Abstract
During the past three decades, the participation of women in medicine has increased from 10.6% (1986) to 19.7% (2012) in Japan. However, women continue to be underrepresented in the top tiers of academic medicine. We highlight gender inequality and discuss the difficulties faced by female surgeons in Japanese academic surgery. Using anonymous and aggregate employment data of medical doctors at Kyoto University Hospital from 2009 and 2013, and a commercially-published faculty roster in 2012-2013, we compared gender balance stratified by a professional and an academic rank. The numbers of total and female doctors who worked at Kyoto University Hospital were 656 and 132 (20.1%) in 2009 and 655 and 132 (20.2%) in 2013, respectively. Approximately half the men (n = 281) were in temporary track and the rest (n = 242) were in tenure track, but only one fifth of women (n = 24) were in tenure track compared to 108 women in temporary track (p < 0.0001) in 2013. There were three female associate professors in basic medicine (8.1%), two female professors in clinical non-surgical medicine (3.9%) and one female lecturer in clinical surgical medicine (2.3%) in 2012. Fewer female doctors were at senior positions and at tenure positions than male doctors at Kyoto University Hospital. There were no female associate and full professors in surgery. The status of faculty members indicates the gender differences in leadership opportunities in Japanese academic surgery.
Introduction
During the past three decades, the participation of women in medicine has increased from 10.6% (1986) to 19.7% (2012) in Japan (Ministry of Health, Labour and Welfare of Japan 2012). Women represented 32.3% of all medical students in 2012, as compared with 25.2% in 1994 (Ministry of Education, Culture, Sports, Science and Technology of Japan 2013). Overall, 20% of practicing doctors in Japan are women, and women made up 15.1% of medical faculty members in 2012 (Ministry of Health, Labour and Welfare of Japan 2012). However, women continue to be underrepresented in the top tiers of academic medicine.
There is currently a disproportionately low ratio of female to male full professors (Yasukawa 2013), especially in the field of surgery in Japan (Kono et al. 2012). Women currently make up 2.5% (2/80) of medical school deans, and 2.6% of full professors in Japanese medical schools and university hospitals (Yasukawa 2013). In addition, there were only three female professors in breast surgery in 2011, but no female full professors in gastrointestinal surgery, thoracic surgery, cardiovascular surgery, or pediatric surgery in Japan (Kono et al. 2012).
On the other hand, some countries systematically gather and publish data on faculty ranks and promotions by gender in academic medicine. The Women in U.S. Academic Medicine Statistics and Medical School Benchmarking Report 2011-2012 showed that in 2012 the proportion of female full professors was 20% and that of female medical school deans was 12%. Additionally, 21% of surgical faculty and 9% of full professor in surgery are women (Association of American Medical Colleges 2012). In a survey of staffing levels of medical clinical academics in UK medical schools as of 31 July 2011, 42% of lecturers, 30% of senior lecturers, and 15% of professors were women. Timeline analysis since 2004, when gender data were first recorded, showed a yearly increase in the number and proportion of female clinical academics in UK medical schools (Medical Schools Council 2012). The other bulk of research on gender gap in academic medicine was based on these databases (Bickel et al. 2002; Jagsi et al. 2006; Kass et al. 2006; Taira et al. 2008; Ahmadiyeh et al. 2010; Isaac et al. 2010; Zhuge et al. 2011).
Recently female doctors’ break in their career because of pregnancy and childcare has been recognized as a social problem from the standpoint of shortage of doctors in Japan (Japan Medical Association 2009; Nomura et al. 2010; Yamazaki et al. 2011). However, due to the lack of a nation-wide level database like the Women in U.S. Academic Medicine Statistics and Medical School Benchmarking Report (Association of American Medical Colleges 2012) and a survey of staffing levels of medical clinical academics in UK medical schools (Medical Schools Council 2012), not much report is available on female career advancement in Japanese academic medicine. Additionally, few reports are available especially on female surgeons because of a paucity of female surgeons in Japan. However, there also appears to be a glass ceiling for female doctors seeking full professorships in Japanese academic medicine.
Here, we conducted this study to analyze the gender inequality in Japanese academic surgery. Our research hypothesis was that gender inequality is more apparent in Japan compared with other countries. Our study reported findings of gender gap at a single institution. We focused on one institution, Kyoto University Hospital, Kyoto, Japan, a national university hospital, because they permitted the use of reliable institutional data on gender, department, rank, and track.
Methods
Subjects and data collection
This study is a descriptive study based on anonymous and aggregate employment data of medical doctors who worked at Kyoto University Hospital in 2009 and 2013, and a commercially-published faculty roster of Kyoto University School of Medicine in 2012-2013. The anonymous and aggregate employment data of medical doctors obtained from the personnel section of Kyoto University Hospital in April 2013 included gender, professional rank and track (tenure track or temporary track) of medical doctors. The professional rank available from the 2009 personnel data included “professor”, “associate professor”, “lecturer”, and “assistant professor” and those available from the 2013 data included “residents” and “clinical fellows” in addition. In Japan, “lecturer” is a higher rank than “assistant professor”. We tallied the total number of males and females for each rank and track. There were both tenure and non-tenure tracks for assistant professors, lecturers, associate professors and professors. The selection procedure for faculty positions is essentially based on open competitive recruitment processes; however, there are no clearly stated rules regarding appointment and promotion. In the case of non-tenure tracks, they are employed for specific programs under limited-time contracts. The employment contract is for one to several years, and is renewable and promotable based on evaluation results.
We categorized all clinical fellows and residents into non-tenure track because they must renew their contract annually.
The faculty roster of Kyoto University Graduate School of Medicine was obtained from Iiku Kikan Meibo 2012-2013 (Meibo-hensyushitsu 2012), which contains personal names, affiliations (i.e., department), and three academic ranks (i.e., professor, associate professor, lecturer). We recorded the gender of a subject by initial inspection of his or her first name. For cases in which gender was not certain, attempts were made to discern the gender by visiting the department website. Kyoto University Graduate School of Medicine included 20 departments of basic medicine and 32 departments of clinical medicine. We defined 13 departments (i.e., Gastrointestinal Surgery; Hepato-billiary-pancreatic Surgery and Transplantation; Breast Surgery; Gynecology and Obstetrics; Urology; Cardiovascular Surgery; Thoracic Surgery; Plastic and Reconstructive Surgery; Ophthalmology and Visual Sciences; Otolaryngology, Head and Neck Surgery; Orthopedic Surgery; Oral and Maxillofacial Surgery; and Neurosurgery) as “clinical medicine (surgery)” and the other 19 clinical departments (i.e., Hematology and Oncology; Medicine and Clinical Science; Cardiovascular Medicine; Gastroenterology and Hepatology; Respiratory Medicine; Rheumatology and Clinical Immunology; Geriatric Medicine; Diabetes, Endocrinology and Nutrition; Pediatrics; Nephrology; Dermatology; Pediatrics; Radiation Oncology and Image-Applied Therapy; Diagnostic Imaging and Nuclear Medicine; Anesthesia; Clinical Laboratory Medicine; Clinical Molecular Biology; Neurology; Psychiatry) as “clinical medicine (non-surgery)”.
In accordance with the latest edition of the AMA Manual of Style (AMA Manual of Style Committee 2009), this study is based on anonymous and aggregate data, which does not permit the identification of study subjects, and therefore, may be exempt from review of ethics committee.
Statistical analyses
We calculated gender proportion according to each professional rank and compared the difference of gender proportion between 2009 and 2013 by using a chi-square or Fisher’s exact test. Next, where the personnel data in 2013 were stratified by track, we investigated the difference of gender proportion among the professional rank based on Fisher’s exact test. Using the same statistical method, we also compared gender proportion among three academic ranks stratified by the above mentioned three department groups.
All analyses were conducted using SAS software Version 9.12 (Cary, NC), and statistical significance was set at p < 0.05.
Results
The total numbers of medical doctors and female doctors who worked at Kyoto University Hospital were 656 and 132 (20.1%) in 2009 and 655 and 132 (20.2%) in 2013, respectively. The number of medical doctors who were ranked assistant professor or higher positions at Kyoto University Hospital was 348 (315 men vs. 33 women) in 2009 and 366 (326 men vs. 40 women) in 2013.
Table 1 shows the gender proportion between 2009 and 2013 according to each professional rank. In both 2009 and 2013, there was a very few number of women doctors in total who were ranked assistant professor or higher compared to men. The proportion of female doctors slightly increased from 2009 to 2013: assistant professor, 29 (13.4%) to 31 (13.5%); lecturer, 2 (3.0%) to 5 (7.8%); associate professor, 1 (3.2%) to 2 (5.4%); and professor, 1 (2.9%) to 2 (5.7%). However, these small changes were all non-significant due to the very small number.
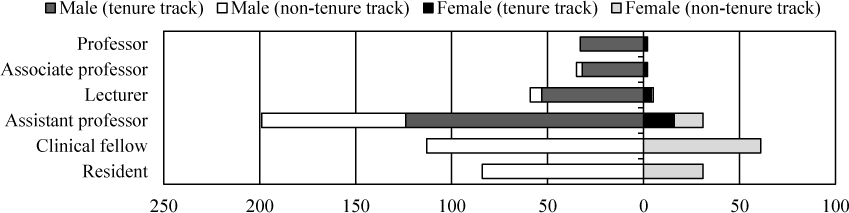
Fig. 1 shows gender proportion among professional ranks in 2013. The majority of medical doctors who worked in 2013 were male doctors. Approximately half the men (n = 281) were in temporary track and the rest (n = 242) in tenure track. On the other hand, only one fifth of total female doctors (n = 24) were in tenure track compared to 108 women in temporary track (p < 0.0001). Gender difference in professional ranks in tenure track was not significant due to the small number of women. Where stratified by tenure track, the number of female doctors among each professional rank was 2 (5.7%; 2/35) in professor, 2 (5.8%; 2/34) in associate professor, 4 (7.1%; 4/57) in lecturer, and 16 (11.4%; 16/140) in assistant professor. On the other hand, gender difference in temporary track was significant (p = 0.016 based on Fisher’s exact test); men were more likely to be ranked in higher positions in temporary track compared to women. Where stratified by temporary track, the number of female doctors was 0 (0%; 0/0) in professor, 0 (0%; 0/3) in associate professor, 1 (14%; 1/7) in lecturer, and 15 (17%; 15/90) in assistant professor, 61 (35.0%; 61/174) in clinical fellow, and 31 (27.0%; 31/115) in resident.
Fig. 2 shows gender proportion among three academic ranks according to three department groups. Across the department groups, the number of women was very few compared to that of men, which failed to reach statistical significance. There were only 3 female associate professors in basic medicine (8.1%; 3/37) and 2 female professors in non-surgical medicine (3.9%; 2/51) and only 1 female lecturer in surgical medicine (2.3%; 1/44). This means that there were no female professors/associate professors in surgical medicine.
Discussion
Our investigation into the status of male and female faculty members in one medical school indicated gender differences in leadership opportunities. There were very few female doctors at senior positions of Kyoto University Hospital. Among medical doctors who worked at Kyoto university Hospital, approximately half the men were in temporary track and the rest were in tenure track. On the other hand, only one fifth of total female doctors were in tenure track. In addition to gender inequality in employment track status, there were no female professors/associate professors in surgical medicine.
These differences support the widespread perception that academic medicine is not gender-blind and that the road to success is more challenging for women than for men in Japan. The results from previous studies conducted at US medical institutions in 1990-2003 (Nickerson et al. 1990; Hostler and Gressard 1993; Holmes-Rovner et al. 1994; Wright et al. 2003) and our findings of gender differences in rank were similar.
Reports by Yasukawa (2013) and Kono et al. (2012) emphasizing the paucity of females holding senior positions hold true universally in Japanese academic medicine, especially in surgery, and Kyoto University is not an exceptional case in Japan. Kyoto University, a national university, which is the second oldest university in Japan, is one of the highest ranked universities in Asia. Kyoto University is well known for producing world-class researchers, including the recent Nobel Prize winner, Shinya Yamanaka for induced pluripotent stem (iPS) cells. In these previous studies (Kono et al. 2012; Yasukawa 2013), it was not discussed whether the positions were tenured or temporary, but we showed gender difference in professional ranks in tenure track, and our study has novelty in this standpoint.
Unfortunately, females in each professional rank have not increased statistically between 2009 and 2013 and there were still very few females at professional ranks in both basic and clinical medicine (non-surgery and surgery) at Kyoto University. Kyoto University opened the Center for Women Researchers in September 2006, to provide an environment in which the abilities of women researchers are promoted as well as those of talented young researchers. Some female doctors at Kyoto University may have obtained considerable benefits from the center (e.g., baby care room or financial support to hire research/experiment assistants), however, the support might not demonstrate observable progress in female doctors’ career advance. There are similar support systems to help female researchers and medical doctors in several Japanese universities and colleges. We need to monitor the effect of such academic support for development of female doctors throughout Japan over the long term.
Kawase and Kayama (2009) reported three issues of women surgeons in Japan from survey conducted by the Japan Surgical Society; difficulty of program for board certification, barrier in career advancement and difficulty in balancing long working time and childcare.
Actually, although women represented 22% of new members of the Japan Surgical Society in 2007 (Tomizawa et al. 2011), only 5.2% of Board Certified Surgeons, who are certificated by Japanese Surgical Society, were woman in 2012 (Ministry of Health, Labour and Welfare of Japan 2012). Percentage of female board certified general thoracic surgeons, cardiovascular surgeons, and gastroenterological surgeons were 3.3%, 1.5% and 1.6%, respectively (Ministry of Health, Labour and Welfare of Japan 2012). In the United States (US) in 2008, women made up 21.3% of active physicians with surgical specialty and 37.5% of surgical residents and fellows (American College of Surgeons Health Policy Research Institute 2010). Additionally, the number of American Board of Surgery certificate holders in General Surgery who are women was 13.5% (Taira et al. 2008). In England in 2011, women made up only 10.6% of consultant surgeons, although 25.9% of surgeons were women. (Health and Social Care Information Centre 2012).
It is patently obvious that female surgeons are still in a minority and less certificated than males in Japanese surgery. Here, we consider that this “leaky pipeline” has shown that females still face significant obstacles when developing a successful career as a surgeon in clinical practice or seeking senior positions in academia, demonstrating the need for a re-focused examination of the work environment and culture surrounding female academics and doctors (especially surgeons).
Female surgeons were more likely to experience work-home conflicts than their male colleagues (Dyrbye et al. 2011). The highly important explanation for the paucity of women at higher ranks in Japan is that they are less committed to their careers because of family and other personal responsibilities. When it comes to the gender gap, Japan is in a highly unusual position. According to The Global Gender Gap Report, published by the World Economic Forum, although Japan ranks nearly at the top of the world in women’s education, health and survival, when it comes to economic participation and political empowerment, Japan is nearly at the bottom. In 2012, the Report ranked Japan at 101 out of 135 countries in the overall gender gap ranking (World Economic Forum 2012).
Japan is also well known for its strong gender division in employment and for its prominent “M curve” in the female labor force participation rate, reflecting the tendency of women to leave paid employment during their child-bearing years and return after their children have reached a certain age (Gender Equality Bureau Cabinet Office 2012). In Japan, the career paths of women follow an M-curve shape because there is a steady decline of women in the workforce from the ages of 25-34 (with the age brackets 20 to 24 and 45 to 49 being two peaks). This M-shaped pattern is unusual compared with women’s career paths in Western nations. Female doctors’ labor force participation rate by age group also shows an M-shaped curve that bottoms out when women are in their 30s (Health Policy Bureau, Ministry of Health, Labour and Welfare of Japan 2006), indicating that many female doctors stop working when they marry and have children.
According to a survey conducted by the Japan Surgical Society (The Committee for the Improvement in Work Environment of Surgeons 2013), surgeons at national university hospitals work an average of 98.1 hours per week. Working nearly 100 hours per week does not allow time for doctors to engage in housework and childcare themselves, thus requiring help from others. Many male doctors entrust these household chores to their wives who remain in the home full-time. In fact, in 2010 at Kyoto University Hospital, 55.1% of the wives of male doctors did not work outside of the home, while 83.3% of female doctors’ husbands were also doctors (Okoshi et al. 2013). Yasukawa and Nomura (2012) have indicated that women in medical practice may not work as many hours per week as males to spend more time (30 hours) doing unpaid domestic work than men (3 hours). Furthermore, surgeons tended to work more hours than non-surgeons at Kyoto University Hospital (Okoshi et al. 2012). Family responsibilities may also been attributed to leaving less time for academic activity. Therefore, we should shorten wholly the long hours of surgeons and support females to tolerate a certain level of long working time and develop a successful surgical career.
In western countries, several other possible reasons have been discussed why female medical doctors were represented in leadership position. Firstly, females might develop fewer publications than male colleagues. However, the gender difference in publication productivity is still highly controversial in US (Schroen et al. 2004; Housri et al. 2008; Taira et al. 2008), and we need to evaluate the gender difference in publication by Japanese surgeons. The second possible reason is sexual and gender discrimination or harassment. Unfortunately, gender-based harassment is highly prevalent in the surgical field (Komaromy et al. 1993; Schiffman and Frank 1995; Frank et al. 1998). Women in academic medicine, who experienced gender discrimination, reported lower levels of career satisfaction than did women who had not experienced discrimination (Carr et al. 1993). The third possible reason is lack of confidence of female surgeons. Several reports showed that female surgical residents (Minter et al. 2005) and students (Lind et al. 2002) tend to underestimate their abilities, although they perform better than men. Lind et al. (2002) described that women who are less confident about their performance on surgery may be less likely to pursue a career in surgery and these gender differences in self-assessment may be important to recognize when faculties provide feedback to students. The fourth possible reason is scarce mentorship. Effective mentors have many roles in the advancement of their mentees: they can act as role models, however, there is a lack of same-gender mentors and role models for women in both academic surgery and medicine (Zhuge et al. 2011). Female mentors were sought particularly for guidance on family or lifestyle issues or as role models (Kass et al. 2006).
The gap in the academic careers of females and males may not be unique to general surgery, but the low number of academic female surgeons might cause a lack of same-gender mentors and role models, resulting in a lower level of interest and a potential downward trend in this specialty among residents and medical students, more than 30% of whom are female in Japan. Improving these disparities in the university hospital may improve the recruitment and retention of competitive women to general surgery. Additionally, there is a report that collective intelligence, a kind of group intelligence, was correlated with the proportion of female in the group (Woolley et al. 2010). Those who work in teaching and medical research determine the content and priorities of future medicine. If more women work in these areas, it could at least be argued that they have some impact on the content of medical knowledge and medical education in the future (Riska 2001a). Furthermore, the sexism inherent in medicine, and in the diagnosis and treatment of women patients, will disappear as the profession changes from a male-dominated to a more female-dominated one (Riska 2001b). Promoting gender equality should be a key strategic priority for all academia.
Our study has several limitations. First, we were only able to collect data from a single institute, which may undermine generalizability. Nevertheless, the small percentage of women in higher academic positions was similar to nationwide rates reported by previous literatures (Kono et al. 2012; Yasukawa 2013). Second, although the counting method used in Iiku Kikan Meibo is widely accepted in Japanese academia, the requirements for positions and track differs depending on each university/college of medicine, which may induce misclassification. In this regard, our result of gender balance in each position and track may require careful interpretation. Third, because of a very few number of female medical doctors in Kyoto University, we were not able to conduct statistical comparison among clinical department groups. Therefore, our results do not provide an overview of the general issues that Japanese female doctors currently face. We did however, obtain reliable data on rank and track, and together with the results from the Kyoto University Hospital Survey for Doctors’ Work-Life Balance (Okoshi et al. 2013), we were able to discuss the realities of gender inequality faced by female doctors in Japan. Lastly, our data did not directly show that women surgical medical doctors give up their jobs at a higher ratio than non-surgical medical doctors. However, if the issue lies in the choice of the career of female doctors, the data indicate that women consider surgical career as an unattractive option because of the poor working conditions including long working hours, few mentors and the difficulties in balancing career success and family. Japanese female medical students and residents should be offered more affirmative and achievement-oriented role models and made to feel free to choose among different career options even in previously male-dominated professions.
Despite these limitations, this is the first survey to focus on the lack of women holding senior positions at academic medical institutions in Japan. Gender inequality is a very serious issue in every area throughout Japan, and therefore worthy of preliminary research to explore this important issue. There is a need for detailed Japanese data to address the lack of female leadership in Japanese academic medicine, and this report may serve as an important initial step.
In conclusion, our analysis shows that fewer female doctors were at senior positions and at tenured positions than males at Kyoto University Hospital. Further studies are required to monitor and support academic career development of female surgeons throughout Japan. Also, bringing change to this inequality will require persistent effort, continuous monitoring of progress and a commitment to diversifying faculty and leadership.
Acknowledgments
The authors’ deepest appreciation goes to Dr. Shigeo Hisamori, whose generous support was invaluable during the course of our study. We would also like to thank Katie Stallard for her assistance in writing this manuscript. Some of the information in this paper was presented as a poster at the 4th Annual International Women in Surgery Career Symposium, 7-9 June 2013, San Francisco.
Conflict of Interest
Authors declare no conflict of interest.
References
-
Ahmadiyeh,
N.,
Cho,
N.L.,
Kellogg,
K.C.,
Lipsitz,
S.R.,
Moore,
F.D. Jr.,
Ashley,
S.W.,
Zinner,
M.J. &
Breen,
E.M.
(2010) Career satisfaction of women in surgery: perceptions, factors, and strategies. J. Am. Coll. Surg., 210, 23-28.
-
AMA Manual of Style Committee
(2009) AMA Manual of Style: A Guide for Authors and Editors (10th edition).
-
American College of Surgeons Health Policy Research Institute
(2010) The Surgical Workforce in the United States: Profile and Recent Trends. http://www.acshpri.org/documents/ACSHPRI_Surgical_Workforce_in_US_apr2010.pdf [Accessed: September 11, 2014].
-
Association of American Medical Colleges
(2012) Women in U.S. Academic Medicine and Science: Statistics and Benchmarking Report 2011-2012. https://members.aamc.org/eweb/upload/Women%20in%20U%20S%20%20Academic%20Medicine%20Statistics%20and%20Benchmarking%20Report%202011-20123.pdf [Accessed: September 11, 2014].
-
Bickel,
J.,
Wara,
D.,
Atkinson,
B.F.,
Cohen,
L.S.,
Dunn,
M.,
Hostler,
S.,
Johnson,
T.R.,
Morahan,
P.,
Rubenstein,
A.H.,
Sheldon,
G.F. &
Stokes,
E.
(2002) Increasing women’s leadership in academic medicine: report of the AAMC Project Implementation Committee. Acad. Med., 77, 1043-1061.
-
Carr,
P.L.,
Friedman,
R.H.,
Moskowitz,
M.A. &
Kazis,
L.E.
(1993) Comparing the status of women and men in academic medicine. Ann. Intern. Med., 119, 908-913.
-
Dyrbye,
L.N.,
Shanafelt,
T.D.,
Balch,
C.M.,
Satele,
D.,
Sloan,
J. &
Freischlag,
J.
(2011) Relationship between work-home conflicts and burnout among American surgeons: a comparison by sex. Arch. Surg., 146, 211-217.
-
Frank,
E.,
Brogan,
D. &
Schiffman,
M.
(1998) Prevalence and correlates of harassment among US women physicians. Arch. Intern. Med., 158, 352-358.
-
Gender Equality Bureau Cabinet Office
(2012) Women and Men in Japan 2012. http://www.gender.go.jp/english_contents/pr_act/pub/pamphlet/women-and-men12/index.html [Accessed: September 11, 2014].
-
Health and Social Care Information Centre
(2012) NHS Staff — 2001-2011, Medical and dental, NHS Workforce: Summary of staff in the NHS: Results from September 2011 Census. http://www.hscic.gov.uk/searchcatalogue?productid=4876&q=title%3a%22nhs+staff%22+%26+title%3a%22medical+and+dental%22&sort=Relevance&size=10&page=1#top [Accessed: September 11, 2014].
-
Health Policy Bureau, Ministry of Health, Labour and Welfare of Japan
(2006) Ishi no jukyu ni kansuru kentokai hokokusho (Report of the Study Group on the Demand for Physician). http://www.mhlw.go.jp/shingi/2006/07/dl/s0728-9c.pdf [Accessed: September 11, 2014].
-
Holmes-Rovner,
M.,
Alexander,
E.,
O’Kelly,
B.,
Rome,
W.,
Wu,
S.M.,
Lovell,
K. &
Alfano,
M.
(1994) Compensation equity between men and women in academic medicine: methods and implications. Acad. Med., 69, 131-137.
-
Hostler,
S.L. &
Gressard,
R.P.
(1993) Perceptions of the gender fairness of the medical education environment. J. Am. Med. Womens Assoc., 48, 51-54.
-
Housri,
N.,
Cheung,
M.C.,
Koniaris,
L.G. &
Zimmers,
T.A.
(2008) Scientific impact of women in academic surgery. J. Surg. Res., 148, 13-16.
-
Isaac,
C.,
Griffin,
L. &
Carnes,
M.
(2010) A qualitative study of faculty members’ views of women chairs. J. Womens Health (Larchmt), 19, 533-546.
-
Jagsi,
R.,
Guancial,
E.A.,
Worobey,
C.C.,
Henault,
L.E.,
Chang,
Y.,
Starr,
R.,
Tarbell,
N.J. &
Hylek,
E.M.
(2006) The “gender gap” in authorship of academic medical literature: a 35-year perspective. N. Engl. J. Med., 355, 281-287.
-
Japan Medical Association: Nihon Ishikai Danjo Kyodo Sankaku Iinkai & Nihon Ishikai Ishi Saisyugyo Shien Jigyo
(2009) Josei ishi no kinnmu kankyo no genkyoni kansuru chosa houkokusho (Report on the working environment of female physicians in Japan). http://dl.med.or.jp/dl-med/teireikaiken/20090408_2.pdf [Accessed: September 11, 2014].
-
Kass,
R.B.,
Souba,
W.W. &
Thorndyke,
L.E.
(2006) Challenges confronting female surgical leaders: overcoming the barriers. J. Surg. Res., 132, 179-187.
-
Kawase,
K. &
Kayama,
M.
(2009) Issues of women surgeons in Japan. Nihon Geka Gakkai Zasshi, 110, 362-365.
-
Komaromy,
M.,
Bindman,
A.B.,
Haber,
R.J. &
Sande,
M.A.
(1993) Sexual harassment in medical training. N. Engl. J. Med., 328, 322-326.
-
Kono,
E.,
Yamasaki,
Y.,
Yasumasa,
K.,
Akamaru,
Y.,
Iwasaki,
T.,
Morimoto,
Y.,
Fujii,
M.,
Inada,
K. &
Yumiba,
T.
(2012) Current status and future outlook of women’s participation in surgical field. Nihon Geka Gakkai Zasshi, 113, 331-333 (in Japanese).
-
Lind,
D.S.,
Rekkas,
S.,
Bui,
V.,
Lam,
T.,
Beierle,
E. &
Copeland,
E.M. 3rd.
(2002) Competency-based student self-assessment on a surgery rotation. J. Surg. Res., 105, 31-34.
-
Medical Schools Council
(2012) A Survey of Staffing Levels of Medical Clinical Academics in UK Medical Schools as at 31 July 2011. http://www.medschools.ac.uk/Publications/Documents/MSC_Clinical_Academic_Staff_Survey_310711.pdf [Accessed: September 11, 2014].
-
Meibo-hensyushitsu
(2012) Iiku Kikan Meibo 2012-2013 (Roster of Academic Medicine in Japan), Yodosha, Tokyo, Japan, pp. 426-429.
-
Ministry of Education, Culture, Sports, Science and Technology of Japan
(2013) School Basic Survey. http://www.e-stat.go.jp/SG1/estat/NewList.do?tid=000001011528 [Accessed: September 11, 2014].
-
Ministry of Health, Labour and Welfare of Japan
(2012) Survey of Physicians, Dentists, and Pharmacists. http://www.e-stat.go.jp/SG1/estat/GL08020101.do?_toGL08020101_&tstatCode=000001030962&requestSender=dsearch [Accessed: September 11, 2014].
-
Minter,
R.M.,
Gruppen,
L.D.,
Napolitano,
K.S. &
Gauger,
P.G.
(2005) Gender differences in the self-assessment of surgical residents. Am. J. Surg., 189, 647-650.
-
Nickerson,
K.G.,
Bennett,
N.M.,
Estes,
D. &
Shea,
S.
(1990) The status of women at one academic medical center. Breaking through the glass ceiling. JAMA, 264, 1813-1817.
-
Nomura,
K.,
Yano,
E. &
Fukui,
T.
(2010) Gender differences in clinical confidence: a nationwide survey of resident physicians in Japan. Acad. Med., 85, 647-653.
-
Okoshi,
K.,
Tanabe,
T. &
Hisamoto,
N.
(2013) The Ideal Working Environment Required for a Successful Career Path and Work-Life Balance: Results of a survey on doctors working at Kyoto University Hospital. JMAJ, 56, 246-252.
-
Okoshi,
K.,
Tanabe,
T.,
Hisamoto,
N. &
Sakai,
Y.
(2012) Analyzing the attributes of surgeons and working environment required for a successful career path and work-life balance: results of a survey administered to doctors working at Kyoto University Hospital. Nihon Geka Gakkai Zasshi, 113, 334-339.
-
Riska,
E.
(2001a) Towards gender balance: but will women physicians have an impact on medicine? Soc. Sci. Med., 52, 179-187.
-
Riska,
E.
(2001b) Medical Careers and Feminist Agendas: American, Scandinavian, and Russian Women Physicians, Aldine De Gruyter, New York, NY.
-
Schiffman,
M. &
Frank,
E.
(1995) Harassment of women physicians. J. Am. Med. Womens Assoc., 50, 207-211.
-
Schroen,
A.T.,
Brownstein,
M.R. &
Sheldon,
G.F.
(2004) Women in academic general surgery. Acad. Med., 79, 310-318.
-
Taira,
B.R.,
Jahnes,
K.,
Singer,
A.J. &
McLarty,
A.J.
(2008) Does reported funding differ by gender in the surgical literature? Ann. Surg., 247, 1069-1073.
-
The Committee for the Improvement in Work Environment of Surgeons
(2013) Survey for Japanese surgeons work environment, Japan Surgical Society, Tokyo, Japan, p. 22.
-
Tomizawa,
Y.,
Kono,
E.,
Nomura,
S.,
Akashi,
S.,
Kawase,
K.,
Kanbayashi,
C. &
Yorozuya,
K.
(2011) Japanese women surgeons’ present and future: report of a survey on support environment and activities at facilities staffed with Japanese Surgical Society counselors. Nihon Geka Gakkai Zasshi, 112, 349-353.
-
Woolley,
A.W.,
Chabris,
C.F.,
Pentland,
A.,
Hashmi,
N. &
Malone,
T.W.
(2010) Evidence for a collective intelligence factor in the performance of human groups. Science, 330, 686-688.
-
World Economic Forum
(2012) The Global Gender Gap Report 2012 (pp.19) http://www3.weforum.org/docs/WEF_GenderGap_Report_2012.pdf [Accessed: September 11, 2014].
-
Wright,
A.L.,
Schwindt,
L.A.,
Bassford,
T.L.,
Reyna,
V.F.,
Shisslak,
C.M.,
St Germain,
P.A. &
Reed,
K.L.
(2003) Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad. Med., 78, 500-508.
-
Yamazaki,
Y.,
Kozono,
Y.,
Mori,
R. &
Marui,
E.
(2011) Difficulties facing physician mothers in Japan. Tohoku J. Exp. Med., 225, 203-209.
-
Yasukawa,
K.
(2013) Gender inequality in academic medicine in Japan. Med. Teach., 35, 700.
-
Yasukawa,
K. &
Nomura,
K.
(2012) The division of labor by sex among Japanese physicians. Igaku Kyoiku Zasshi, 43, 315-319.
-
Zhuge,
Y.,
Kaufman,
J.,
Simeone,
D.M.,
Chen,
H. &
Velazquez,
O.C.
(2011) Is there still a glass ceiling for women in academic surgery? Ann. Surg., 253, 637-643.