Abstract
Purpose: Japanese government has been promoted community-based integrated care systems which provide seamless community healthcare resources for elderly people. In this system, medical-dental collaboration and hospital-clinic collaboration play important roles. In this study, to understand the actual the situation, survey was conducted for the member of the Iwate Dental Association and analyzed the difficulty of the collaboration and the regional differences.
Materials and Methods: The questionnaires were distributed to 609 all members of Iwate Dental Association. Implementation of dental treatment for mentally handicapped patients, the experiences of dental treatment for patients with diseases, the experiences of participated in nutrition support team and dental rounds at the hospital, dental treatment after nutrition support team rounds, dental and oral care at the hospital or medical clinic, participated in a collaborative conference at the hospital were surveyed. Data were analyzed by item response theory and correspondence analysis.
Results: The 354 members retuned the questionnaire (collection rate was 58.1%). The 216/343 (61%) of dental clinic had experienced the dental treatment of the patients with mental handicap. Participation of nutrition support team and dental treatment after nutrition support ream round had high discrimination ability for the medical and dental collaboration. By the correspondence analysis, regional differences can be observed.
Conclusion: There were the regional differences in the supply of the medical-dental and hospital-clinic collaboration service in Iwate Prefecture. Providing information for the members of team approach may be one of the resolutions for the regional difference.
Introduction
In Japanese super-aging society, the Japanese Ministry of Health, Labour and Welfare have promoted community-based integrated care systems which provide seamless community healthcare resources for elderly people with chronic diseases and disabilities [1,2]. By 2025, with the purpose of maintaining the dignity of elderly people and supporting independent living, in the area where people can live as much as possible, people can continue their own life to the end of life. In Japan, dental treatments have been mainly supplied by private dental clinics. Hospital-clinic collaboration and medical-dental collaboration are important elements for the construction of community-based integrated care systems and promote the oral health of the elderly with chronic diseases and disabilities.
Japanese Medical Service Act obligated every prefecture to design medical care plan according to their own affairs for every five years. In this medical care plan, four diseases: cancer, cerebral apoplexy, acute myocardial infarction, diabetes, and mental disease, have been focused on planning a seamless care plan in the community. In this seamless care system, dentist plays an important role to promote the oral health and quality of life for the community dowelling patients. Accumulated evidence of the effect of oral care for diseases support the role of the dentist. The implementation of oral care is beneficial for the prevention of oral mucositis during chemotherapy, head, and neck radiation therapy, and hematopoietic stem cell transplantation [3]. Perioperative oral management reduces the risk of surgical site infection after colorectal cancer surgery and shortens postoperative hospital stay [4]. Starting professional oral care immediately after surgery and establishing effective self-care may be important to prevent postoperative complications in patients with esophageal cancer [5]. Periodontal disease exerted on the cardiovascular system health and diabetes [6,7,8]. Individuals with dementia living in special facilities have more oral health problems than individuals without dementia [9].
Iwate prefecture is located northeast of Japan. It has the second largest area in Japanese prefecture. Statistics Bureau, Ministry of Internal Affairs and Communications reported population density was 82.15/km2 at 2017. Most of the areas are a rural area. Therefore, access to the regional core hospital is one of the barriers. Under these conditions, to establish and promote primary health care system and regional comprehensive care system is important [10,11]. In "Health Iwate 21 plan (second stage)", the prevention of tooth loss and maintenance/improvement of the oral function of elderly people and prevention of periodontal disease for the patients with diabetes mellitus are listed as the basic direction. The basic stance of Iwate Health and Medical Plan for visiting home dental care, dental treatment and oral care should be carried out under medical-dental collaboration. Maintenance of oral function of elderly people and popularization and establishment of family dentists has been also the aim of Medical Plan of Iwate Prefecture. The Iwate Dental Association is promoting medical-dental collaboration by the collaboration with Iwate Prefecture Administration and Iwate Medical Association. However, according to the Interim report of Health Plan 21 Iwate, not all of the dental clinics work on these collaborations.
In this study, to understand the actual situation of the medical-dental collaboration and hospital-clinic collaboration, the survey was conducted for the member of Iwate Dental Association and analyzed the difficulty of the collaboration and the regional differences.
Materials and Methods
Study population
This study was a cross-sectional survey conducted using a self-administered postal questionnaire. The questionnaires were distributed to 609 all members of Iwate Dental Association.
Questionnaire
The questionnaire consisted of 61 major categories including demographic factors, scales of the dental clinic, visiting home dental treatment, medical-dental collaboration, and availability of services provided by Iwate Dental Association for the members. Among these items, the following items were used for the analysis; assignment in the branch, implementation of dental treatment for mentally handicapped patients (yes, no, could not cope with), experience of dental treatment for patients with diseases (cancer, palliative care, diabetes mellitus, heart disease, stroke, others). For the experience of participating in medical-dental collaboration was used following items; participated in nutrition support team (NST) and dental rounds at the hospital, dental treatment after NST rounds, dental and oral care at the hospital or medical clinic, participated in a collaborative conference at the hospital, and never participate in the medical-dental collaboration.
Data analysis
Cross tabulations were carried out for each item against the branches in Iwate Dental Association. Under the Item Response Theory (IRT) approach three parameters logistic model was applied [12,13,14,15]. Item difficulty, item discrimination and item information were calculated. Item response curve and item information curves were graphically illustrated. Analysis of IRT was performed by the R software with ltm and irtoys package. To visualize the relations, correspondence analysis was conducted. The results were expressed as biplot [16]. These analyses were conducted with IBM SPSS Statistics version 24 and IBM Amos 24 (IBM Inc., Tokyo, Japan).
Ethics statement
The study was carried out in compliance with the principles of the Helsinki Declaration. Informed written consent for publication was obtained from each subject when the questionnaires were returned. This study was approved by the Ethics Committee of Tsurumi University School of Dental Medicine (approval number: 430).
Results
The questionnaire was distributed for 609 all members of Iwate Dental Association and 343 retuned the questionnaire (Tables 1 and 2). Collection rate was 56.3%. For the medical-dental corporation, 217 (61.3%) dental clinics experienced the dental treatment of mentally-handicapped patients. Only 8 (2.3%) cannot cope with dental treatment for mentally-handicapped patients. As patients with cancer had many oral problems, intensive oral care is recommended before the operation. Salivary flow drastically decreased for the patients undertaken radiation therapy. Ministry of Health, Labour and Welfare consignment and registered the dentist who has certificated the dental treatment and oral care for the patients with cancer. The 237 (69.0%) dental clinics had experienced the dental treatment of patients with cancer. And most of the area, more than 60% of dental clinics initiative worked on the dental treatment of the patients with cancer.
Table 1
Experience of dental treatment for mentally handicapped patients
|
Experience of dental treatment for mentally handicapped patients |
Total |
| Yes |
No |
Could not cope with |
| Branch |
n |
% |
n |
% |
n |
% |
| Morioka |
66 |
59 |
45 |
40 |
1 |
1 |
112 |
| Iwate-Hachimantai |
10 |
48 |
11 |
52 |
0 |
0 |
21 |
| Miyako |
17 |
81 |
3 |
14 |
1 |
5 |
21 |
| Kamaishi |
5 |
71 |
2 |
29 |
0 |
0 |
7 |
| Toono |
6 |
60 |
4 |
40 |
0 |
0 |
10 |
| Shiwa |
9 |
69 |
3 |
23 |
1 |
8 |
13 |
| Hanamaki |
15 |
71 |
6 |
29 |
0 |
0 |
21 |
| Kitakami |
16 |
62 |
9 |
35 |
1 |
4 |
26 |
| Ousyu |
24 |
65 |
11 |
30 |
2 |
5 |
37 |
| Ichinoseki |
21 |
60 |
12 |
34 |
2 |
6 |
35 |
| Kesen |
14 |
64 |
8 |
36 |
0 |
0 |
22 |
| Kuji |
6 |
75 |
2 |
25 |
0 |
0 |
8 |
| Ninohe |
7 |
70 |
3 |
30 |
0 |
0 |
10 |
| Total |
216 |
63 |
119 |
35 |
8 |
2 |
343 |
As the number of patients under palliative care was small, dental clinics in most of the branches had not experienced the dental treatment of the patients under palliative care. However, 50% of the dental clinics in Hanamaki branch and 75% in Kitakami branch had experienced the treatment.
Every prefecture is obligated to plan hospital and health planning for every 5 years. In hospital and health planning, Regional alliances clinical path for the patients with diabetes are included. However, less than 20% of dental clinics in three areas had experienced dental treatment with diabetes and more than 40% of dental clinics in six areas had experienced. For the dental treatment of patients with heart disease, around 30% of dental clinics had experienced the dental treatment. The number of branches that more than 30% of dental clinics that experienced the dental treatment of the patients with stroke was only three.
Table 2
Experience of dental treatment for patients with diseases
| Branch |
Cancer |
Palliative care |
Diabetes mellitus |
Heart disease |
Stroke |
Others |
| n |
% |
n |
% |
n |
% |
n |
% |
n |
% |
n |
% |
| Morioka |
59 |
69.4 |
16 |
18.8 |
35 |
41.2 |
27 |
31.8 |
19 |
22.4 |
10 |
11.8 |
| Iwate-Hachimantai |
15 |
78.9 |
4 |
21.1 |
6 |
31.6 |
7 |
36.8 |
3 |
15.8 |
1 |
5.3 |
| Miyako |
19 |
95 |
2 |
10 |
4 |
20 |
7 |
35 |
4 |
20 |
0 |
0 |
| Kamaishi |
2 |
33.3 |
2 |
33.3 |
3 |
50 |
2 |
33.3 |
2 |
33.3 |
0 |
0 |
| Tono |
6 |
75 |
0 |
0 |
4 |
50 |
6 |
75 |
2 |
25 |
0 |
0 |
| Shiwa |
9 |
90 |
0 |
0 |
4 |
40 |
5 |
50 |
4 |
40 |
0 |
0 |
| Hanamaki |
17 |
85 |
10 |
50 |
3 |
15 |
5 |
25 |
4 |
20 |
2 |
10 |
| Kitakami |
22 |
91.7 |
18 |
75 |
12 |
50 |
11 |
45.8 |
9 |
37.5 |
5 |
20.8 |
| Oshu |
36 |
100 |
6 |
16.7 |
11 |
30.6 |
9 |
25 |
6 |
16.7 |
0 |
0 |
| Ichinoseki |
29 |
87.9 |
10 |
30.3 |
14 |
42.4 |
7 |
21.2 |
6 |
18.2 |
2 |
6.1 |
| Kesen |
10 |
62.5 |
5 |
31.3 |
7 |
43.8 |
6 |
37.5 |
4 |
25 |
0 |
0 |
| Kuji |
7 |
87.5 |
1 |
12.5 |
1 |
12.5 |
3 |
37.5 |
1 |
12.5 |
0 |
0 |
| Ninohe |
5 |
83.3 |
0 |
0 |
2 |
33.3 |
2 |
33.3 |
1 |
16.7 |
0 |
0 |
| Total |
236 |
81.1 |
74 |
21.5 |
106 |
30.9 |
97 |
28.3 |
65 |
19 |
20 |
5.8 |
Table 3
Experience of medical-dental collaboration
| Category |
1 |
2 |
3 |
4 |
5 |
| Branch |
n |
% |
n |
% |
n |
% |
n |
% |
n |
% |
| Morioka |
15 |
13.9 |
11 |
10.2 |
28 |
25.9 |
22 |
20.4 |
46 |
42.6 |
| Iwate-Hachimantai |
1 |
4.8 |
2 |
9 |
5 |
23.8 |
12 |
57.1 |
14 |
66.7 |
| Miyako |
3 |
13.6 |
2 |
9.1 |
10 |
45.5 |
11 |
50 |
17 |
77.3 |
| Kamaishi |
9 |
100 |
5 |
55.6 |
3 |
33.3 |
4 |
44.4 |
9 |
100 |
| Toono |
2 |
20 |
1 |
10 |
2 |
20 |
3 |
30 |
5 |
50 |
| Shiwa |
3 |
23.1 |
0 |
0 |
5 |
38.5 |
5 |
38.5 |
6 |
46.2 |
| Hanamaki |
20 |
95.2 |
13 |
61.9 |
13 |
61.9 |
9 |
42.9 |
21 |
100 |
| Kitakami |
20 |
76.9 |
15 |
57.7 |
14 |
53.8 |
16 |
61.5 |
22 |
84.6 |
| Ousyu |
33 |
86.8 |
16 |
42.1 |
15 |
39.5 |
13 |
34.2 |
36 |
94.7 |
| Ichinoseki |
7 |
18.9 |
6 |
16.2 |
13 |
35.1 |
14 |
37.8 |
22 |
59.5 |
| Kesen |
13 |
59.1 |
6 |
27.3 |
7 |
31.8 |
11 |
50 |
17 |
77.3 |
| Kuji |
0 |
0 |
0 |
0 |
2 |
25 |
5 |
62.5 |
6 |
75 |
| Ninohe |
9 |
81.8 |
6 |
54.5 |
4 |
36.4 |
5 |
45.5 |
10 |
90.9 |
| Total |
135 |
39.3 |
83 |
24.1 |
121 |
35.3 |
130 |
37.9 |
231 |
67.3 |
Category:
1) Participated in NST and dental rounds at the hospital;
2) Dental treatment after NST rounds;
3) Dental and oral care at hospital or medical clinic;
4) Participated in a collaborative conference at hospital;
5) Never participate in medical-dental collaboration.
NST, Nutrition support team
Table 4
Three parameter logistic model for medical-dental collaboration
(A) Experience of dental treatment for patients with diseases (B) Experience of medical-dental collaboration
|
Discrimination |
Difficulty |
Guessing |
| Mentally handicapped patients |
12.27 |
1.25 |
0.3 |
| Cancer |
4.24 |
1.38 |
0.26 |
| Palliative care |
0.62 |
−2.3 |
0.01 |
| Diabetes mellitus |
1.73 |
−0.72 |
0.00002 |
| Heart disease |
3.22 |
−0.66 |
0.00001 |
| Stroke |
4.76 |
−0.95 |
0.00006 |
| Others |
0.29 |
−9.75 |
0.04791 |
| Category |
Discrimination |
Difficulty |
Guessing |
| 1 |
16.95 |
0.94 |
0.21 |
| 2 |
12.76 |
0.92 |
0.03 |
| 3 |
1.63 |
0.59 |
0.0003 |
| 4 |
1.02 |
0.68 |
0.01 |
Category for (B):
1) Participated in NST and dental rounds at the hospital;
2) Dental treatment after NST rounds;
3) Dental and oral care at hospital or medical clinic;
4) Participated in a collaborative conference at hospital.
NST, Nutrition support team
Table 3 shows the experience of the medical-dental corporation of the dental clinics by the branch. Large regional differences existed. Less than 10% of dental clinics in four branches experienced attendance in NST team rounds and dental practice after NST rounds. More than 50% of dental clinics in six branches experienced attendance in NST team rounds. The 231 (67.3%) dental clinics did not experience the medical-dental corporation. The rate of without experience was varied from 43.6% to 100% by the branch.
To evaluate the difficulty to participate in the medical-dental collaborations, three parameters logistic analysis by Item Response Theory (IRT) approach were carried out. The models constructed are shown in Table 4 (A) for the dental treatment for the patients with diseases and Table 4 (B) for the participation of medical-dental collaborations.
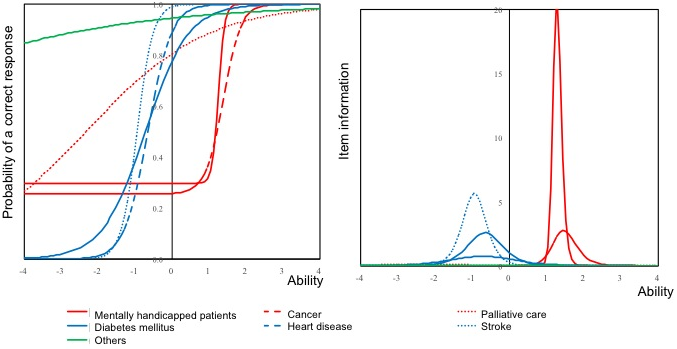
Fig. 1
Item response curves and Item information curves for the experience of dental treatment for patients with diseases
Response scores were standardized from -4 to 4. Steep slope indicates high discrimination ability.
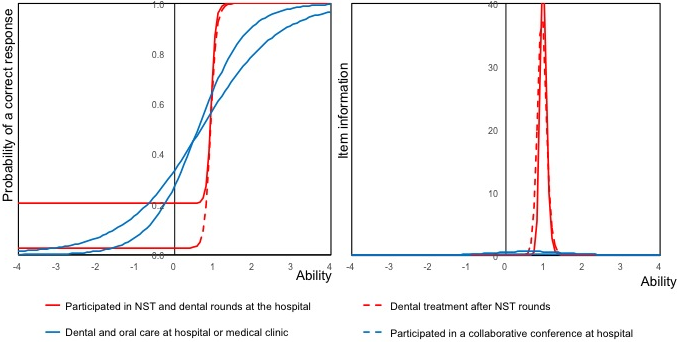
Fig. 2
Item response curves and Item information curves for the experience of medical-dental collaborations
The item response curves and item information curves are shown in Figs. 1 and 2. The item response curve of the dental treatment of the mentally handicapped patients and cancer showed a similar pattern and the item response curves of cancer, heart disease, and stroke showed a similar pattern. The item response curve of the dental treatment of patients with palliative care showed a loose slope. From the item information curve of the mentally handicapped patient, implementation of dental treatment of mentally handicapped patient clearly distinguish the high levels of participation of medical-dental collaborations.
For the difficulty of the participation in medical-dental collaborations, item response curves of participated in NST and dental rounds at the hospital and dental treatment after NST rounds showed steep curves. The item information curves of these participation showed sharp slopes. The item response curves of dental and oral care at the hospital or medical clinic and participated in a collaborative conference at the hospital showed loose slopes.
Fig. 3
Biplot of the branches of Iwate Dental Association and experience of dental treatment for the patients with diseases (left)
Regional differences were visualized by correspondence analysis and biplot. Red diamonds indicate the branch of Iwate Dental
Association and the blue circles indicate the experience of dental treatment for patients with diseases.
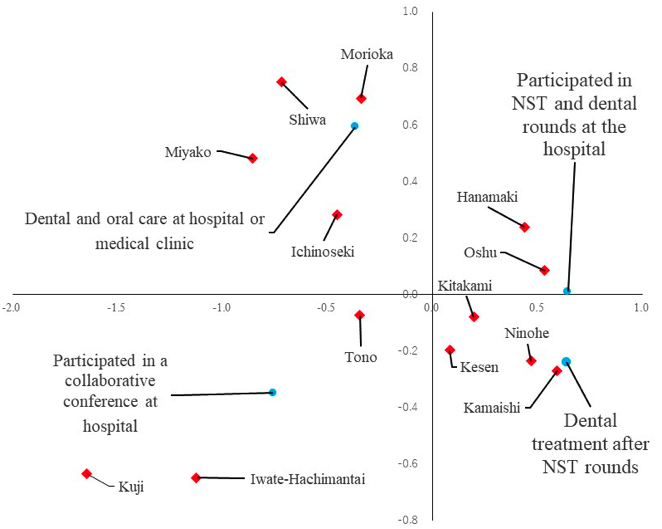
Fig. 4
Biplot of the branches of Iwate Dental Association and experience of medical-dental collaborations (right)
Red diamonds indicate the branch of Iwate Dental Association, and blue circles indicate experience of medical-dental collaboration.
Figure 3 shows the biplot by the diseases and blanches. The regional difference could be observed for the diseases. Figure 4 shows the biplot of the experience of medical-dental collaboration by the branch. There were branches that advanced in NST collaboration, advanced in visiting dental care for the hospital and advanced in joint training with hospitals.
Discussion
In this study, difficulty and regional differences in medical-dental collaboration and hospital-clinic collaborations in Iwate prefecture were analyzed. Clear regional differences could be observed. For the difficulty of dental treatment of the patient with diseases, dental treatment of the patients with mentally handicapped patients and cancer were a difficult treatment. There are many barriers including human resources for dental treatment of the patients with mentally handicapped patients [17,18,19]. There are many problems of oral health inpatient with cancer [20]. For the dental treatment and oral care for patients with cancer, Ministry of Health, Labour and Welfare consignment and registered the dentist who is certificated. These facts may lead to the difficulty of the dental treatment of these two diseases. However, Y values of mentally handicapped patients and cancer against −4 of X value was 0.3. It indicated that 30% of dental clinics that had almost no approach for medical-dental collaborations experienced dental treatment for these two diseases. The Y value of patients with palliative care against −4 of X value was also 0.3 and the slope of it was loose. It indicated patients who need palliative care continuously attend or returned to their family dentist. It suggested that the system of family dentist works.
For the medical-dental collaboration, the Y value of item response curve of participated in NST and dental rounds at the hospital against −4 was 0.2 and it continues to more than 0 value of X value. It indicated that there may be some dental clinics that only to attend the round. The intercept of item response curves was less than 0.4. It indicated that 40% of average levels for medical-dental collaboration tried no approach.
In Iwate prefecture, which has the second largest area in Japanese prefecture, the regional difference in the supply of medical and dental services mainly derived from the difference of medical resources. The number of regional core hospital in Iwate prefecture is 20 hospitals and 6 medical centers, which is highest in Japan. However, there is a large difference in their scales. The differences were derived from the unbalance of human resources. It resulted in the number of the medical department in the hospital and with or without regional collaboration center. For the supply of dental services, the services supplied varied between the dental clinics. Therefore, the dentist who participates in the medical-dental collaboration is fixed. However, according to the Interim report of Health Plan 21 Iwate, the major problem is the number of dentists is unbalanced between the areas.
For the areas that without dental department in regional core hospital, dental clinics need close collaboration with regional core hospital. There are three types of collaborations: dentist participates in the NST, visiting dental treatment and oral care for the inpatients in the hospital, and dental treatment and oral care before and after hospitalization. For the participation in NST, the dentist needs to understand the nursing and nutrition by on-the-job training. Training of the dentist is important to participate in the team approach. For visiting dental treatment and oral care for the inpatients, calibration between dentists is important. In some cases, the dentist needs to care of the patients after hospitalization. The dentist needs collaboration concerning the whole health control. For dental treatment and oral care before and after hospitalization, to control the team approach is important. Dentist needs collaboration with not an only the hospital but also the family of the patients. In addition, if the nursing care is necessary at home, collaboration with visiting nurse and care manager is also necessary. To establish the system including education and training of the dentist may be one of the resolutions of the regional difference.
Dental care for patients with palliative care was advanced in two branches. There may be two major reasons for advancement. One is the medical doctors’ understanding of the importance of dental care for patients with palliative care. The hospital that the medical doctor who understands the importance of dental care, dentist participates in the NST and visiting dental treatment and oral care for the inpatients in the hospital were already implemented. According to the Interim report of Health Plan 21 Iwate, another reason was that there were some areas that the regional core hospital did not set the palliative care ward. Moreover, in the regional core hospital that newly set the palliative care ward, the medical doctor often lacks the understanding of dental care for the patients need palliative care. It led to the basic concept of the home dentist. To provide the information for medical doctor may be one of the resolutions for the dissemination of dental treatment and oral care for the patients under palliative care.
In conclusion, there were the regional differences in the supply of the medical-dental and hospital-clinic collaboration service in Iwate prefecture. Providing information for the members of team approach may be one of the resolutions for the regional difference.
Acknowledgment
This work was supported by the annual fund of Iwate Dental Association.
Conflict of Interest
The authors declare no conflict of interest exists.
References
- 1) Marshall AC, Cooper NR. The association between high levels of cumulative life stress and aberrant resting state EEG dynamics in old age. Biol Psychol 2017; 127: 64-73. Arai H, Ouchi Y, Toba K, Endo T, Shimokado K, Tsubota K, et al. Japan as the front-runner of super-aged societies: Perspectives from medicine and medical care in Japan. Geriatr Gerontol Int 2015; 15: 673-87.
- 2) Hatano Y, Matsumoto M, Okita M, Inoue K, Takeuchi K, Tsutsui T, et al. The vanguard of community-based integrated care in Japan: The effect of a rural town on national policy. Int J Integr Care 2017; 17: 2.
- 3) Hong CHL, Gueiros LA, Fulton JS, Cheng KKF, Kandwal A, Galiti D, et al. Mucositis Study Group of the Multinational Association of Supportive Care in Cancer/International Society for Oral Oncology (MASCC/ISOO). Systematic review of basic oral care for the management of oral mucositis in cancer patients and clinical practice guidelines. Support Care Cancer. 2019.
- 4) Nobuhara H, Yanamoto S, Funahara M, Matsugu Y, Hayashida S, Soutome S, et al. Effect of perioperative oral management on the prevention of surgical site infection after colorectal cancer surgery: A multicenter retrospective analysis of 698 patients via analysis of covariance using propensity score. Medicine (Baltimore) 2018; 97: e12545.
- 5) Inai Y, Nomura Y, Takarada T, Yamazoe J, Hidaka K, Hanada N, et al. Risk factors for postoperative complications in patients with esophageal cancer receiving perioperative oral management. J Dent Oral Care 2018; 4: 40-6.
- 6) Simpson TC, Weldon JC, Worthington HV, Needleman I, Wild SH, Moles DR, et al. Treatment of periodontal disease for glycaemic control in people with diabetes mellitus. Cochrane Database Syst Rev 2015; 11: CD004714.
- 7) Pérez-Losada FL, Jané-Salas E, Sabater-Recolons MM, Estrugo-Devesa A, Segura-Egea JJ, López-López J. Correlation between periodontal disease management and metabolic control of type 2 diabetes mellitus. A systematic literature review. Med Oral Pathol Oral Cir Bucal 2016; 21: e440-6.
- 8) Liccardo D, Cannavo A, Spagnuolo G, Ferrara N, Cittadini A, Rengo C, et al. Periodontal disease: A risk factor for diabetes and cardiovascular disease. Int J Mol Sci 2019; 20: pii: E1414.
- 9) Rejnefelt I, Andersson P, Renvert S. Oral health status in individuals with dementia living in special facilities. Int J Dent Hyg 2006; 4: 67-71.
- 10) Stuart J, Hoang H, Crocombe L, Barnett T. Relationships between dental personnel and non-dental primary health care providers in rural and remote Queensland, Australia: dental perspectives. BMC Oral Health. 2017; 17: 99.
- 11) Santos TP, Matta Machado ATG, Abreu MHNG, Martins RC. What we know about management and organisation of primary dental care in Brazil. PLoS One 2019; 14: e0215429.
- 12) Rizopoulos D. ltm: An R package for latent variable modeling and item response theory analyses. J Stat Softw 2006; 17: 1-25.
- 13) Reis CMRD, Mambrini JVM, da Matta-Machado ATG, Amaral JHLD, Werneck MAF, Abreu MHNG. Primary dental care evaluation in Brazil: an item response theory approach. J Public Health Dent 2017; 77: 317-24.
- 14) Nomura Y, Matsuyama T, Fukai K Okada A, Ida M, Yamauchi N, et al. PRECEDE-PROCEED model based questionnaire and saliva tests for oral health checkup in adult. J Oral Sci 2019; 61: 544-8.
- 15) Nomura Y, Maung K, Kay Khine EM, Sint KM, Lin MP, Win Myint MK, et al. Prevalence of dental caries in 5- and 6-year-old Myanmar children. Int J Dent 2019; 5948379.
- 16) Nomura Y, Okada A, Miyoshi J, Mukaida M, Akasaka E, Saigo K, et al. Willingness to work and the working environment of Japanese dental hygienists. Int J Dent 2018; 2727193.
- 17) Wilson KI. Treatment accessibility for physically and mentally handicapped people--a review of the literature. Community Dent Health 1992; 9: 187-92.
- 18) Milnes AR, Tate R, Perillo E. A survey of dentists and the services they provide to disabled people in the Province of Manitoba. J Can Dent Assoc 1995; 61: 149-52.
- 19) Waldman HB, Perlman SP. What about dental care for people with mental retardation? A commentary. J Am Coll Dent 2002; 69: 35-8.
- 20) Reis CMR, Matta-Machado ATG, Amaral JHL, Mambrini JVM, Werneck MAF, de Abreu MHNG. Understanding oral health care team performance in primary care: A mixed-method study. PLoS One 2019; 14: e0217738.