Abstract
The hypothesis of an American origin of acquired (venereal) syphilis and other infectious diseases carried by Columbus’s crew has been considered for a long time as the most plausible one, and has been supported recently by considerable anthropological and molecular evidence. According to this line of thought, it can be argued that Spain would have been the gateway of acquired syphilis, which quickly expanded after the return of Columbus in the late 15th century. However, the hypothesis that syphilis previously existed in Europe but went unrecognized has also been considered by many authors. The present work reports one Pre-Columbian putative case of venereal syphilis found in a Spanish necropolis and radiocarbon dated to the 9th–11th century. The complexities of carrying out accurate diagnoses in remains from archaeological timeframes are addressed by the combined use of palaeopathological, medical, and histological techniques. The results, which point toward third-stage acquired syphilis, spark discussion about the need to revisit or complement the theories and hypothesis on the origin of syphilis in the light of a growing body of cases from European historical populations.
Introduction
Treponematosis is a chronic or subacute infectious disease whose causative agent is an anaerobic filamentous spirochete of the genus Treponema (Turner and Hollander, 1957). Based on clinical and geographical criteria, four types of treponemal infection can be distinguished: pinta (called mal de pinto or cute), yaws (or frambesia) and bejel (also known as non-venereal syphilis or endemic syphilis), which are transmitted by fomites (shared contaminated utensils) and non-venereal contact (Perine et al., 1984); and acquired syphilis (or simply syphilis), which might be congenital or acquired. Of all of these, only pinta, caused by Treponema carateum, does not leave evidence in the bone, causing only cutaneous disease (Powell and Cook, 2005; Farnsworth and Rosen, 2006; Mandell et al., 2009). The other three types of treponemal disease are caused by infection of different subspecies of Treponema pallidum: T. pallidum subsp. endemicum leads to bejel, T. pallidum subsp. pertenue causes yaws, and T. pallidum subsp. pallidum is the bacteria responsible for both congenital and acquired syphilis (Antal et al., 2002; Centurion-Lara et al., 2006; Mandell et al., 2009).
Some authors have hinted that syphilis could have acted as a decimating agent in the European continent during the Renaissance and Early Modern Age (Quétel, 1990), although no reliable epidemiological data exists to assess the real demographic impact of this disease. In the late 15th century, the first outbreak of this epidemic was reported in the Old World, carried and disseminated by mercenaries accompanying King Charles VIII of France in the invasion of Italy. In the 16th century syphilis became more widespread but reportedly became less virulent (Quétel, 1990; Sefton, 2001; Tognotti, 2009), and a controversy started about whether this disease could be a result of the mutual European–American discovery (Berlinguer, 1992). The exchange of infectious diseases in this context, at least from Europe to America was not rare, and some examples are very well known, such as influenza, poliomyelitis, rabies, smallpox, measles, and mumps. In the opposite direction, from America to Europe, the findings are less clear. For example, it has been said that tegumentary leishmaniasis may have originated in South America and travelled from the New world into Europe (Gonçalves et al., 2004; Lukeš et al., 2007). Nevertheless, studies from Ancient Egypt and Upper Nubia found cases of leishmaniasis in humans as early as 2000 BC in north-east Africa (Zink et al., 2006). The sporadic nature of anthropological findings and the difficulties of phylogenetic dating make these cases of conflicting evidence very hard to resolve (Clark, 2010).
There is added controversy regarding the origin of syphilis. One of the most popular and oldest hypotheses (the ‘Columbian hypothesis’) promulgates that the disease came from America and subsequently spread throughout Europe (see Naranjo, 1994, for a review). The chronicler Gonzalo Fernandez de Oviedo was probably the first person who argued for the Columbian hypothesis. In 1526, after a decade living in Santo Domingo, he published a book (Of the Natural History of the Indies), where he described how the natives used lignum vitae (Guaiacum sp.) to treat syphilis. Nine years later, in his comprehensive study General and Natural History of the Indies, isles and mainland of the Ocean, he argued for the American origin of syphilis based on his research of indigenous medicine and lignum vitae. This followed the common maxim at the time that “wherever God sends punishment or disease, there he also sends the cure” (Steinbock, 1976). Modern ethnohistorical and palaeoanthropological studies from Jamaica have indeed suggested that the indigenous Taínos (Pre-Columbian inhabitants of the Bahamas and Antilles) suffered endemically from syphilis, and used medicinal plants to treat this (Santos et al., 2013). For many years the archaeological evidence supported this American origin (Baker and Armelagos, 1988; Powell and Cook, 2005), as the vast majority of incontestable syphilis cases were found in New World sites. For example, Rothschild et al. (2000) recognized acquired syphilis in Pre-Columbian archaeological remains in areas where Columbus actually had contact with the natives, identifying the Dominican Republic as the point of initial contact with syphilis and subsequent spread from the New to the Old World. Sailors enrolled in Christopher Columbus’s ships have long been regarded as the probable first importers of the infection (e.g. Price, 1979), which would have arisen in the New World before the arrival of the Europeans and would have been one of the intercontinental exchanges that occurred over time.
In recent years, some authors have reported lesions compatible with acquired syphilis in Pre-Columbian skeletons in regions as distant as Britain (Stirland, 1991; Mays et al., 2003, 2012; von Hunnius et al., 2006; Cole and Waldron, 2011), central Europe (Gaul et al., 2015), and the eastern Mediterranean (Mitchell, 2003, 2009; Erdal, 2006). These findings, if their palaeopathological assessments are correct, support a view different to the Columbian hypothesis: the Pre-Columbian hypothesis. First formulated in the earliest decades of the 20th century, this argument proposes that syphilis, or a closely related treponemal disease, was already present and widespread both in the New and the Old World in Pre-Columbian times. In ancient Europe, a possible source of confounding might have been leprosy, whose transmission agent is the Hansen bacillus, Mycobacterium leprae (Holcomb, 1934; Hudson, 1961; Meyer et al., 2002; Powell and Cook, 2005), and which was only recognized as a different entity to syphilis because of a surge of virulence (Meyer et al., 2002; Waldron, 2009). In this framework, it is thought that recognition of treponemal diseases improved over time, and references to syphilis became increasingly more usual. Some authors propose that a reason for the increase of awareness of syphilis were important outbreaks (Waldron, 2009) that could have been caused by virulent New World strains (El-Najjar, 1979; Kampmeier, 1984).
While these hypotheses are both supported by palaeopathological findings, actual strains of treponemal bacteria have been analysed to assess the origin of acquired syphilis using phylogenetic approaches. Hackett (1963) proposed an interesting mutational pattern of the origin and dispersal of the four treponemal diseases. He argued that acquired syphilis could have arisen in south-western Asia from a mutation in the bacteria that causes bejel about 5000 years BP. Later it would have spread to Europe and the rest of the world. This theory has been recently tested with phylogenetic methodology, which showed that pathogenic yaws-causing Treponema from Africa showed the greatest similarity with simian strains and were the first to arise in human history (Harper et al., 2008). Additional evidence was added by the finding of two new strains of T. pallidum in inhabitants from Guyana. The Guyana disease, caused by a DNA-related strain of T. pallidum, seemed like a combination of two diseases, syphilis and yaws, with raspberry-like eruptions and without open sores. It has been suggested that this organism could be the ancestor from which T. pallidum evolved thousands of years ago (Harper et al., 2008).
This collection of results excludes the possibility of syphilis being present in Europe before the return of Columbus, and points to other treponemal diseases, not acquired syphilis, as responsible for the above-mentioned Pre-Columbian Old World cases. A recent paper by Harper et al. (2011) showed an extensive review of published syphilis cases belonging to the Old World (Africa, Asia, and Australia and Europe). The conclusion of this study was that no single case with a convincing diagnosis had a secure Pre-Columbian date, though some of its arguments were disputed (Cole and Waldron, 2012). In any case, the authors of the original paper maintained their position and claimed that their intention was not to rediagnose putative cases but to assess the certainty of both diagnoses and dating, as some of the findings traditionally held as true by the scientific community had actually been published in journals which lacked a proper peer-review process (Armelagos et al., 2012).
Despite all the methodological and technical advances, the origin of acquired syphilis remains a controversial matter. Assuming the Columbian hypothesis and an origin of syphilis in the New World, the Iberian Peninsula would have probably been the gateway for the entry of the disease into Europe given the large number of sailors who travelled with Christopher Columbus to the Old World and back (Gould, 1925; Díaz-Trechuelo, 1991). In fact, when the first reported outbreak occurred in Naples in 1495, Spanish soldiers garrisoned there were seen as the transmitters of the disease to the general population and the mercenaries who later scattered throughout Europe (Pearce, 1998). Considering this fact and the existence of one account, albeit of dubious accuracy, of a syphilis outbreak in Barcelona in 1493 (Meyer et al., 2002), there exists the possibility that many early episodes of the epidemic could have actually taken place in Spain. This might have been historically unnoticed, given the presumably high mobility of sailors in the past and the documented speed with which the epidemic moved (Tognotti, 2009), which would have made any area of the European continent equally affected in a few years. While this is a hypothesis to consider, it is not currently supported by available data, as, to our knowledge, there have been relatively few published cases of palaeopathological putative acquired syphilis (Reverte, 1979; Lopes and Cardoso, 2000; Codinha, 2002; De Souza et al., 2006; Rissech et al., 2013; Schwarz et al., 2013) coming from the Iberian Peninsula before the Modern Age.
To contribute to this currently small body of cases, we report in this study the analysis of one Pre-Columbian skeleton, which shows lesions that could be attributable to alleged acquired syphilis. Skeletal evidence from Spain such as this could shed further light on the debate concerning the origins of acquired syphilis in Europe. The remains were found in an archaeological excavation of a cemetery from the northern part of the Iberian Peninsula dated to the 9th–11th century. Those were intense years of military activity in that part of Spain, as a small Christian nucleus, the Kingdom of Asturias, became established and expanded into the territories of the dominating Umayyad Caliphate (Boyd, 2002). The territory of this kingdom reached the Douro river in the year 910 and as a consequence King Ordoño II (914–924) moved its political core further south, creating the Kingdom of Leon (O’Callaghan, 2013). Between the 11th and 13th centuries, further expansion resulted in the establishment of the Kingdom of Castile, the borders of which expanded past the Spanish central mountains and into the Tagus river basin (Zamora, 1973).
Materials and Methods
Studied necropolis
The archaeological intervention was carried out in the years 1990 and 1991, at the ‘La Morterona’ necropolis, located in the municipality of Saldaña, in the present territory of Castilla-Leon (Figure 1). The necropolis was completely excavated and 56 individuals were recovered—a total of 15 subadults and 41 adults of both sexes (López, 2000; López Martínez, 2002). Historical and archaeological evidence showed that the necropolis was used during the medieval era (9th–15th centuries) and can be considered of Pre-Columbian origin. Osseous material was directly provided to the researchers by the archaeologists in charge of the excavations, under the responsibility of the Regional Government of Castilla-León.
Dating
Due to the importance of knowing exactly the antiquity of the remains found in this medieval necropolis, radiocarbon dating of a fragment from the basilar region of the occipital bone from the reported individual was performed at the Beta Analytic Inc. laboratory (Miami, FL, USA) in 2011. Accelerator mass spectrometry was used for dating (Elmore and Phillips, 1987), and the laboratory code given was Beta-311429. The result of the radiocarbon analysis was calibrated to calendar years using the IntCal09 dataset included in the software CALIB v. 6.01 (Reimer et al., 2009; Stuiver et al., 2010).
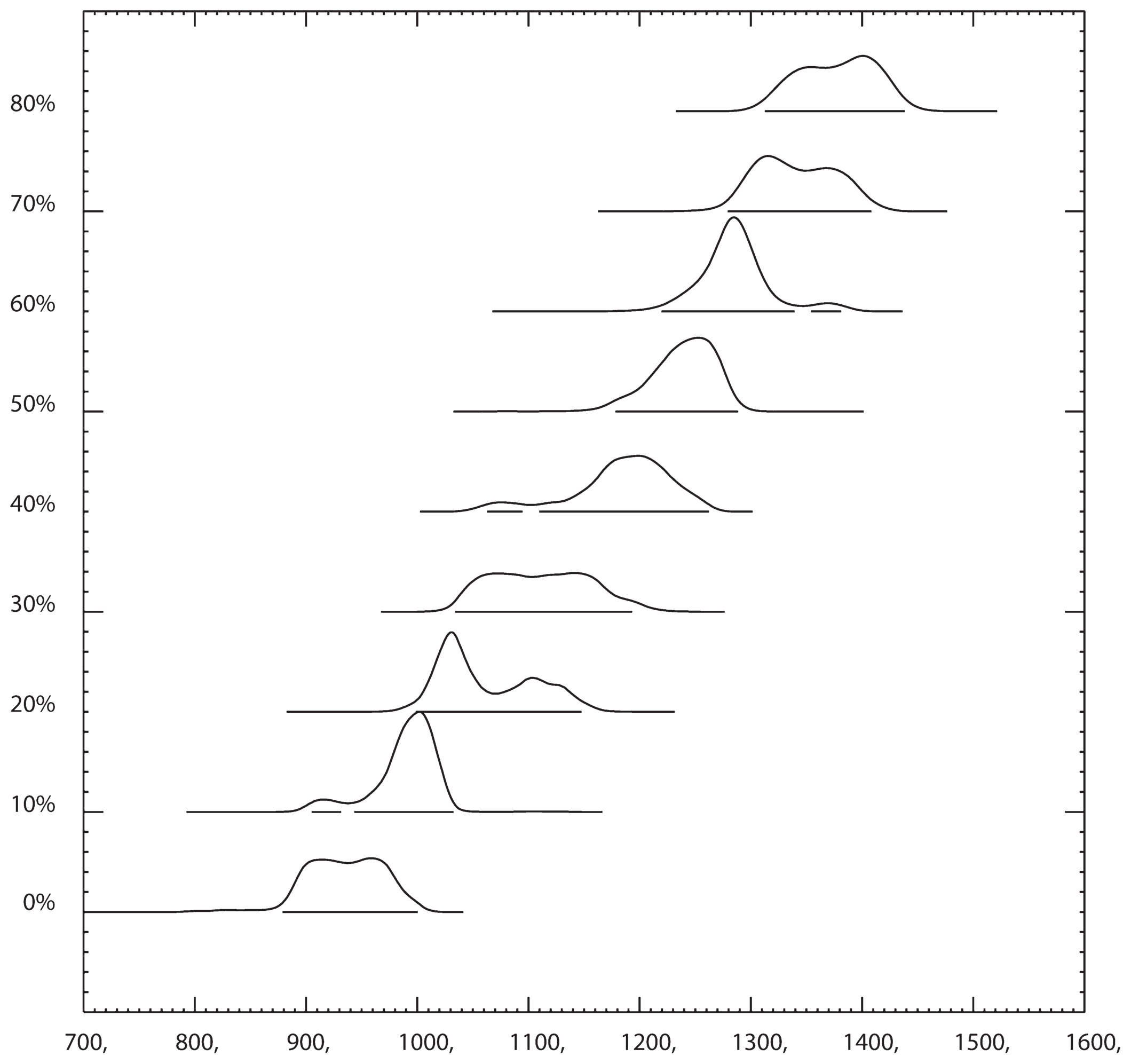
A high dietary intake of marine protein has long been known as a source of bias for radiocarbon dates (Schoeninger et al., 1983; Bayliss et al., 2004). Thus, the proportion of carbon of marine origin in collagen is usually estimated by analysis of stable isotopes of carbon (δ13C) and nitrogen (δ15N) (Mays, 1997). Nevertheless, various concerns have been raised related to accuracy, reliability, and margins of error of this estimation (Harper et al., 2011), and thus we used an indirect approach to assess the influence of marine intake in our radiocarbon dates. Again, using CALIB v. 6.01, calibrated radiocarbon ages were calculated by simulating the presence of up to 80% marine carbon in the sample, at 10% intervals. Also, to properly take into account the marine reservoir effect, a ΔR of 270 ± 40 14C years was considered as valid for our geographical region and temporal period. This quantity was described in a neighbouring region of northern Spain (Galicia) using samples dated at 890 ± 90 BP (Monge Soares and Alveirinho Dias, 2007).
Sex determination
Biological sex determination was based on methods that relied on classical morphological parameters of sexual dimorphism in the os coxae (Byers, 2005). The following morphological features of the pelvis were assessed: presence of a subpubic concavity, ventral arc, and preauricular sulcus; thickness of the ischiopubic ramus; and a greater sciatic notch shape in the pelvic bone. In addition, morphological cranial characteristics of the skull, such as the robusticity of the nuchal crest, the size of the mastoid process, the sharpness of the supraorbital margin, the prominence of glabella, and the projection of the mental eminence, were also used (Buikstra and Ubelaker, 1994).
Age determination
The assessment of age-at-death was based on published standards related to the main macroscopic changes of the pelvis with the following criteria: metamorphosis of the pubic symphysis (Brooks and Suchey, 1990), changes of the auricular surface of the ilium (Lovejoy et al., 1985), and stages of tooth attrition (Hillson, 1996). The general presence of degenerative changes of the skeleton was also used (Cox, 2000).
Individual SAL 633, female, 30–40 years of age
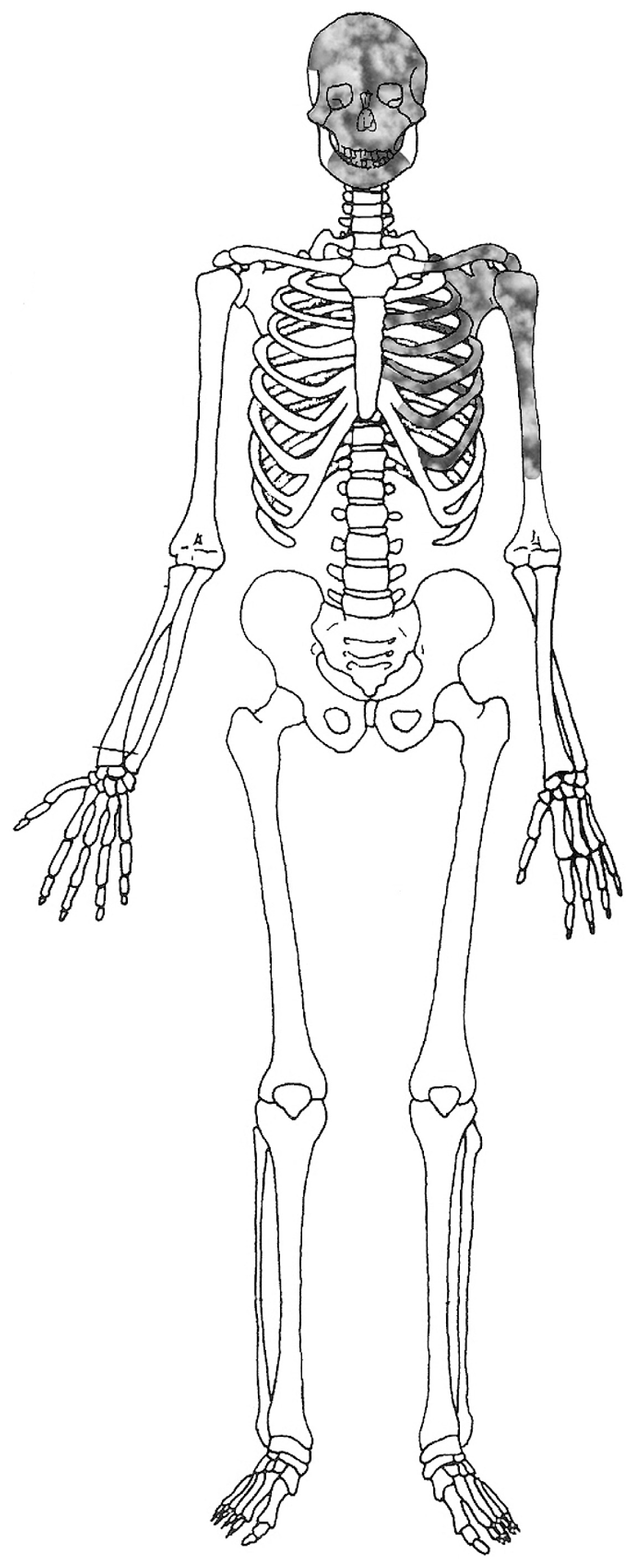
The state of preservation was poor due the fragmentary nature of many of its bones. The skull showed an almost complete splanchnocranium, left parietal, left temporal, part of the occipital bone, and a complete maxillary bone. The upper right second and first incisors and both second molars were lost post-mortem, while the two first molar were lost ante-mortem with full to partial healing of the socket. Only the mandible arch was preserved with all the teeth except both second molars and the right second incisive, which were lost post-mortem. The postcranial skeleton available includes part of the right humerus, scapulae, and clavicle, with some of the ribs of this side, also fragments of sacrum and both os coxae. The remaining bones are missing.
Identification of palaeopathological indicators
The bones and teeth of SAL 633 were examined directly for detection of macroscopic and radiographic lesions suggestive of treponemal disease (e.g. acquired syphilis) as described by Hackett (1975) and Aufderheide and Rodriguez-Martin (1998). Acquired syphilis manifests in three different clinical stages, commonly known as primary, secondary, and tertiary syphilis (Tramont, 1995), several of which result in identifiable skeletal lesions (Ortner, 2003). Soft parts of the body are involved in the disease from the start, and even mild, non-diagnostic lesions may develop in the skeleton in the earliest stage (Ehrlich and Kricun, 1976), though the influence of the disease on the skeletal system usually begins from the late second to tertiary phase (Little, 2005). In the tertiary stage of the disease a reaction may occur in the bone tissue, resulting in either chronic gummatous or non-gummatous inflammation (Steinbock, 1976; Ortner, 2003; Powell and Cook, 2005). These are seen in roughly 10–20% of the cases (Resnick and Niwayama, 1995; Aufderheide and Rodriguez-Martin, 1998) and are mostly a combination of the two processes (Ortner, 2003). Gummatous lesions (erosive granulomas) occur due to an alteration of the blood supply to the tissues, which initiate a reaction that creates a granulomatous appearance of nodular foci with central liquefying necrosis, called ‘gumma.’ The gumma is the classic lesion found in tertiary syphilis (Steinbock, 1976; Aufderheide and Rodriguez-Martin, 1998; Ortner, 2003; Kinghorn, 2004) and it is found in both the skull and long bones. It is widely accepted in palaeopathology that the type of lesions that can be attributed to syphilis cannot be distinguished from those caused by bejel and yaws, the other two variants of treponemal disease (Ortner, 2003; Harper et al., 2011).
Regarding the skull, lesions tend to start in the frontal bone and usually spread to affect other elements of the cranium. Initial lesions are pits on the surface of the bone which may become confluent and deeper (Steinbock, 1976). The boundaries of this lesion usually rise over time, rolling over the margins of the injuries. As healing progresses, the cavity starts to be covered by scar tissue until only a low depression remains, showing radial scarring on the surface. ‘Caries sicca’ is the term that refers to the progress in contiguous lesions that mainly affect the frontal and parietal skull bones (Skinner, 1994; Ortner, 2003; Powell and Cook, 2005). This is a combination of three processes: active lytic lesions, remodelling, and scarring (Waldron, 2009). Hackett (1976) illustrated eight stages of this type of lesion, describing the sequence of events in the formation of lesions in the skull outer table, and its manifestation in dry bone (Table S1).
To improve the differential diagnosis and overcome the former difficulties to some extent, the lesions of the one individual who was macroscopically catalogued as a ‘putative case of treponemal infection’ were inspected in detail by radiographic and histological techniques. Radiographs were performed at the Central University Hospital of Oviedo (Spain) using conventional techniques (40 kv and 2 mAs) and treated in a digital CR Caresteam® system. X-ray computerized tomography (CT) was performed on the skull remains of that same individual using an Aquilion 16 scanner (Toshiba Medical System), employing a 0.5 mm slice thickness. Images were visualized in a Vitrea workstation in which multiplanar and volume-rendered pictures were made. Bone samples for light microscopic analysis were removed using a handheld circular saw and subsequently dehydrated using ascending concentrations of ethanol and embedded in low-viscosity epoxy resin Durkupan-ACM (Sigma) under vacuum. The embedded samples were ground down to a thickness of 15 μm, stained with toluidine blue and analysed using a Nikon Eclipse E400 microscope equipped with phase contrast, following the approach of Schultz 2001.
Results
Only the adult female SAL633 (estimated age 30–40 years) exhibited lesions that could be indicative of acquired syphilis. Radiocarbon analysis provided a date for these remains of 1110 ± 30 BP, and calibration using the IntCal09 dataset provided a corrected date of 879–1001 AD (at 2σ). The 13C/12C ratio measured in the bone sample was of −21.1‰, which has been traditionally considered as indicating no marine contribution to the diet of the living individual (Arneborg et al., 1999). Further evaluation of a possible bias due to marine protein intake by the individual is shown in Figure S1. The maximum calibrated age interval reached by our sample occurs at the value of 80% of marine contribution and is 1313–1439 AD (at 2σ).
The skull of this individual had been fragmented during excavation, and was partially reconstructed later in the laboratory. It showed three lesions in the outer table of the frontal bone, of which the bigger one comprised an irregular eroded area of 8 × 5 cm (Figure 2). This area was separated by 30 mm from the glabellum. It strongly affected the outer table, while the inner table presented a slight porosity. The erosion, with the margins rolled inwards towards the center, manifested an important loss of diploe in some points. In an ectocranial view, islands of surviving outer table and confluent pit clusters can be seen (Figure 3). There were other two important lesions of smaller size, situated near to the coronal suture (Figure 4), showing the same erosion and loss of diploe described in the bigger one. There were other two important features in this skull: a smooth porosity (cluster of pits) over the orbital margin and glabellum, and a widening of the nasal cavity which appeared empty due the post-mortem destruction of the nasal septum (Figure 2). The maxillary bone also appeared to have a perforation of the hard palate, but we cannot be sure that this is due to the high degree of destruction.



Radiographs showed a lytic lesion in the frontal bone, with irregular edges without a sclerosing reaction (Figure 5). CT volume-rendered images show three irregular destructive lesions of worm-eaten appearance, which involve the outer table. Multiplanar slices show an irregular destruction on the outer table and some portions of the diploe (Figure 6). Microscopic analysis of bone samples from this lesion demonstrated the presence of many characteristic features of diagenetically modified bone originated by the post-mortem destruction of bone tissue by taphonomic processes. However, it is remarkable that the fundamental histological pattern of the bone, characterized by concentric bone layers encircling Haversian canals, was clearly recognizable (Figure 7A). Furthermore, some regions showed osteons with a modified lamellar layering pattern consisting of irregular accumulations of stacks of non-concentric lamellae (Figure 7B). This structure is consistent with partial healing after necrosis by formation of less organized bony tissue which would be subsequently remodelled and implies the occurrence of bone formation, a distinctive feature of caries sicca.


Most of the other skeletal material from SAL633 was lost during the excavations and before the archaeological team arrived. The remains recovered included the mandibular arc, with partial dentition but without the ramus mandibulae; the left humerus without the distal third; the left scapula and some ribs (Figure S2). None of these elements showed any signs that could be pathognomic for syphilis or other diseases.
Discussion
Radiocarbon dating showed that SAL633 lived during the War of Reconquista period (9th–11th century), in the Pre-Columbian era. Even though these dates could be biased by an undetected marine intake in the diet of the individual, the antiquity of the remains does not encompass Post-Columbian times in any way. Simulation analysis of marine carbon in our sample showed that the calendar date of the return of the first Columbian expedition (1493 AD) is never reached, even when marine uptake is raised up to 80%. It should be noted that such a high proportion of marine-based carbon would be at best improbable in an inhabitant from an inland peasant population such as the one we studied, with no direct access to marine resources other than importing them from neighbouring regions (Polet and Katzenberg, 2003; Müldner and Richards, 2005).
Palaeopathological results are based on direct inspection of morphological osseous lesions, as well as radiographic and histologic study. While full certainty can hardly be achieved even combining all these methods, a detailed analysis of skull and bone lesions is still considered the most reliable method for identification of acquired syphilis in past populations (Ortner, 2009). In this case, the CT appearance of our specimen (Figure 6) is very similar to images which have been reported by Gurland et al. (2001) and Huang et al. (2007) in HIV-infected patients with acquired syphilis; and also by Kang et al. (2010) in a patient with confirmed T. pallidum infection. This morphological appearance has been previously reported as characteristic of acquired treponemal infection on radiographic and palaeopathological assessments (Thompson and Preston, 1952; Ortner, 2003; Shang and Trinkaus, 2008; Boone et al., 2009; Reinus, 2010). As for the microscopic structure, it is relatively well preserved and scar tissue can be unmistakably recognized. The occurrence of this scar tissue implies a healing process including new bone tissue formation. This is consistent with the hypothesis that the living bone could have suffered an inflammatory process induced by bacterial infection, which would have caused a diminishing of blood supply to the centre of the lesion and, over time, necrosis.
Differential diagnosis
It is important to consider that these bone lesions, albeit similar to others which had been identified as the result of acquired syphilis, could also have been caused by pathologic processes other than treponematosis. The first circumstance that we must consider is the possibility that post-mortem taphonomic processes could have caused them, since the alteration of the characteristic morphology of the outer or inner table of bones due to the action of natural factors such as animals, plants, water and soil features is possible. Post-mortem damage might sometimes be difficult to differentiate from certain pathological conditions that affect the skeletal structure, but some processes can hardly be mimicked by natural post-mortem damage. This is the case of the alterations in the SAL633 skull, which exhibits both bone osteolysis and neoformation, as these cannot be caused by taphonomy.
Regarding the specificity of lesions to acquired syphilis, it has to be said that osseous reactions, although reproducible for each variety of treponemal disease (except pinta, which does not manifest in bone), are not uniform between skeletons. Thus, there is no histological, biochemical, immunological, or microbiological technique that can be used to distinguish them (Noordhoek et al., 1990; Rothschild and Rothschild; 1995, Waldron, 2009). This led syphilis long being called “the great imitator” (Ehrlich and Kricun, 1976; Sefton, 2001), as both its clinical pathogenesis and skeletal alterations are very similar to other diseases such as leprosy, tuberculosis, Paget’s disease, or haematogenous osteomyelitis (von Hunnius et al., 2006). Thus, in archaeological specimens it is very difficult to achieve a differential diagnosis, especially for an incomplete skeleton. The great majority of lesions commonly attributed to syphilis, such as periostitis and tibial bowing, are non-specific and can be caused by different diseases, both infectious and no-infectious, so it is not unusual that bone alterations of putatively syphilitic individuals mimic several diseases. Von Hunnius et al. (2006) recommended a microscopic approach to differentiate disease processes, but also commented on the difficulties in using the features reccomended by Schultz (2001) for palaeohistological diagnosis: Grenzstreifen (border stripes), polsters (padding) and ‘sinous lacunae.’ Other authors, such as Weston (2009), have suggested that these microscopic features cannot be used to diagnose specific pathological conditions at all, as they were found to occur in pathological bone specimens with different disease aetiologies.
The above reasons indicate that, if a pathological explanation is considered, some alternative causes should also be considered. One is osteomyelitis, but there is no evidence of the sequestra or involucra typical of such disease (Rogers and Waldron, 1989; Aufderheide and Rodriguez-Martin, 1998; Waldron, 2009). A possible metastatic neoplasm can also be discarded because it implies multiple perforating skull holes, which are not present in our case (Aufderheide and Rodriguez-Martin, 1998; Shang and Trinkaus, 2008). Furthermore, the bony changes and alterations exhibited by these remains do not correspond with other infectious diseases that can be confounded with acquired syphilis. Tuberculosis, for example, typically produces a lone lesion that destroys both tables, the destruction being much more evident in the inner table where the disease first manifests in the skull (Mitchell, 2003; Ortner, 2003; Shang and Trinkaus, 2008). Leprosy also destroys bone, but its pathological changes are not frequently found in the skull vault as in our case (Møller-Christensen, 1965; Ortner, 2003). Paget’s disease, of unknown aetiology, can also be ruled out, as the engrossing of the cranial vault is very different to our case (Steinbock, 1976; Aufderheide and Rodriguez-Martin, 1998).
Finally, it should be said that the different types of treponematosis are nearly impossible to differentiate by the lesions they leave on archaeological specimens (Hackett, 1976; Webb, 1995; Ortner, 2003; Harper et al., 2011). Nevertheless, the geographical location in which our remains were found makes it unlikely for yaws to be the causative agent of our possible case of treponematosis, as this is a tropical disease (Farnsworth and Rosen, 2006). The possibility of bejel cannot be completely discarded and has to remain open, as even though this disease is uncommon in Spain (Berco, 2011) and typical of hot desert areas, it has also been described as endemic in some regions of temperate Europe (Baker, 2005). Of course, apart from this last remark, one must consider the possibility that our specimen could have contracted one of these diseases during a voyage to another country, or even that the remains belong to an immigrant who was buried in the cemetery of Saldaña.
As for other kind of analyses which can identify acquired syphilis it should be said that they exist, but their use in archaeological remains is unclear. Some years ago, T. pallidum subsp. pallidum, the causative agent of syphilis, was detected in a 200-year-old skeletal specimen from Easter Island by DNA analysis (Kolman et al., 1999), and sensitive molecular markers for detection of this bacteria in living tissues have long been known (e.g. Burstain et al., 1991). However, further assays failed to detect treponemal DNA in bones otherwise suitable for ancient DNA analysis, even when using highly sensitive PCR protocols, suggesting that treponemal DNA is not well preserved in human bone and that ancient DNA analysis is not adequate, at present, to study ancient cases of putative acquired syphilis on a routine basis (Bouwman and Brown, 2005; Barnes and Thomas, 2006). Treponemal bacteria (and, consequently, its DNA) likely disseminates to bone early during the first stages of infection but is not present in the same location at later stages of the disease, making ancient DNA techniques unreliable for studies on acquired syphilis in past human populations (von Hunnius et al., 2007).
Conclusions
Some conclusions can be obtained from our results. The first is that acquired syphilis may have occurred in Spain before the European–American interchange, as early as in the 9th century. This supports other studies reporting Pre-Columbian syphilis in Europe and adds to a recently growing field of evidence that does not agree with the Columbian hypothesis of an American origin of syphilis (e.g. Mitchell, 2009; Mays et al., 2012; Cole and Waldron, 2011). Nevertheless, all these cases and many others have been recently evaluated by Harper et al. (2011), in a study that raised numerous critiques of their diagnostic and dating criteria, eventually concluding that the only incontestable reported cases of syphilis from Pre-Columbian times have their origin in the New World. Even in light of this recent review, the pathologic evidence shown in our remains, coupled with their antiquity, forces us to propose that the European Pre-Columbian existence of acquired syphilis is, at least, possible. Thus, we also have to seek an explanation for the origin of syphilis in the Old World. European contacts with the New World in the form of Viking expeditions from Greenland have been proposed as an explanation, but this is not supported by existing historical or skeletal evidence (Mays et al., 2003). Another explanation could be the introduction of syphilis in Europe by the pilgrims and crusaders that marched to the Near East during the Crusades (Hudson, 1963). These took place during the 11th–13th centuries, greatly enhancing human and trade flow between Europe and south-west Asia (Lewis, 1991).
A possible earlier origin has been defended using the cases of congenital syphilis found in the Greek colony of Metaponto (southern Italy), dated between the 1st and 4th centuries BC (Henneberg and Henneberg, 1994). Greek colonies in this period were scattered throughout Europe and western Asia (Cerchiai et al., 2004), and syphilis could have arrived at this particular location from some other place in the Mediterranean. The major drawback of the Metaponto cases is that they never were published in a peer-reviewed publication, or adequately photographed, so their validity is contested (Harper et al., 2011). Another alternative hypothesis would be based in a possible origin of syphilis in Saharan or Sub-Saharan Africa, where it is currently a major burden (Gerbase et al., 1998), although the endemicity of bejel in this areas accounts for many misdiagnoses of treponemal disease (Baker, 2005). A putatively long-standing relationship of African populations with treponemal disease was previously proposed by Hudson (1964), and contacts between European and African societies have occurred at least since the 2nd millenium BP, according to archaeology and ancient DNA studies (Brun et al., 1998; Martínez-Laso et al., 2000; Anderung et al., 2005). While there is a famous Egyptian archaeological case of treponematosis from the first millennium AD (Ortner, 2003), its dating methodology was never provided (Harper et al., 2011). Apart from that, there are no other clear syphilis cases coming from other African archaeological sites. This could be due to the high degree of deterioration that skeletal material quickly suffers in arid environments, both after and prior to burial (Maat, 1993; Trueman et al., 2004), which may erase identifiable traces of treponematosis. Even so, it is worth mentioning that if an African origin of syphilis were proposed, the Iberian Peninsula would again appear as a probable gateway for the entry of treponemal infections into Europe, as the Strait of Gibraltar is thought to have been a place of frequent contact between European and African human populations (Escacena, 2000; Pardiñas et al., 2014).
As for the Columbian hypothesis, one of its last main supporters is the phylogenetic approach of Harper et al. (2008), which suggested an American origin of trepanematoses. Harper et al. compared modern DNA sequences of isolates from different countries, including American, Asian (India) and African (South Africa) strains of T. pallidum subsp. pallidum as well as strains of other pathogenic subspecies (pertenue, endemicus) and even different Treponema species. The resulting phylogeny supported an American origin of acquired syphilis, but no Spanish strains of T. pallidum subsp. pallidum were represented, nor were strains from other parts of Europe, such as Britain or the Mediterranean, reported. A more recent analysis of whole-genome data from T. pallidum strains from worldwide patients showed all the samples shared a common ancestor around the time of the Columbian voyages, and while this supports that population dynamics after this date favoured the emergence of a syphilis pandemic, it does not resolve where the ultimate origin of the pathogen lies (Arora et al., 2016). It might be the case that genetics, or indeed any of the individual techniques outlined in this article, might not be able to resolve such a persisting question on its own, and multidisciplinary approaches on current and future palaeopathological findings will surely be needed.
Acknowledgments
This study has been supported by the research Contract EL01/98, funded by the Consejería de Educación y Cultura de la Junta de Castilla y León.
References
- Anderung C., Bouwman A., Persson P., Carretero J.M., Ortega A.I., Elburg R., Smith C., Arsuaga J.L., Ellegren H., and Götherström A. (2005) Prehistoric contacts over the Straits of Gibraltar indicated by genetic analysis of Iberian Bronze Age cattle. Proceedings of the National Academy of Sciences of the United States of America, 102: 8431–8435.
- Antal G.M., Lukehart S.A., and Meheus A.Z. (2002) The endemic treponematoses. Microbes and Infection, 4: 83–94.
- Armelagos G.J., Zuckerman M.K., and Harper K.N. (2012) The science behind pre-Columbian evidence of syphilis in Europe: research by documentary. Evolutionary Anthropology: Issues, News, and Reviews, 21: 50–57.
- Arneborg J., Heinemeier J., Lynnerup N., Nielsen H.L., Rud N., and Sveinbjörnsdóttir A.E. (1999) Change of diet of the Greenland Vikings determined from stable carbon isotope analysis and 14C dating of their bones. Radiocarbon, 41: 157–168.
- Arora N., Schuenemann V.J., Jäger G., Peltzer A., Seitz A., Herbig A., Strouhal M., Grillová L., Sánchez-Busó L., Kühnert D., Bos K.I., Rivero Davis L., Mikalová L., Bruisten S., Komericki P., French P., Grant P.R., Pando M.A., Gallo Vaulet L., Fermepin M.R., Martinez A., Centurion Lara A., Giacani L., Norris S.J., Smajs D., Bossshard P.P., González-Candelas F., Nieselt K., and Bagheri H.C. (2016) Origin of modern syphilis and emergence of a pandemic Treponema pallidum cluster. Nature Microbiology, 2: 16245.
- Aufderheide A.C. and Rodriguez-Martin C. (1998) The Cambridge Encyclopedia of Human Paleopathology. Cambridge University Press, Cambridge.
- Baker B.J. (2005) Patterns of pre-and post-Columbian treponematosis in the northeastern United States. In: Powell M.L. and Cook D.C. (eds.), The Myth of Syphilis: The Natural History of Treponematosis in North America. University Press of Florida, Gainesville, pp. 63–76.
- Baker B.J. and Armelagos G.J. (1988) The origin and antiquity of syphilis: paleopathological diagnosis and interpretation. Current Anthropology, 29: 703–738.
- Barnes I. and Thomas M.G. (2006) Evaluating bacterial pathogen DNA preservation in museum osteological collections. Proceedings. Biological Sciences, 273: 645–653.
- Bayliss A., Shepherd Popescu E., Beavan-Athfield N., Bronk-Ramsey C., Cook G.T., and Locker A. (2004) The potential significance of dietary offsets for the interpretation of radiocarbon dates: an archaeologically significant example from medieval Norwich. Journal of Archaeological Science, 31: 563–575.
- Berco C. (2011) Syphilis, sex, and marriage in early modern Spain. Journal of Early Modern History, 15: 223–253.
- Berlinguer G. (1992) The interchange of disease and health between the Old and New Worlds. American Journal of Public Health, 82: 1407–1413.
- Boone P.M., Levy V., and Relucio K.I. (2009) Early syphilis in an HIV-infected man presenting with bone lesions and orbital swelling. Infections in Medicine, 26: 178–183.
- Bouwman A.S. and Brown T.A. (2005) The limits of biomolecular palaeopathology: ancient DNA cannot be used to study venereal syphilis. Journal of Archaeological Science, 32: 703–713.
- Boyd C.P. (2002) The second battle of Covadonga: the politics of commemoration in modern Spain. History and Memory, 14: 37–64.
- Brooks S. and Suchey J.M. (1990) Skeletal age determination based on the os pubis: a comparison of the Acsádi-Nemeskéri and Suchey-Brooks methods. Human Evolution, 5: 227–238.
- Brun J.-P., Dutour O., and Pálfi G. (1998) L’antiquité des tréponématoses dans l’Ancien Monde: évidences historiques, archéologiques et paléopathologiques. Bulletins et Mémoires de la Société d’Anthropologie de Paris, 10: 375–409.
- Buikstra J.E. and Ubelaker D.H. (1994) Standards for Data Collection from Human Skeletal Remains: Proceedings of a Seminar at the Field Museum of Natural History (Arkansas Archeological Report Research Series). Arkansas Archeological Survey, Fayetteville.
- Burstain J.M., Grimprel E., Lukehart S.A., Norgard M.V., and Radolf J.D. (1991) Sensitive detection of Treponema pallidum by using the polymerase chain reaction. Journal of Clinical Microbiology, 29: 62–69.
- Byers S.N. (2005) Attribution of sex. In: Byers S.N. (ed.), Introduction to Forensic Anthropology. Allyn & Bacon, Boston, MA, pp. 151–173.
- Centurion-Lara A., Molini B.J., Godornes C., Sun E., Hevner K., Van Voorhis W.C., and Lukehart S.A. (2006) Molecular differentiation of Treponema pallidum subspecies. Journal of Clinical Microbiology, 44: 3377–3380.
- Cerchiai L., Janelli L., and Longo F. (2004) The Greek Cities of Magna Graecia and Sicily. J. Paul Getty Museum, Los Angeles.
- Clark D. (2010) Germs, Genes, & Civilization: How Epidemics Shaped Who We Are Today. Financial Times Press, Upper Saddle River.
- Codinha S. (2002) Two cases of venereal syphilis from the cemetery of the Igreja do Convento do Carmo (Lisboa). Antropologia Portuguesa, 19: 29–40.
- Cole G. and Waldron T. (2011) Apple Down 152: A putative case of syphilis from sixth century AD Anglo-Saxon England. American Journal of Physical Anthropology, 144: 72–79.
- Cole G. and Waldron H.A. (2012) Letter to the editor: syphilis revisited. American Journal of Physical Anthropology, 149: 149–150.
- Cox M. (2000) Ageing adults from the skeleton. In: Cox M. and Mays S. (eds.), Human Osteology in Archaeology and Forensic Science. Greenwich Medical Media, London, pp. 61–82.
- De Souza S.M., Codinha S., and Cunha E. (2006) The girl from the Church of the Sacrament: a case of congenital syphilis in XVIII century Lisbon. Memórias do Instituto Oswaldo Cruz, 101: 119–128.
- Díaz-Trechuelo L. (1991) Cristóbal Colón, primer Almirante del Mar Océano. Ediciones Palabra DL, Madrid.
- Ehrlich I. and Kricun M.E. (1976) Radiographic findings in early acquired syphilis: case report and cirtical review. American Journal of Roentgenology, 127: 789–792.
- Elmore D. and Phillips F.M. (1987) Accelerator mass spectrometry for measurement of long-lived radioisotopes. Science, 236: 543–550.
- El-Najjar M.Y. (1979) Human treponematosis and tuberculosis: evidence from the New World. American Journal of Physical Anthropology, 51: 599–618.
- Erdal Y.S. (2006) A pre-Columbian case of congenital syphilis from Anatolia (Nicaea, 13th century AD). International Journal of Osteoarchaeology, 16: 16–33.
- Escacena J.L. (2000) Applications of evolutive archaeology: Migrations from Africa to Iberia in the Recent Prehistory. In: Arnaiz-Villena A. (ed.), Prehistoric Iberia: Genetics, Anthropology, and Linguistics. Kluwer Academic/Plenum Publishers, New York, pp. 125–162.
- Farnsworth N. and Rosen T. (2006) Endemic treponematosis: review and update. Clinics in Dermatology, 24: 181–190.
- Gaul J.S., Grossschmidt K., Gusenbauer C., and Kanz F. (2015) A probable case of congenital syphilis from pre-Columbian Austria. Anthropologischer Anzeiger, 72: 451–472.
- Gerbase A.C., Rowley J.T., Heymann D.H., Berkley S.F., and Piot P. (1998) Global prevalence and incidence estimates of selected curable STDs. Sexually Transmitted Infections, 74: 512–517.
- Gonçalves M.L.C., da Silva V.L., de Andrade C.M., Reinhard K., da Rocha G.C., Le Bailly M., Bouchet F., Ferreira L.F., and Araujo A. (2004) Amoebiasis distribution in the past: first steps using an immunoassay technique. Transactions of the Royal Society of Tropical Medicine and Hygiene, 98: 88–91.
- Gould A.B. (1925) Nueva lista documentada de los tripulantes de Colón en 1492. Boletín de la Real Academia de la Historia, 86: 491–532.
- Gurland I., Korn L., Edelman L., and Wallach F. (2001) An unusual manifestation of acquired syphilis. Clinical Infectious Diseases, 32: 667–669.
- Hackett C.J. (1963) On the origin of the human treponematoses (pinta, yaws, endemic syphilis and venereal syphilis). Bulletin of the World Health Organization, 29: 7–41.
- Hackett C.J. (1975) An introduction to diagnostic criteria of syphilis, treponarid and yaws (treponematoses) in dry bones, and some implications. Virchows Archive A: Pathological Anatomy and Histology, 368: 229–241.
- Hackett C.J. (1976) Diagnostic Criteria of Syphilis, Yaws, and Treponarid (Treponematoses) and Some Other Diseases in Dry Bones (for the Use in Osteo-Archaeology). Springer-Verlag, Berlin.
- Harper K.N., Ocampo P.S., Steiner B.M., George R.W., Silverman M.S., Bolotin S., Pillay A., Saunders N.J., and Armelagos G.J. (2008) On the origin of the treponematoses: a phylogenetic approach. PLoS Neglected Tropical Diseases, 2: e148.
- Harper K.N., Zuckerman M.K., Harper M.L., Kingston J.D., and Armelagos G.J. (2011) The origin and antiquity of syphilis revisited: an appraisal of Old World pre-Columbian evidence for treponemal infection. American Journal of Physical Anthropology, 146: 99–133.
- Henneberg M. and Henneberg R.J. (1994) Treponematosis in an Ancient Greek colony of Metaponto, Southern Italy 580–250 BCE. In: Dutour O., Palfi G., Berato J., and Brun J.P. (eds.), The Origin of Syphilis in Europe, Before or After 1493? Centre Archeologique du Var, Éditions Errance, Toulon-Paris, pp. 92–98.
- Hillson S. (1996) Dental Anthropology. Cambridge University Press, New York.
- Holcomb R. (1934) Christopher Columbus and the American origin of syphilis. United States Naval Medical Bulletin, 32: 401–430.
- Huang I., Leach J.L., Fichtenbaum C.J., and Narayan R.K. (2007) Osteomyelitis of the skull in early-acquired syphilis: evaluation by MR imaging and CT. American Journal of Neuroradiology, 28: 307–308.
- Hudson E.H. (1961) Historical approach to the terminology of syphilis. Archives of Dermatology, 84: 545–562.
- Hudson E.H. (1963) Treponematosis and anthropology. Annals of Internal Medicine, 58: 1037–1049.
- Hudson E.H. (1964) Treponematosis and African slavery. British Journal of Venereal Diseases, 40: 43–52.
- Kampmeier R.H. (1984) Early development of knowledge of sexually transmitted diseases. In: Holmes K.K., Mardh P.-A., Sparling P.F., and Wesisner P.J. (eds.), Sexually Transmitted Diseases. McGraw-Hill, New York, pp. 19–29.
- Kang S.H., Park S.W., Kwon K.Y., and Hong W.J. (2010) A solitary skull lesion of syphilitic osteomyelitis. Journal of Korean Neurosurgical Society, 48: 85–87.
- Kinghorn G.R. (2004) Syphilis. In: Cohen J. and Powderly W.G. (eds.), Infectious Diseases, 2nd edn. Elsevier, Saint Louis, MO, pp. 725–727.
- Kolman C.J., Centurion-Lara A., Lukehart S.A., Owsley D.W., and Tuross N. (1999) Identification of Treponema pallidum subspecies pallidum in a 200-year-old skeletal specimen. Journal of Infectious Disease, 180: 2060–2063.
- Lewis A.R. (1991) Nomads and Crusaders, AD 1000–1368. Indiana University Press, Bloomington.
- Little J.W. (2005) Syphilis: an update. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 100: 3–9.
- Lopes L.A. and Cardoso H. (2000) Possível caso de sífilis em fémur e tíbia direitos de um indivíduo proveniente do carneiro da segunda capela da epístola do convento do Carmo de Lisboa (Sécs. XVI–XIX?), Contributos das ciências e das tecnologias para a arqueologia da Península Ibérica, Actas do 3° Congresso de Arqueologia Peninsular ADECAP, Vila Real 1999, Porto, pp. 459–463.
- López B. (2000) Estudio Antropológico de poblaciones históricas de Castilla y León. Tesis Doctoral, Universidad de León, León.
- López Martínez B. (2002) Los pobladores del antiguo Reino de León: Antropometria, Paleodemografía y Paleopatología. Secretariado de Publicaciones Universidad de León, León.
- Lovejoy C.O., Meindl R.S., Pryzbeck T.R., and Mensforth R.P. (1985) Chronological metamorphosis of the auricular surface of the ilium: a new method for the determination of adult skeletal age at death. American Journal of Physical Anthropology, 68: 15–28.
- Lukeš J., Mauricio I.L., Schönian G., Dujardin J.C., Soteriadou K., Dedet J.P., Kuhls K., Tintaya K.W., Jirků M., Chocholová E., Haralambous C., Pratlong F., Oborník M., Horák A., Ayala F.J., and Miles M.A. (2007) Evolutionary and geographical history of the Leishmania donovani complex with a revision of current taxonomy. Proceedings of the National Academy of Sciences of the United States of America, 104: 9375–9380.
- Maat G.J.R. (1993) Bone preservation, decay and its related conditions in ancient human bones from Kuwait. International Journal of Osteoarchaeology, 3: 77–86.
- Mandell G.L., Bennett J.E., and Dolin R. (2009) Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 7th edn. Elsevier Churchill Livingstone, Philadelphia.
- Martínez-Laso J., Gómez-Casado E., Varela P., González-Hevilla M., Alonso-García J., Longás J., and Arnaiz-Villena A. (2000) Genetic and historical relationships among Mediterraneans. In: Arnaiz-Villena A. (ed.), Prehistoric Iberia: Genetics, Anthropology, and Linguistics. Kluwer Academic/Plenum Publishers, New York, pp. 3–32.
- Mays S. (1997) Carbon stable isotope ratios in mediaeval and later human skeletons from northern England. Journal of Archaeological Science, 24: 561–567.
- Mays S., Crane-Kramer G., and Bayliss A. (2003) Two probable cases of treponemal disease of Medieval date from England. American Journal of Physical Anthropology, 120: 133–143.
- Mays S., Vincent S., and Meadows J. (2012) A possible case of treponemal disease from England dating to the 11th–12th century AD. International Journal of Osteoarchaeology, 22: 366–372.
- Meyer C., Jung C., Kohl T., Poenicke A., Poppe A., and Alt K.W. (2002) Syphilis 2001—a palaeopathological reappraisal. HOMO–Journal of Comparative Human Biology, 53: 39–58.
- Mitchell P.D. (2003) Pre-Columbian treponemal disease from 14th century AD Safed, Israel, and implications for the medieval eastern Mediterranean. American Journal Physical Anthropology, 121: 117–124.
- Mitchell P.D. (2009) Technical note: A revised radiocarbon date for a case of treponemal disease from Safed, Israel, from the 15th century AD. American Journal of Physical Anthropology, 139: 274.
- Møller-Christensen V. (1965) New knowledge of leprosy through paleopathology. International Journal of Leprosy, 33: 603–610.
- Monge Soares A. and Alveirinho Dias J. (2007) Reservoir effect of coastal waters off western and northwestern Galicia. Radiocarbon, 49: 925–936.
- Müldner G. and Richards M.P. (2005) Fast or feast: reconstructing diet in later medieval England by stable isotope analysis. Journal of Archaeological Science, 32: 39–48.
- Naranjo P. (1994) On the American Indian origin of syphilis: fallacies and errors. Allergy Proceedings, 15: 89–99.
- Noordhoek G.T., Wieles B., van der Sluis J.J., and van Embden J.D. (1990) Polymerase chain reaction and synthetic DNA probes: a means of distinguishing the causative agents of syphilis and yaws? Infection and Immunity, 58: 2011–2013.
- O’Callaghan J.F. (2013) Reconquest and Crusade in Medieval Spain. University of Pennsylvania Press, Philadelphia.
- Ortner D.J. (2003) Infectious diseases: treponematosis and other bacterial infectious diseases. In: Ortner D.J. (ed.), Identification of Pathological Conditions in Human Skeletal Remains, 2nd edn. Academic Press, San Diego, pp. 273–323.
- Ortner D.J. (2009) Issues in paleopathology and possible strategies for dealing with them. Anthropologischer Anzeiger, 67: 323–340.
- Pardiñas A.F., Martínez J.L., Roca A., García-Vazquez E., and López B. (2014) Over the sands and far away: interpreting an Iberian mitochondrial lineage with ancient Western African origins. American Journal of Human Biology, 26: 777–783.
- Pearce J.M. (1998) A note on the origins of syphilis. Journal of Neurology, Neurosurgery and Psychiatry, 64: 542–547.
- Perine P.L., Hopkins D.R., Niemel P.L.A., St. John R.K., Causse G., and Antal G.M. (1984) Handbook of Endemic Treponematoses: Yaws, Endemic Syphilis and Pinta. World Health Organization, Geneva.
- Polet C. and Katzenberg M.A. (2003) Reconstruction of the diet in a mediaeval monastic community from the coast of Belgium. Journal of Archaeological Science, 30: 525–533.
- Powell M.L. and Cook D.C. (2005) Treponematosis: inquiries into the nature of a protean disease. In: Powell M.L. and Cook D.C. (eds.), The Myth of Syphilis: The Natural History of Treponematosis in North America. University Press of Florida, Gainesville, pp. 9–62.
- Price R. (1979) Spanish medicine in the Golden Age. Journal of the Royal Society of Medicine, 72: 864–874.
- Quétel C. (1990) History of Syphilis. Johns Hopkins University Press, Baltimore, MD.
- Reimer P.J., Baillie M.G.L., Bard E., Bayliss A., Beck J.W., Blackwell P.G., Bronk-Ramsey C., Buck C.E., Burr G.S., Edwards R.L., Friedrich M., Grootes P.M., Guilderson T.P., Hajdas I., Heaton T.J., Hogg A.G., Hughen K.A., Kaiser K.F., Kromer B., McCormac F.G., Manning S.W., Reimer R.W., Richards D.A., Southon J.R., Talamo S., Turney C.S.M., van der Plicht J., and Weyhenmeyer C.E. (2009) IntCal09 and Marine09 radiocarbon age calibration curves, 0–50,000 years cal BP. Radiocarbon, 51: 1111–1150.
- Reinus W.R. (2010) Imaging approach to musculoskeletal infections. In: Bonakdarpour A., Reinus W.R., and Khurana J.S. (eds.), Diagnostic Imaging of Musculoskeletal Diseases: A Systematic Approach. Humana Press, Totowa, NJ, pp. 363–405.
- Resnick D. and Niwayama G. (1995) Osteomyelitis, septic arthritis, and soft tissue infection: organism. In: Resnick D. (ed.), Diagnosis of Bone and Joint Disorders, 3rd edn, Saunders, Philadelphia, PA, pp. 2448–2558.
- Reverte J.M. (1979), Dos Casos de Sífilis Craneal de la Necrópolis de, S. Millán (Segovia). Actas del VI Congreso de Historia de la Medicina, Barcelona.
- Rissech C., Roberts C., Tomás-Batlle X., Tomás-Gimeno X., Fuller B., Fernandez P.L., and Botella M. (2013) A Roman skeleton with possible treponematosis in the north-east of the Iberian Peninsula: a morphological and radiological study. International Journal of Osteoarchaeology, 23: 651–663.
- Rogers J. and Waldron T. (1989) Infections in palaeopathology: the basis of classification according to most probable cause. Journal Of Archaeological Science, 16: 611–625.
- Rothschild B.M. and Rothschild C. (1995) Treponemal disease revisited: skeletal discriminators for yaws, bejel, and venereal syphilis. Clinical Infectious Diseases, 20: 1402–1408.
- Rothschild B.M., Calderon F.L., Coppa A., and Rothschild C. (2000) First European exposure to syphilis: the Dominican Republic at the time of Columbian contact. Clinical Infectious Diseases, 31: 936–941.
- Santos A.L., Gardner M.T., and Allsworth-Jones P. (2013) Treponematosis in Pre-Columbian Jamaica: a biocultural approach to the human cranium found in Bull Savannah. Journal of Archaeological Science, 40: 490–496.
- Schoeninger M.J., DeNiro M.J., and Tauber H. (1983) Stable nitrogen isotope ratios of bone collagen reflect marine and terrestrial components of prehistoric human diet. Science, 220: 1381–1383.
- Schultz M. (2001) Paleohistopathology of bone: a new approach to the study of ancient diseases. Yearbook of Physical Anthropology, 44: 106–147.
- Schwarz S., Skytte L., and Rasmussen K.L. (2013) Pre-Columbian treponemal infection in Denmark? A paleopathological and archaeometric approach. Heritage Science, 1: 19.
- Sefton A. (2001) The Great Pox that was … syphilis. Journal of Applied Microbiology, 91: 592–596.
- Shang H. and Trinkaus E. (2008) An ectocranial lesion on the middle Pleistocene human cranium from Hulu Cave, Nanjing, China. American Journal of Physical Anthropology, 135: 431–437.
- Skinner M. (1994) Osseous treponemal disease: limits on our understanding. In: Dutour O., Pálfi G., Bérato J., and Brun J.P. (eds.), L’origine de la Syphilis en Europe: Avant ou Après 1493? [The Origin of Syphilis in Europe: Before or After 1493?]. Éditions Errance, Paris, pp. 191–201.
- Steinbock R.T. (1976) Paleopathological Diagnosis and Interpretation. Charles, C. Thomas, Springfield, IL.
- Stirland A. (1991) Pre-Columbian treponematosis in medieval Britain. International Journal of Osteoarchaeology, 1: 39–47.
- Stuiver M., Reimer P.J., and Reimer R.W. (2010) CALIB 6.01. WWW program and documentation.
- Thompson R. and Preston R. (1952) Lesions of the skull in secondary syphilis. American Journal of Syphilis, Gonorrhea, and Venereal Diseases, 36: 332–341.
- Tognotti E. (2009) The rise and fall of syphilis in Renaissance Europe. Journal of Medical Humanities, 30: 99–113.
- Tramont E.C. (1995) Syphilis in adults: from Christopher Columbus to Sir Alexander Fleming to AIDS. Clinical Infectious Diseases, 21: 1361–1369.
- Trueman C.N.G., Behrensmeyer A.K., Tuross N., and Weiner S. (2004) Mineralogical and compositional changes in bones exposed on soil surfaces in Amboseli National Park, Kenya: diagenetic mechanisms and the role of sediment pore fluids. Journal of Archaeological Science, 31: 721–739.
- Turner T.B. and Hollander D.H. (1957) Biology of the treponematoses based on studies carried out at the International Treponematosis Laboratory Center of the Johns Hopkins University under the auspices of the World Health Organization. WHO Monograph Series No. 35, Columbia University Press, New York.
- von Hunnius T.E., Roberts C.A., Boylston A., and Saunders S.R. (2006) Histological identification of syphilis in pre-Columbian England. American Journal of Physical Anthropology, 129: 559–566.
- von Hunnius T.E., Yang D., Eng B., Waye J.S., and Saunders S.R. (2007) Digging deeper into the limits of ancient DNA research on syphilis. Journal of Archaeological Science, 34: 2091–2100.
- Waldron T. (2009) Palaeopathology. Cambridge University Press, Cambridge.
- Webb S. (1995) Paleopathology of Aboriginal Australians: Health and Disease across a Hunter-Gatherer Continent. Cambridge University Press, Cambridge.
- Weston D.A. (2009) Brief communication: Paleohistopathological analysis of pathology museum specimens: can periosteal reaction microstructure explain lesion etiology? American Journal of Physical Anthropology, 140: 186–193.
- Zamora J.M.J. (1973) Historia de España: Espana musulmana (711–1031 de, J.C.). Espasa-Calpe, Madrid.
- Zink A.R., Spigelman M., Schraut B., Greenblatt C.L., Nerlich A.G., and Donoghue H.D. (2006) Leishmaniasis in ancient Egypt and upper Nubia. Emerging Infectious Diseases, 12: 1616–1617.