Brief Communications
Two cases of large bregmatic bone along with a persistent metopic suture from necropoles on the northern Black Sea coast of Bulgaria
2016 Volume 124 Issue 2 Pages 145-153

Details
2016 Volume 124 Issue 2 Pages 145-153
The co-occurrence of a bregmatic bone and metopism is an extremely rare finding. In the present study we investigate, compare, and describe this uncommon combination in two skulls of a child and an adult male. Both samples were from the osteological collection of the Institute of Experimental Morphology, Pathology and Anthropology with Museum, Bulgarian Academy of Sciences. The skulls were obtained from archaeological excavations of two necropoles located on the northern Black Sea coast of Bulgaria. The samples were macroscopically observed and measured. A CT scan was also performed in order to investigate the internal structure and the relation between the calvarial bones. Both bregmatic bones were slightly prominent unpaired structures wedged into the frontal and parietal bones with a developed diploic space. In the child, the frontal sinus was underdeveloped, whereas in the adult the frontal sinuses were well developed on both sides of the metopic suture. In the latter, an osteoma on the left side of the sinus was observed. The retention of the metopic suture along with the formation of a bregmatic bone could be considered as indispensable accessory sites for the regulation of the bone growth as a response to the increasing brain mass requirements under specific circumstances. This could be a mechanism for maintaining the optimal balance between the calvarial shape and size for a maximal effectiveness and stability in the presence of some developmental abnormalities.
The concept of wormian bones includes all supernumerary bones in the neurocranium located between the calvarial bones, along the sutures or filling in the fontanelles. It has been supposed that they are designed to strengthen the cranium due to an insufficiency of the normal ossification centres (Parker, 1905). They are also considered as a response to mechanically induced factors which widen the sutures and affect the dural strain within the sutures and fontanelles (Sanchez-Lara et al., 2007). The fonticullar and sutural wormian bones are independent formations (Barberini et al., 2008) and appear as isolated ectopic islands of intramembranous ossification (Jeanty et al., 2000), whereas others such as Inca bone are a consequence of primary ossification centre fragmentation (Cremin et al., 1982; Nikolova et al., 2014a). Wormian bones are considered ‘normal’ or innocuous variations but in certain circumstances they could be an indicator for some congenital pathological conditions (Cremin et al, 1982; Nikolova et al, 2014b).
The bregmatic bone is a wormian bone occupying the anterior fontanelle. It represents a slightly elevated bone plate (Graham, 2007) which is initially flat and does not develop a diploic space as early as do the surrounding bones (Girdany and Blank, 1965), at about six years of age (Tubbs et al., 2012). The formation of a bregmatic bone occurs before birth or later in infancy from an additional ossification centre(s), which usually grows centrifugally and fuses in a variable sequence with the centripetally growing edges of the parietal and frontal bones before the age of five (Girdany and Blank, 1965). If the fusion fails, the bregmatic bone persists in adults as a supernumerary bone with rectangular, rhomboidal, triangular, or oval shape but more commonly with a rounded outline (Kadanoff and Mutafov, 1984). The reported frequency of a bregmatic bone in different population groups ranges from 0.2% to 2.5% (Parker, 1905; Berry and Berry, 1967; Berry, 1975; Kadanoff and Mutafov, 1984; Hauser and De Stefano, 1989), but in other groups it is not found at all (Akabori, 1933; Berry and Berry, 1967; Hauser and De Stefano, 1989; O’Loughlin, 2004). The reported cases of bregmatic bone in Bulgaria show a frequency of 1.16% among a series of contemporary adult male skulls (Kadanoff and Mutafov, 1984), a frequency of 1.25% in a medieval series of male skulls, and are entirely absent in a medieval female series (Nikolova and Toneva, 2014).
Metopism is a condition observed in adults, in which the frontal bone is composed of two symmetrical halves joined in the midline by an entirely preserved metopic suture. It is not established whether metopism is related to skull shape or to cranial capacity but it is positively correlated with an increase of the frontal curvature (Scheuer and Black, 2004). The presumptive factors causing metopism are heterogeneous and include an abnormal growth of the cranial bones, hydrocephalus, growth retardation, heredity and heredospecific factors, sexual influence, atavism, stenocrotaphia, plagiocephaly, scaphocephaly, mechanical causes, and hormonal dysfunction (Del Sol et al., 1989). The preserved metopic suture was found to range from 0.8% up to 15% in different population groups (Bryce, 1915; Limson, 1924; Jit and Shah, 1948; Keith, 1948; Woo, 1949; Torgersen, 1950; Breathnach, 1958; Romanes, 1972; Das et al., 1973; Berry and Berry, 1967; Berry, 1975; Agarwal et al., 1979; Ajmani et al., 1983; Del Sol et al., 1989; Baaten et al., 2003; Castilho et al, 2006; Eroğlu, 2008; Hussain Saheb et al., 2010; Murlimanju et al., 2011; Chakravarthi and Venumadhav, 2012).
In the relevant literature, few cases of a large bregmatic bone along with a metopic suture have been reported (Hauser and De Stefano, 1989; Becker, 2003; Radović and Miladinović-Radmilović, 2013). The goal of this study was to investigate two cases showing this rare combination. We aimed to demonstrate the macro- and microscopic appearance of the calvarial bones in these cases. Since the first sample was from a child, while the second one was from an adult male, we had the opportunity to compare and describe the presence of these traits in both developing and adult skulls.
The objects of the present study were two skulls possessing large bregmatic bones along with metopic sutures. Both samples are part of the osteological collection of the Institute of Experimental Morphology, Pathology and Anthropology with Museum, Bulgarian Academy of Sciences. The skulls were obtained during archaeological excavations of two necropoles located on the northern Black Sea coast of Bulgaria. The first sample was from the necropolis of Kavarna, dated to the 15th–17th centuries AD (Boev et al., 1982), i.e. the Ottoman period in Bulgaria. It represents an entirely preserved skull (Figure 1) without a mandible and postcranial skeleton. The second sample was from the medieval necropolis in the residential district of Troshevo of the city of Varna, dated to the 10th century AD. The sample represents a well-preserved calvaria without an occipital bone, but with two separate wormian bones: a large one located in the lambda region and a smaller sutural one probably located along the lambdoid suture (Figure 2). The right temporal squama with the zygomatic process was also preserved (Figure 3a). The left zygomatic bone and parts from the left maxilla and the mandibular body were present as well (Figure 3b, d). As for the postcranial skeleton, only the lengths of the right humerus (338 mm) and ulna (292 mm) were documented, but the bones were not available.
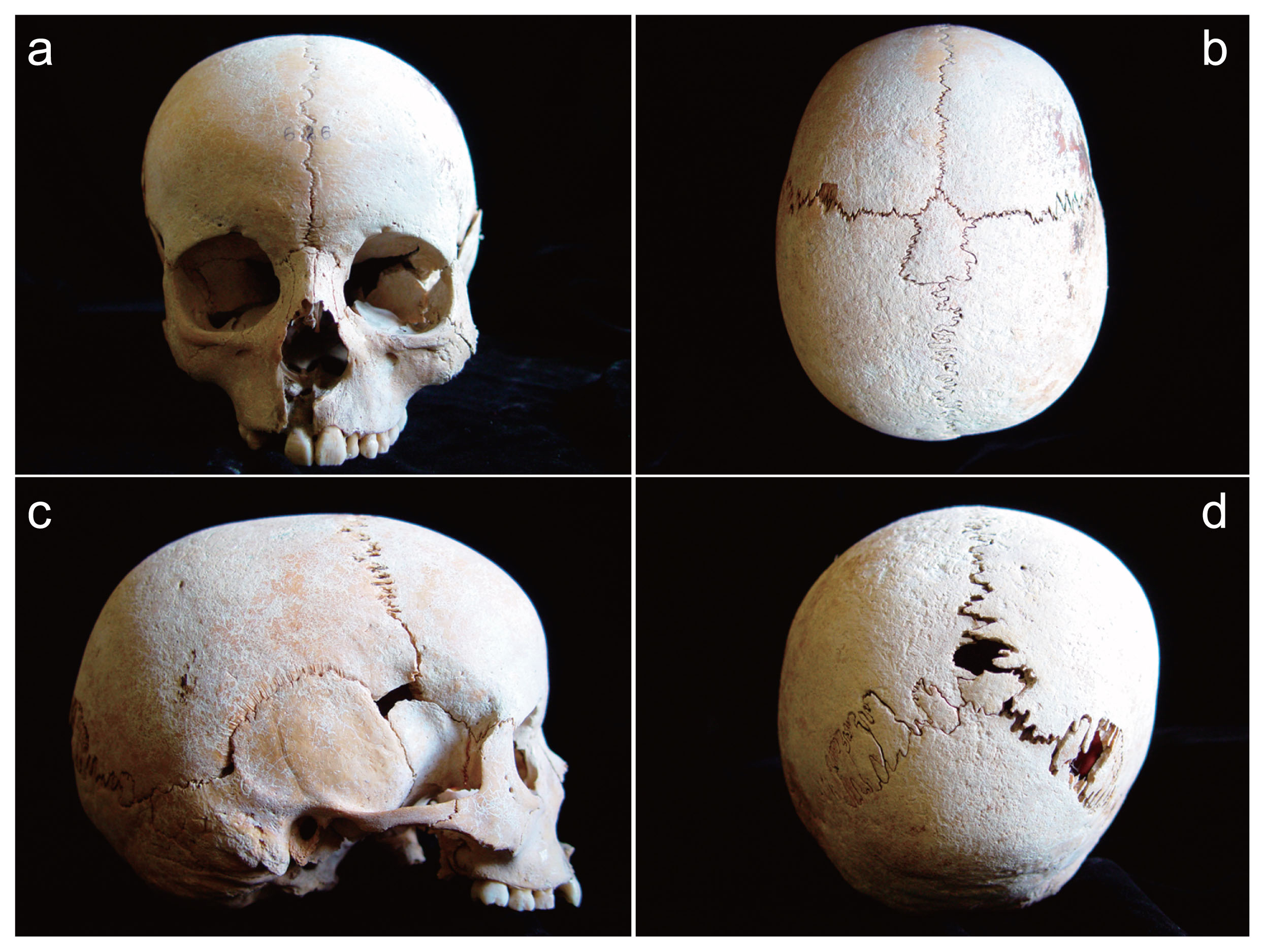
Views of the child skull: (a) frontal; (b) parietal; (c) lateral; (d) occipital.

Views of the adult calvaria: (a) parietal; (b) endocranial; (c) left lateral; (d) separated wormian bones.

Bone fragments from the adult skull: (a) right temporal squama; (b) left maxilla and zygomatic bone; (c, d) views of the mandibular part. Scale bars = 1 cm.
The physiological age of the child was determined according to dental eruption and cranial bone development (Scheuer and Black, 2000; Işcan and Steyn, 2013). Sex and age of the adult were determined based on the morphological features of the skull, the sutural obliterations, and the degree of dental attrition of the preserved teeth (Buikstra and Ubelaker, 1994; Işcan and Steyn, 2013).
Both samples were macroscopically observed and described. The measurements of the bregmatic bone and metopic suture were taken with a sliding caliper and a measuring tape. A computed tomography (CT) scan was applied in order to visualize the internal bone structure and organization, the development and thickness of the diploic space, the relation between bregmatic bone, metopic suture and the surrounding calvarial bones, the frontal sinus development and the structure of the sclerotic lesion in the frontal sinus of the adult. The CT scanning was performed on a Nikon XT H 225 system with reflection head and a voltage of 80 kV with a power of 6.8 W and 85 μA tube current. To generate a 3-D CT volume, a series of sequential 2-D X-ray images (projections) were captured as the object was rotated through 360°. For each scan 3000 projections were registered, where each projection was taken with an exposure time of 1000 ms. The images were then reconstructed to generate a 3-D volumetric representation of the object with voxel size of 98 μm. For 3-D visualization, VG Studio Max 2.2 software was used (Figure 4).

3-D volumetric representations: (a–d) of the child skull; (e–g) of the adult calvaria.
The first sample corresponded to a child of about 7–8 years of age. The second one was determined to belong to an adult male of about 25–35 years of age. The samples did not show any evident pathological alterations.
Macroscopic observationBoth individuals showed a large supernumerary bregmatic bone on the exo- and endocranial surfaces of the skull. The bregmatic bone of the child had an irregular pentagonal outline, while the bone in the adult had a regular rhomboid shape occupying exactly the anterior fontanelle position (Figure 5a, b). Both bregmatic bones possessed an anterior apex, right and left lateral vertices, two anterolateral and two posterolateral margins, though they differed in the posterior parts, which were a base in the child and an apex in the adult (see Figure 5). In both skulls, the anterior apex of bregmatic bones met the persistent metopic suture at the sagittal midline. The anterolateral margins were contiguous to both halves of the frontal bone and the posterolateral ones to the parietals. The right and left lateral vertices were adjacent to the coronal suture. The posterior base of the child’s bregmatic bone crossed the sagittal suture in a transverse direction and met the posterolateral margins. In the adult, the posterior apex met the sagittal suture at the midline. In both cases the sutures demarcating the bregmatic bone on the exocranial aspect were with a structure typical of the coronal one, except for the posterior base in the child and the posterior halves of the posterolateral margins of the adult, which resembled the pattern of the sagittal suture. Thus, the sutures surrounding the bregmatic bones appeared to be a direct continuation of the coronal and sagittal ones. The bregmatic bones on the exocranial surface were slightly raised above the other calvarial bones, but followed the curvature of the skull. In the adult, the sagittal midline diameter of the bregmatic bone was larger on the exocranial surface compared to that of the endocranial one, whereas the transverse diameter was larger on the endocranial surface than the exocranial one (Table 1).

Bregmatic bones: (a) in the child; (b) in the adult. Abbreviations: MS, metopic suture; CS, coronal suture; SS, sagittal suture; AA, anterior apex, lALM, left anterolateral margin; rALM, right anterolateral margin; lLV, left lateral vertex; rLV, right lateral vertex; lPLM, left posterlateral margin; rPLM, right posterolateral margin; PB, posterior base; PA, posterior apex.
| Measurements | Adult | Infant | ||||
|---|---|---|---|---|---|---|
| Diameters of bregmatic bone | Exocranially | Endocranially | Exocranially | |||
| Sagittal diameter (SD) | 75 | 70 | 30 | |||
| Transverse diameter (TD) | 52 | 54 | 21 | |||
| Basis | — | — | 23 | |||
| Margins of bregmatic bone | Right | Left | Right | Left | Right | Left |
| Anterolateral margin (ALM) | 43 | 45 | 43 | 45 | 14 | 15 |
| Posterolateral margin (PLM) | 46 | 51 | 44 | 46 | 25 | 24 |
| Metopic suture (MS) | Exocranially | Endocranially | Exocranially | |||
| Chord | 85 | 73 | 93 | |||
| Arch | 96 | 77 | 108 | |||
In both cases, a persistent metopic suture was seen on the exo- and endocranial surfaces (Table 1). The suture was situated between the nasion and the anterior apex of the bregmatic bone (Figure 1, Figure 2, Figure 4). In the adult, the continuation of the coronal suture drawn as a line upon the bregmatic bone divided it into two equal halves, whereas the sagittal axis connecting the metopic and sagittal sutures divided the bregmatic bone into a larger left and a smaller right part (Figure 5b). In the child, the same lines divided the bregmatic bone into a smaller anterior part and a larger posterior one, and into almost equal right and left halves as the right one was slightly larger (Figure 5a).
In the adult, granular foveolae were seen on the parietal bones along the sagittal suture. However, they were more numerous on the bregmatic bone (Figure 2b).
In the child, sutural bones were observed at the posterior part of the sagittal as well as in the lambdoid suture (Figure 1d). In the adult, a large wormian bone was placed at the upper part of the occipital squama beneath the lambda (Figure 6). A smaller separate sutural wormian bone, which was probably situated along the lambdoid suture, was also present (Figure 2d).

Wormian bone in the upper part of the occipital squama in the adult.
The internal structure of the bregmatic bone and the surrounding calvarial bones in both individuals was typically trilaminar. No evident pathological alterations in the diploic thickness of the adult calvarial bones were registered.
In the region of the anterior and posterior apexes of the bregmatic bone in the adult, the sutural facets of the surrounding bones enclosing the bregmatic bone were obliquely arranged and overlapping on the endocranial surface, whereas in the region of the lateral vertices they were slightly inclined from endo- to the exocranial surface (Figure 7). In the child, a similar tendency was observed, though not so clearly expressed (Figure 8).

Bregmatic bone wedging into the calvarial bones in the adult: (a) coronal section at the region of the posterior apex; (b) coronal section at the level of the lateral vertices; (c) sagittal section at the midline.

Bregmatic bone wedging into the calvarial bones in the child: (a) coronal section at the anterior apex; (b) coronal section at the level of the lateral vertices; (c) coronal section at the region of the posterior base; (d) sagittal section at the midline.
In the child, there was no sign of frontal bone pneumatization and development of the frontal sinus (Figure 8d). In the adult, however, the frontal sinus was large and asymmetrically developed on either side of the metopic suture and the left sinus was larger than the right one (Figure 9a). Furthermore, on the left half of the sinus a bony ridge projected in an anteroposterior direction. A well-defined sclerotic lesion attached to the ridge was observed. The lesion was radiodense, i.e. composed exclusively of compact bone and had the semblance of an osteoma (Figure 9b).

Frontal sinus osteoma in the adult: (a) transverse section; (b) coronal section.
As far as we know, there have been only a few reported cases of large bregmatic bones in adults (Gruber, 1852; Barberini et al., 2008; Becker, 2003; Radović and Miladinović-Radmilović, 2013). Nevertheless, only the findings of Becker (2003) and Radović and Miladinović-Radmilović (2013) have also showed a persistent metopic suture and coincide with ours. However, in the case reported by Becker (2003), most of the right coronal suture was largely obliterated, possibly by a disease. Hauser and De Stefano (1989) have also illustrated a case of a two-part squarish bregmatic bone in an adolescent with metopism.
Because of the rarity of bregmatic bones, the metric data characterizing their size are insufficient. The bregmatic bone reported by Gruber (1852) was 5 cm × 6 cm. Other recently described bregmatic bones had equal values for the transverse diameter on the exocranial surface, i.e. 56 mm. The reported values for their sagittal diameter were 57 mm (Barberini et al., 2008) and 69 mm (Radović and Miladinović-Radmilović, 2013), respectively. Thus, compared to these data the adult bregmatic bone described here was more elongated in the sagittal midline and narrower in the transverse direction (Table 1). What we found confirms that the adult bregmatic bone in our case was rhomboid and consistent with an anterior fontanelle shape, whereas in both previously reported cases the bregmatic bones were pentagonal and did not exactly reflect a fontanellar shape.
In the adult, the size differences between exo- and endocranial diameters of the bregmatic bone are due to the oblique arrangement of the sutural facets and represent a kind of wedging of the bregmatic bone into the frontal and parietal bones (Figure 7). In the sagittal plane the bregmatic bone is built in from the exo- to endocranial aspect, whereas in the coronal it seems to be built in from the endo- to exocranial aspect.
It is worth noting that the bregmatic bone is significantly correlated to the wormian bones in the sagittal and lambdoid sutures (Hauser and Bergman, 1984). The reported cases of a large bregmatic bone along with a persistent metopic suture also displayed wormian bones in the lambdoid suture (Radović and Miladinović-Radmilović, 2013; present study).
Implication of the bregmatic bone formation and metopic suture retentionThere have been reported cases of bregmatic bone presence without other apparent alteration of the vault architecture, and due to this it was supposed that the bregmatic bone did not interfere with the normal growth of the skull (Girdany and Blank, 1965; Woods and Johnson, 2010) and represents an innocuous variation. In these cases, the bregmatic bone has been considered of clinical significance because it may erroneously suggest a premature closure of the fontanelle or a fracture of the frontal or parietal bones in radiological imaging (Girdany and Blank, 1965).
However, the formation of a bregmatic bone has been frequently associated with a non-syndromic isolated craniosynostosis and more commonly with a sagittal one (Agrawal et al., 2006; Sanchez-Lara et al., 2007; Woods and Johnson, 2010; Stotland et al., 2012). An interesting finding was the formation of a bregmatic bone after a surgical intervention for sagittal craniosynostosis (Cray et al., 2010). The non-syndromic single-suture craniosynostosis has been often related to an increase in the intracranial pressure (Tamburrini et al., 2005; Wall et al., 2014) and more commonly when a midline suture (metopic or sagittal) is involved (Thompson et al., 1995). In these cases, the intracranial pressure tends to grow gradually, occurring with the growth of the child (Tamburrini et al., 2005). Furthermore, the initial site in the sagittal synostosis is crucial for the direction of the increased intracranial pressure from the rapidly growing brain, anteriorly or posteriorly along the midline. This causes the sutural widening and dural strain which probably trigger the wormian bone formation in the anterior or posterior fontanelles (Sanchez-Lara et al., 2007).
Interestingly, the cultural cranial deformations of different types seem not to be related to the bregmatic bone in adults (O’Loughlin, 2004; Van Arsdale and Crark, 2012), although its presence during childhood cannot be excluded. A CT investigation of adult skulls with an oblique and erect form of annular intentional deformation from Bulgaria rejected the existence of indirect bony signs of chronic elevated intracranial pressure (Enchev et al., 2010). It seems that the application of a constant external pressure (binding of the infant’s head) is involved to a lesser extent in the bregmatic bone formation, compared to the internal straining caused by a gradual elevation of the intracranial pressure due to craniosynostosis. Besides craniosynostosis, the elevation of the intracranial pressure could be a consequence of many other heterogeneous conditions such as haematoma, neoplasm, trauma, seizure, hydrocephalus, meningitis, etc. (Du Boulay, 1980), as most of them are not associated with distortion of the skull configuration. In infants, the main signs of acute and chronic elevated intracranial pressure are suture diastasis and bulging of the anterior fontanelle (Du Boulay, 1980). So, the retention of the metopic suture along with the formation of a bregmatic bone could represent indispensable accessory sites for the regulation of the bone growth as a response to the increasing brain mass requirements under such specific circumstances. This could be a mechanism for maintaining the optimal balance between the calvarial shape and size for a maximal effectiveness and stability in the presence of some developmental abnormalities. Undoubtedly, purposeful studies are needed to evaluate a hypothetical influence of the increased intracranial pressure over these structures taking into account the causative condition, time of occurrence, and its duration.
This work was partially supported by FP7 project AComIn ‘Advanced Computing for Innovation’ grant 316087, Bulgarian Ministry of Education and Science grant DO1-192/214, and H2020 project VI-SEEM contract no. 675121.
The authors declare no conflict of interest.