegrist J, Singh-Manoux A,
Suominen SB, Väänänen A, Vahtera J, Virtanen M, Westerholm PJ, Westerlund H, Zins M,
Steptoe A Theorell T, IPD-Work Consortium (2012) Job strain as a risk factor for coronary
heart disease: a collaborative meta-analysis of individual participant data. Lancet 380,
1491–7.
- 6) Siegrist J (2008) Chronic psychosocial stress at work and risk of
depression: evidence from prospective studies. Eur Arch Psychiatry Clin Neurosci 258,
115–9.
- 7) Mäntyniemi A, Oksanen T, Salo P, Virtanen M, Sjösten N, Pentti J, Kivimäki
M, Vahtera J (2012) Job strain and the risk of disability pension due to musculoskeletal
disorders, depression or coronary heart disease: a prospective cohort study of 69,842
employees. Occup Environ Med 69, 574–81.
- 8) Virtanen M, Kurvinen T, Terho K, Oksanen T, Peltonen R, Vahtera J, Routamaa
M, Elovainio M, Kivimäki M (2009) Work hours, work stress, and collaboration among ward
staff in relation to hospital-associated infection among patients. Med Care 47,
310–8.
- 9) Hasson D, Gustavsson P (2010) Declining sleep quality among nurses: a
population-based four-year longitudinal study on the transition from nursing education to
working life. PLoS ONE 5, e14265.
- 10) Härmä M, Kompier MA, Vahtera J (2006) Work-related stress and health -risks,
mechanisms and countermeasures. Scand J Work Environ Health 32, 413–9.
- 11) Vahtera J, Pentti J, Helenius H, Kivimäki M (2006) Sleep disturbances as a
predictor of long-term increase in sickness absence among employees after family death or
illness. Sleep 29, 673–82.
- 12) Elovainio M, Ferrie JE, Gimeno D, De Vogli R, Shipley M, Brunner JE, Kumari
M, Vahtera J, Marmot MG, Kivimäki M (2009) Organizational justice and sleeping problems:
the Whitehall II study. Psychosom Med 71, 334–40.
- 13) Åkerstedt T (2006) Psychosocial stress and impaired sleep. Scand J Work
Environ Health 32, 493–501.
- 14) Hall M, Thayer JF, Germain A, Moul D, Vasko R, Puhl M, Miewald J, Buysse DJ
(2007) Psychological stress is associated with heightened physiological arousal during
NREM sleep in primary insomnia. Behav Sleep Med 5, 178–93.
- 15) Ekstedt M, Åkerstedt T, Söderström M (2004) Microarousals durinf sleep are
associated with increased levels of lipids, cortisol, and blood pressure. Psychosom Med
66, 925–31.
- 16) Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick P (1998) The
job content questionnaire (JCQ): an instrument for internationally comparative assessments
of psychological job characteristics. J Occup Health Psychol 3, 322–55.
- 17) Groeger JA, Zijlstra FR, Dijk D (2004) Sleep quantity, sleep difficulties
and their perceived consequences in a representative sample of some 2000 British adults. J
Sleep Res 13, 359–71.
- 18) Lallukka T, Rahkonen O, Lahelma E, Arber S (2010) Sleep complaints in
middle-aged women and men: the contribution of working conditions and work-family
conflicts. J Sleep Res 19, 466–77.
- 19) Kompier MA, Taris TW, van Veldhoven M (2012) Tossing and turning − insomnia
in relation to occupational stress, rumination, fatigue and well-being. Scand J Work
Environ Health 38, 238–46.
- 20) Kalimo R, Tenkanen L, Härmä M, Poppius E, Heinsalmi P (2000) Job stress and
sleep disorders: findings from the Helsinki Heart Study. Stress Med 16,
65–75.
- 21) Åkerstedt T, Torsvall L (1981) Shift work. Shift-dependent well-being and
individual differences. Ergonomics 24, 265–73.
- 22) Bonnefond A, Härmä M, Hakola T, Sallinen M, Kandolin I, Virkkala J (2006)
Interaction of age with shift-related sleep-wakefulness, sleepiness, performance, and
social life. Exp Aging Res 32, 185–208.
- 23) Härmä M (2006) Work hours in relation to work stress, recovery and health.
Scand J Work Environ Health 32, 502–14.
- 24) Rugulies R (2012) Studying the effect of the psychosocial work environment
on risk of ill-health: towards a more comprehensive assessment of working conditions.
Scand J Work Environ Health 38, 187–91.
- 25) Steinmetz H, Schmidt P (2010) Subjective health and its relationship with
working time variables and job stressors: sequence or general factor model? Work Stress
24, 159–78.
- 26) Alasaari JS, Lagus M, Ollila HM, Toivola A, Kivimäki M, Vahtera J, Kronholm
E, Härmä M, Puttonen S, Paunio T (2012) Environmental stress affects DNA methylation of a
CpG rich promoter region of serotonin transporter gene in a nurse cohort. PLoS ONE 7,
e45813.
- 27) Dohrenwend BS, Krasnoff L, Askenasy AR, Dohrenwend BP (1978) Exemplification
of a method for scaling life events: the Peri Life Events Scale. J Health Soc Behav 19,
205–29.
- 28) Smith CS, Reilly C, Midkiff K (1989) Evaluation of three circadian rhythm
questionnaires with suggestions for an improved measure of morningness. J Appl Psychol 74,
728–38.
- 29) Beck AT, Steer RA, Brown GK (1996) Manual for the beck Depression
Inventory-II. Psychological Corporation, San Antonio.
- 30) Astill RG, Verhoeven D, Vijzelaar RL, Van Someren EJ (2013) Chronic stress
undermines the compensatory sleep efficiency increase in response to sleep restriction in
adolescents. J Sleep Res (in press).
- 31) Wilkinson RT, Houghton D (1982) Field test of arousal: a portable reaction
timer with data storage. Hum Factors 24, 487–93.
- 32) Dinges DF, Pack F, Williams K, Gillen KA, Powell JW, Ott GE, Aptowicz C,
Pack AI (1997) Cumulative sleepiness, mood disturbance, and psychomotor vigilance
performance decrements during a week of sleep restricted to 4–5 hours per night. Sleep 20,
267–77.
- 33) Åkerstedt T (2003) Shift work and disturbed sleep/wakefulness. Occup Med
(Lond) 53, 89–94.
- 34) Kronholm E, Härmä M, Hublin C, Aro AR, Partonen T (2006) Self-reported sleep
duration in Finnish general population. J Sleep Res 15, 276–90.
- 35) Ruggiero JS, Redeker NS, Fiedler N, Avi-Itzhak T, Fischetti N (2012) Sleep
and psychomotor vigilance in female shift workers. Biol Res Nurs 14,
225–35.
- 36) Åkerstedt T, Ingre M, Broman JE, Kecklund G (2008) Disturbed sleep in shift
workers, day workers, and insomniacs. Chronobiol Int 25, 333–48.
- 37) Lin PC, Chen CH, Pan SM, Pan CH, Chen CJ, Chen YM, Hung HC, Wu MT (2012)
Atypical work schedules are associated with poor sleep quality and mental health in Taiwan
female nurses. Int Arch Occup Environ Health 85, 877–84.
- 38) Sallinen M, Kecklund G (2010) Work, sleep and sleepiness -differences
between shift schedules and systems. Scand J Work Environ Health 36,
121–33.
- 39) Åkerstedt T, Wright P (2009) Sleep loss and fatigue in shift work and shift
work disorder. Sleep Med Clin 4, 257–71.
- 40) Härmä M, Knauth P, Ilmarinen J (1989) Daytime napping and its effects on
alertness and short-term memory performance in shiftworkers. Int Arch Occup Environ Health
61, 341–5.
- 41) Tremaine R, Dorrian J, Paterson J, Neall A, Piggott E, Grech C, Pincombe J
(2013) Actigraph estimates of the sleep of australian midwives: the impact of shift work.
Biol Res Nurs 15, 191–9.
- 42) Ekstedt M, Söderstrom M, Åkerstedt T, Nilsson J, Søndergaard HP, Perski A
(2006) Disturbed sleep and fatique in occupational burnout. Scand J Work Environ Health
32, 121–31.
- 43) Mitler MM, Miller JC, Lipsitz JJ, Walsh JK, Wylie CD (1997) The sleep of
long-haul truck drivers. N Engl J Med 337, 755–61.
- 44) Morgenthaler T, Alessi C, Friedman L, Owens J, Kapur V, Boehlecke B, Brown
T, Chesson A Jr Coleman J, Lee-Chiong T, Pancer J, Swick TJ. Standards of Practice
Committee; American Academy of Sleep Medicine (2007) Practice parameters for the use of
actigraphy in the assessment of sleep and sleep disorders: an update for 2007. Sleep 30,
519–29.
- 45) Björkelund C, Bengtsson C, Lissner L, Rödström K (2002) Women’s sleep:
longitudinal changes and secular trends in a 24-year perspective. Results of the
population study of women in Gothenburg, Sweden. Sleep 25, 894–6.
- 46) Dorrian J, Paterson J, Dawson D, Pincombe J, Grech C, Rogers A (2011) Sleep,
stress and compensatory behaviors in Australian nurses and midwives. Rev Saude Publica 45,
922–30.
- 47) Takahashi M (2003) The role of prescribed napping in sleep medicine. Sleep
Med Rev 7, 227–35.
- 48) Takeyama H, Kubo T, Itani T (2005) The nighttime nap strategies for
improving night shift work in workplace. Ind Health 43, 24–9.
- 49) van der Hulst M (2003) Long working hours and health. Scand J Work Environ
Health 29, 171–88.
- 50) Vandekerckhove M, Weiss R, Schotte C, Exadaktylos V, Haex B, Verbraecken J,
Cluydts L (2011) The role of presleep negative emotion in sleep physiology.
Psychophysiology 48, 1738–44.
- 51) Loh S, Lamond N, Dorrian J, Roach G, Dawson D (2004) The validity of
psychomotor vigilance tasks of less than 10-minute duration. Behav Res Methods Instrum
Comput 36, 339–46.
- 52) Barr CD, Spitzmuller C, Stuebing KK (2008) Too stressed out to participate?
Examining the relation between stressors and survey response behavior. J Occup Health
Psychol 13, 232–43.
- 53) Ala-Mursula L, Vahtera J, Pentti J, Kivimäki M (2004) Effect of employee
worktime control on health: a prospective cohort study. Occup Environ Med 61,
254–61.