Abstract
Background: There are only limited numbers of reviews on the association of maternal-child genetic polymorphisms and environmental and lifestyle-related chemical exposure during pregnancy with adverse fetal growth. Thus, this article aims to review: (1) the effect of associations between the above highlighted factors on adverse fetal growth and (2) recent birth cohort studies regarding environmental health risks.
Methods: Based on a search of the PubMed database through August 2021, 68 epidemiological studies on gene-environment interactions, focusing on the association between environmental and lifestyle-related chemical exposure and adverse fetal growth was identified. Moreover, we also reviewed recent worldwide birth cohort studies regarding environmental health risks.
Results: Thirty studies examined gene-smoking associations with adverse fetal growth. Sixteen maternal genes significantly modified the association between maternal smoking and adverse fetal growth. Two genes significantly related with this association were detected in infants. Moreover, the maternal genes that significantly interacted with maternal smoking during pregnancy were cytochrome P450 1A1 (CYP1A1), X-ray repair cross-complementing protein 3 (XRCC3), interleukin 6 (IL6), interleukin 1 beta (IL1B), human leukocyte antigen (HLA) DQ alpha 1 (HLA-DQA1), HLA DQ beta 1 (HLA-DQB1), and nicotinic acetylcholine receptor. Fetal genes that had significant interactions with maternal smoking during pregnancy were glutathione S-transferase theta 1 (GSTT1) and fat mass and obesity-associated protein (FTO). Thirty-eight studies examined the association between chemical exposures and adverse fetal growth. In 62 of the 68 epidemiological studies (91.2%), a significant association was found with adverse fetal growth. Across the studies, there was a wide variation in the analytical methods used, especially with respect to the genetic polymorphisms of interest, environmental and lifestyle-related chemicals examined, and the study design used to estimate the gene-environment interactions. It was also found that a consistently increasing number of European and worldwide large-scale birth cohort studies on environmental health risks have been conducted since approximately 1996.
Conclusion: There is some evidence to suggest the importance of gene-environment interactions on adverse fetal growth. The current knowledge on gene-environment interactions will help guide future studies on the combined effects of maternal-child genetic polymorphisms and exposure to environmental and lifestyle-related chemicals during pregnancy.
1. Introduction
One of the rationales for life course epidemiology is the fetal programming hypothesis of the “Developmental Origins of Health and Disease (DOHaD)” theory. The fetal programming hypothesis proposed by Dr. David Barker [1] is based on the results of epidemiological studies in the United Kingdom that children born with low birth weights have a higher risk of diabetes and metabolic syndromes in adulthood [2, 3]. The “first thousand days of life after conception” includes the periods in utero period that usually lasts for about nine months, as well as the first two years after birth (i.e., 9 months × 30 days/month + 365 days/year × 2 years = 1,000 days). This is the period during which susceptibility to non-communicable diseases (NCDs) in later life is programmed [4]. Furthermore, the chemical exposure during the “first thousand days of life after conception” is associated with the formation of organs [5], the neurological system [5], the urogenital system [6], the reproductive system [7], and the respiratory system [8].
Adverse fetal growth, such as low birth weight (LBW), preterm birth (PB), small-for-gestational-age (SGA) fetuses, and intrauterine growth restriction (IUGR), is indicators of fetal growth that are affected by exposure to environmental and lifestyle-related chemicals. LBW and PB have been estimated to contribute to 36% of the infant mortality that occurred in 2013 [9]. These two outcomes have been associated with an increased risk of chronic adverse health conditions throughout infancy, childhood, and adulthood [10–12]. As adverse fetal growth serves both as indicators of fetal growth and predictors of the postnatal growth index, it is important for environmental epidemiologists to examine the association between the fetal environment and adverse fetal growth. In the recent reports, the heritability of birth weight, gestational age, SGA fetuses, PB, and LBW from the maternal genetic contribution ranges from approximately 15–42% [13–18]. Both genetic factors and environmental factors during pregnancy, such as smoking, alcohol consumption, and chemical exposure, predict adverse health effects at birth. However, gene-environment interaction studies may help to identify subgroups of women and children that are at a high risk of adverse health outcomes at birth. The results of these studies can contribute to preventive medicine in maternal-child and environmental health. Interestingly, the results of epidemiological studies on environmental and lifestyle-related chemicals during pregnancy indicate the existence of related gene-environment interactions. However, gene-environment interaction studies, with hypotheses aiming to identify new genetic or environmental factors, are scarce. In this review, we summarize and discuss the current findings related to the gene-environment interactions related to the environmental and lifestyle-related chemicals identified in adverse fetal growth. Moreover, we also reviewed recent birth cohort studies regarding environmental health risks.
2. Search methods
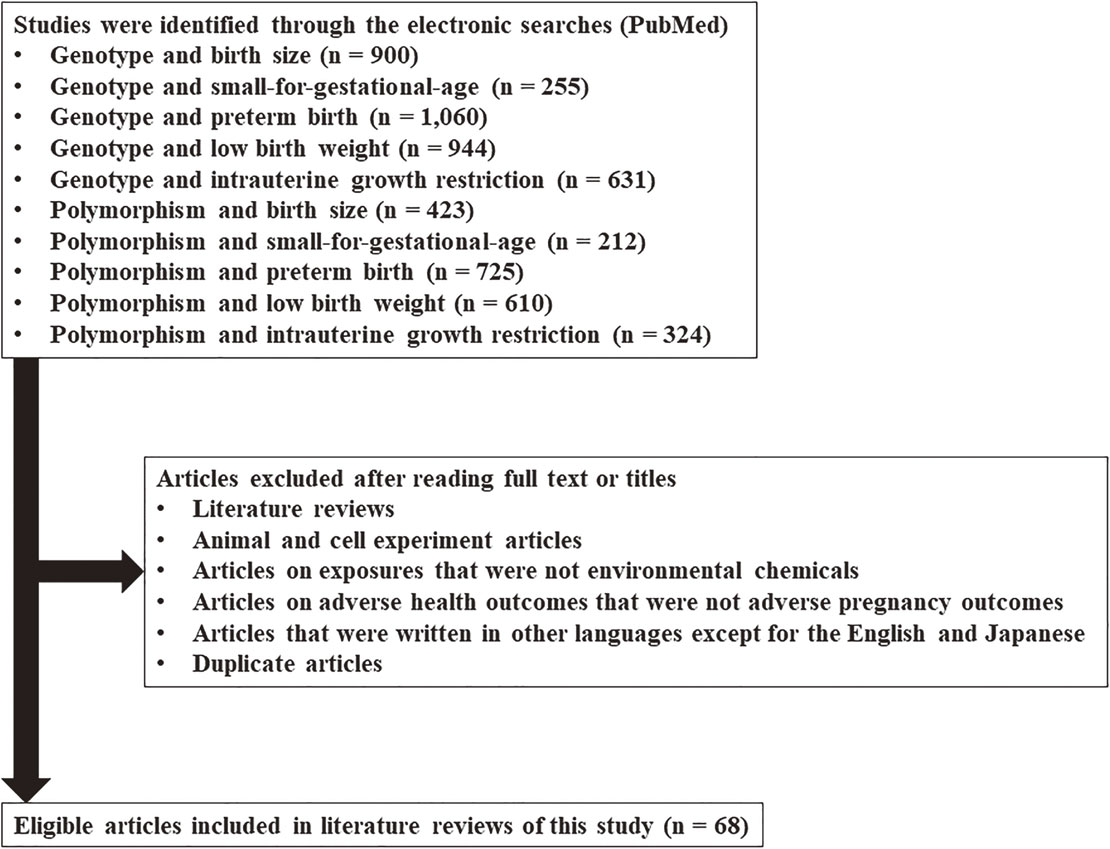
Electronic searches were performed using PubMed. There were no limits set for language, year of publication, or publication status. The genetic-related keywords used were “genotype” and “polymorphism.” The keywords related to adverse fetal growth were: “birth size,” “small-for-gestational-age,” “preterm birth,” “low birth weight,” and “intrauterine growth restriction.” Search keywords were designed using a combination of one genetic keyword and one adverse fetal growth keyword with the condition “AND.” After viewing the search results, certain articles were excluded; these included literature reviews; articles on animal and cell experiments, exposures to non-environmental chemicals, non-lifestyle-related chemicals, adverse health outcomes other than adverse fetal growth; articles that were written in languages other than English or Japanese; and duplicate articles. Finally, 68 studies on gene-environment interactions that focused on the association between environmental and lifestyle-related chemical exposure and adverse fetal growth were identified (Fig. 1).
3. Gene-environment interaction studies
To describe the current state of gene-environment interaction studies on the topic of environmental and lifestyle-related chemical exposure, we have summarized the study designs; measurements of environmental and lifestyle-related chemicals; and main findings.
3.1. Study design and measurement of environmental and lifestyle-related chemicals
The study designs varied across the selected studies, as they included case-control studies [19–39], birth cohort studies [40–71], nested case-control studies [72–77], cross-sectional studies [78–83], collaborations of birth cohort studies [84–86], and a case study [87]. The types of environmental and lifestyle-related chemicals assessed were diverse. Twenty-seven studies used questionnaires to investigate the type of maternal smoking during pregnancy (also see Tables 1 to 5), including maternal active smoking, passive smoking, or secondhand smoking [20, 23, 25, 27, 31, 34, 36, 38–40, 46, 56, 60–62, 68, 70, 73, 74, 79, 80, 82–87]. Three studies examined the biomarker levels related to maternal smoking including cotinine levels [47, 49, 51]. Thirty-eight other studies observed the outcomes of chemical exposure during pregnancy (also see Supplementary Tables 1 to 5), including exposure to particulate matter (PM) of 2.5 microns or less in diameter (PM2.5) [65], PM of 10 microns or less in diameter (PM10) [66], household air pollution (HAP) [67], air quality index (AQI) [77], benzo(a)pyrene [43], nitrogen oxides (NOx) [57–59], acrylamides [45], caffeine [28, 63], metals [42, 48, 53, 54, 75, 81], soluble mica [35], pesticides [22, 32, 44], perfluorinated compounds [52], dioxins [41, 50], disinfection by-products [21, 26, 29, 69, 71, 72, 76], parabens [64], phenols [55], alcohol [19, 24], floriculture work [30], phthalates [37], and folates [81]. This present study especially focuses on exposure to smoking during pregnancy.
Table 1 Maternal smoking during pregnancy and associated reduction of birth weight
| Location |
Study design and participants |
Environmental exposure |
Genetic polymorphism of mother or child (dbSNP ID) |
Mother or child risk genotype |
Reduction of birth weight |
Reference |
| China |
Case-control
(n = 741) |
Smoking |
CYP1A1 MspI (rs4646903; mother) |
m1/m2 or m2/m2 |
520 g ↓ |
Wang et al. [36] |
| Japan |
Birth cohort
(n = 293) |
Smoking |
CYP1A1 MspI (rs4646903; mother) |
m1/m2 or m2/m2 |
170 g ↓ |
Sasaki et al. [61] |
| Japan |
Birth cohort
(n = 3,263) |
Smoking (based on cotinine) |
CYP1A1 Ile462Val (rs1048943; mother) |
AG or GG |
62 g ↓ |
Kobayashi et al. [49] |
| China |
Case-control
(n = 741) |
Smoking |
GSTM1 non-null/null (mother) |
Null |
642 g ↓ |
Wang et al. [36] |
| Japan |
Birth cohort
(n = 293) |
Smoking |
GSTM1 non-null/null (mother) |
Null |
171 g ↓ |
Sasaki et al. [61] |
| United States |
Birth cohort
(n = 502) |
Smoking |
GSTT1 non-null/null (mother) |
Null |
190 g ↓ |
Aagaard-Tillery et al. [40] |
| United States |
Case-control
(n = 1,671) |
Smoking |
GSTT2 non-null/null (mother) |
Null |
284 g ↓ |
Zheng et al. [39] |
| Lithuania |
Nested case-control
(n = 646) |
Smoking |
GSTM1 non-null/null (mother) and GSTT1 non-null/null (mother) |
GSTM1-null and GSTT1-null |
311 g ↓ |
Grazuleviciene et al. [74] |
| Lithuania |
Case-control
(n = 543) |
Smoking |
GSTM1 non-null/null (mother) and GSTT1 non-null/null (mother) |
GSTM1-null and GSTT1-null |
311 g ↓ |
Danileviciute et al. [23] |
| Japan |
Birth cohort
(n = 293) |
Smoking |
AHR Arg554Lys (rs2066853; mother) |
Arg/Arg |
211 g ↓ |
Sasaki et al. [61] |
| Japan |
Birth cohort
(n = 3,263) |
Smoking (based on cotinine) |
AHR Arg554Lys (rs2066853; mother) |
GG |
62 g ↓ |
Kobayashi et al. [49] |
| Japan |
Birth cohort
(n = 293) |
Smoking |
AHR Arg554Lys (rs2066853; mother) and CYP1A1 MspI (rs4646903; mother) |
AHR-Arg/Arg and CYP1A1-m1/m2 or m2/m2 |
315 g ↓ |
Sasaki et al. [61] |
| Japan |
Birth cohort
(n = 293) |
Smoking |
AHR Arg554Lys (rs2066853; mother) and GSTM1 non-null/null (mother) |
AHR-Arg/Arg and GSTM1-null |
237 g ↓ |
Sasaki et al. [61] |
| Japan |
Birth cohort
(n = 460) |
Smoking |
NQO1 Pro185Ser (rs1800566; mother) |
Pro/Pro |
199 g ↓ |
Sasaki et al. [62] |
| Japan |
Birth cohort
(n = 460) |
Smoking |
CYP2E1*5 (rs2031920; mother) |
c1/c1 or c1/c2 |
195 g ↓ |
Sasaki et al. [62] |
| Turkey |
Cross-sectional
(n = 61) |
Smoking |
OGG1 Ser326Cys (rs13181; mother) |
CG or GG |
406 g ↓ |
Karahalil et al. [80] |
| Japan |
Birth cohort
(n = 1,784) |
Smoking |
MTHFR A1298C (rs1801131; mother) |
AA |
107 g ↓ |
Yila et al. [70] |
| Japan |
Birth cohort
(n = 3,263) |
Smoking (based on cotinine) |
XRCC1 Arg194Trp (rs.1799782; mother) |
CT or TT |
59 g ↓ |
Kobayashi et al. [49] |
| Japan |
Birth cohort
(n = 3,263) |
Smoking (based on cotinine) |
XRCC1 Gln399Trp (rs25487; mother) |
GA or AA |
46 g ↓ |
Kobayashi et al. [49] |
| Italy |
Cross-sectional
(n = 584) |
Smoking |
Haptoglobin (Hp) 2 (rs72294371; mother) |
*2 |
Association observed |
Gloria-Bottini et al. [79] |
| United Kingdom |
Cross-sectional
(n = 552) |
Smoking |
HLA-DQA1 (rs2187668; mother) |
*0101 |
Interaction observed |
Taylor et al. [83] |
| United Kingdom |
Cross-sectional
(n = 552) |
Smoking |
HLA-DQB1 (mother) |
*0201 |
Interaction observed |
Taylor et al. [83] |
| Europe |
Birth cohort
(n = 3,563) |
Smoking |
15q25 nicotinic acetylcholine receptor (rs1051730; mother) |
No report |
Interaction observed |
Leermakers et al. [56] |
| Europe |
12 birth cohorts
(n = 26,241) |
Smoking |
15q25 nicotinic acetylcholine receptor (rs1051730; mother) |
No report |
Interaction observed |
Tyrrell et al. [86] |
| Europe |
2 birth cohorts
(n = 8,621) |
Smoking |
15q25 nicotinic acetylcholine receptor (rs1051730; mother) |
No report |
In the Mendelian randomization analysis using maternal rs1051730 genotype as an instrument for smoking quantity, association observed (Reduction of estimated fetal weight) |
Brand et al. [84] |
| Japan |
Birth cohort
(n = 3,263) |
Smoking (based on cotinine) |
AHR Arg554Lys (rs2066853; mother), CYP1A1 Ile462Val (rs1048943; mother), and XRCC1 Arg194Trp (rs1799782; mother) |
AHR-GG, CYP1A1-AG/GG, and XRCC1-CT/TT |
145 g ↓ |
Kobayashi et al. [49] |
| United States |
Birth cohort
(n = 502) |
Smoking |
GSTT1 non-null/null (child) |
Null |
262 g ↓ |
Aagaard-Tillery et al. [40] |
| Italy |
Cross-sectional
(n = 360) |
Smoking |
ADA (child) |
*1 |
255 g ↓ |
Gloria-Bottini et al. [78] |
| Europe |
2 birth cohorts
(n = 3,512) |
Smoking |
FTO (rs9939609; child) |
AA |
Interaction observed |
Marsh et al. [85] |
| Korea |
Birth cohort
(n = 266) |
Environmental tobacco smoke (ETS) |
GSTT1 non-null/null (mother) |
Null |
236 g ↓ |
Hong et al. [46] |
| China |
Birth cohort
(n = 1,338) |
Passive smoking |
EPHX1 Tyr113His (rs1051740; mother) |
His/His |
316 g ↓ |
Wu et al. [68] |
| Japan |
Birth cohort
(n = 3,263) |
Cotinine (dose-dependent association) |
AHR Arg554Lys (rs2066853; mother) |
GG |
Dose-dependent association observed |
Kobayashi et al. [51] |
| Japan |
Birth cohort
(n = 3,263) |
Cotinine (dose-dependent association) |
XRCC1 Arg194Trp (rs1799782; mother) |
TT |
Dose-dependent association observed |
Kobayashi et al. [51] |
↓: reduction.
Table 2 Maternal smoking during pregnancy and increased risk of low birth weight (LBW)
| Location |
Study design and participants |
Environmental exposure |
Genetic polymorphism of mother or child (dbSNP ID) |
Mother or child risk genotype |
Increased risk of LBW |
Reference |
| Lithuania |
Nested case-control
(n = 646) |
Smoking |
GSTM1 non-null/null (mother) |
Null |
No association observed |
Grazuleviciene et al. [73] |
| Lithuania |
Nested case-control
(n = 646) |
Smoking |
GSTT1 non-null/null (mother) |
Null |
No association observed |
Grazuleviciene et al. [73] |
Table 3 Maternal smoking during pregnancy and increased risk of preterm birth (PB)
| Location |
Study design and participants |
Environmental exposure |
Genetic polymorphism of mother or child (dbSNP ID) |
Mother or child risk genotype |
Increased risk
of PB |
Reference |
| United States |
Case-control
(n = 1,030) |
Smoking |
CYP1A1 MspI (rs4646903; mother) |
m1/m2 or m2/m2 |
Interaction observed |
Tsai et al. [34] |
| United States |
Birth cohort
(n = 954) |
Smoking |
GSTT1 non-null/null (mother) or GSTT1 non-null/null (child) |
Null (mother) or null (child) |
Odds ratio = 4.0 |
Nukui et al. [60] |
| United States |
Birth cohort
(n = 954) |
Smoking |
GSTT1 non-null/null (mother) and GSTT1 non-null/null (child) |
Null (mother) and null (child) |
Odds ratio = 7.2 |
Nukui et al. [60] |
| United States |
Case-control
(n = 1,749) |
Smoking |
CYP1A1 MspI (rs4646903; mother) and GSTT1 non-null/null (mother) |
CYP1A1-m1/m2 or m2/m2 and GSTT1-null |
Odds ratio = 5.8 |
Tsai et al. [33] |
| United States |
Case study
(n = 227) |
Smoking |
MDM4 (rs1090595; mother) |
AC |
Odds ratio = 1.4
(Both IUGR and PB) |
Huang et al. [87] |
| United States |
Case study
(n = 227) |
Smoking |
TP53 (rs8079544; mother) |
CT |
Odds ratio = 1.7
(Both IUGR and PB) |
Huang et al. [87] |
| Uruguay |
Case-control
(n = 251) |
Smoking |
IL6 (rs1800795; mother) |
No report |
Interaction observed |
Pereyra et al. [31] |
| Uruguay |
Case-control
(n = 251) |
Smoking |
IL1B (rs16944; mother) |
No report |
Interaction observed |
Pereyra et al. [31] |
| Croatia |
Case-control
(n = 324) |
Smoking (before pregnancy) |
DNMT3B (rs1569686; mother) |
TT |
Odds ratio = 6.9 |
Barisic et al. [20] |
IUGR: intrauterine growth restriction.
Table 4 Maternal smoking during pregnancy and increased risk of intrauterine growth restriction (IUGR)
| Location |
Study design and participants |
Environmental exposure |
Genetic polymorphism of mother or child (dbSNP ID) |
Mother or child risk genotype |
Increased risk of IUGR |
Reference |
| United Kingdom |
Case-control
(n = 270) |
Smoking |
CYP1A1 MspI (rs4646903; mother) |
m1/m2 or m2/m2 |
Odds ratio = 3.2 |
Delpisheh et al. [25] |
| United Kingdom |
Case-control
(n = 270) |
Smoking |
GSTM1 non-null/null (mother) |
Null |
Odds ratio = 4.1 |
Delpisheh et al. [25] |
| United Kingdom |
Case-control
(n = 270) |
Smoking |
GSTT1 non-null/null (mother) |
Null |
Odds ratio = 4.3 |
Delpisheh et al. [25] |
| United States |
Case study
(n = 227) |
Smoking |
MDM4 (rs1090595; mother) |
AC |
Odds ratio = 1.38 (Both IUGR and PB) |
Huang et al. [87] |
| United States |
Case study
(n = 227) |
Smoking |
TP53 (rs8079544; mother) |
CT |
Odds ratio = 1.66 (Both IUGR and PB) |
Huang et al. [87] |
| United Kingdom |
Cross-sectional
(n = 497) |
Smoking |
NQO1 Pro187Ser (rs1800566; child) |
Pro/Pro |
Association observed |
Price et al. [82] |
PB: preterm birth.
Table 5 Maternal smoking during pregnancy and increased risk of small-for-gestational-age (SGA) fetuses
| Location |
Study design and participants |
Environmental exposure |
Genetic polymorphism of
mother or child (dbSNP ID) |
Mother or child risk genotype |
Increased risk of SGA |
Reference |
| Canada |
Case-control
(n = 965) |
Smoking |
CYP1A1 (rs4646903; mother) |
*2A |
Interaction observed |
Infante-Rivard et al. [27] |
| Canada |
Case-control
(n = 965) |
Smoking |
XRCC3 Thr241Met (rs861539; mother) |
Thr/Met or Met/Met |
Interaction observed |
Infante-Rivard et al. [27] |
| Canada |
Case-control
(n = 965) |
Smoking |
GSTT1 non-null/null (child) |
Null |
Interaction observed |
Infante-Rivard et al. [27] |
| China |
Case-control
(n = 468) |
Second-hand smoke |
CYP2A6*4 (mother) |
*1/*4 or *4/*4 |
Odds ratio = 2.0 |
Xie et al. [38] |
| China |
Case-control
(n = 468) |
Second-hand smoke |
CYP2A6*4 (mother) and GSTT1 non-null/null (mother) |
CYP2A6-*1/*4 or *4/*4 and GSTT1-null |
Odds ratio = 2.5 |
Xie et al. [38] |
| Taiwan |
Birth cohort
(n = 328) |
Cotinine |
GSTM1 non-null/null (mother) |
Null |
Odds ratio = 5.7 |
Huang et al. [47] |
| Taiwan |
Birth cohort
(n = 328) |
Cotinine |
GSTT1 non-null/null (mother) |
Null |
Odds ratio = 7.6 |
Huang et al. [47] |
| Taiwan |
Birth cohort
(n = 328) |
Cotinine |
GSTM1 non-null/null (mother) and GSTT1 non-null/null (mother) |
GSTM1-null and GSTT1-null |
Odds ratio = 8.9 |
Huang et al. [47] |
Nineteen studies found significantly decreased birth size or observed gene-environment interactions on birth size [18, 23, 36, 39, 40, 46, 49, 51, 56, 61, 62, 70, 74, 79, 80, 83–86]. Eleven studies found significantly increased risks or observed gene-environment interactions related to PB, SGA fetuses, and IUGR [20, 25, 27, 31, 33, 34, 38, 47, 60, 82, 87]. The significant maternal genotypes detected were cytochrome P450 (CYP) 1A1 (CYP1A1; MspI) m1/m2 and m2/m2 [28, 34, 36, 61], CYP1A1 (Ile462Val) AG/GG [49], glutathione S-transferase (GST) mu 1 (GSTM1) null [25, 36, 47, 61], GST theta 1 (GSTT1) null [25, 40, 47, 60], GST theta 2 (GSTT2) null [39], aryl hydrocarbon receptor (AHR) (Arg554Lys) Arg/Arg or GG [49, 61], NAD[P]H quinone dehydrogenase 1 (NQO1; Pro185Ser) Pro/Pro [62], CYP2E1*5 [62], 8-oxoguanine glycosylase 1 (OGG1; Ser326Cys) CG/GG [80], methylenetetrahydrofolate reductase (MTHFR; A1298C) AA [70], X-ray repair cross-complementing protein 1 (XRCC1; Arg194Trp) CT/TT [49], XRCC1 (Gln399Trp) GA/AA [49], murine double minute 4 (MDM4; rs1090595) AC [87], tumor protein p53 (TP53) CT [87], haptoglobin 2 (Hp2)*2 [79], DNA [cytosine-5-]-methyltransferase 3 beta (DNMT3B; rs1569686) TT [20], epoxide hydrolase 1 (EPHX1; Tyr113His) His/His [68], CYP2A6*1/*4 and CYP2A6*4/*4 [38]. The significant infant genotypes detected were GSTT1 null [40] and NQO1 (Pro187Ser) Pro/Pro [82]. The detected maternal genes that significantly interacted with maternal active or passive smoking during pregnancy were CYP1A1 (MspI) [34], CYP1A1*2A [27], X-ray repair cross-complementing protein 3 (XRCC3; Thr241Met) [27], interleukin 6 (IL6; rs1800795) [31], interleukin 1 beta (IL1B; rs16944) [31], human leukocyte antigen (HLA) DQ alpha 1 (HLA-DQA1)*0101 [83], HLA DQ beta 1 (HLA-DQB1)*0201 [83], and nicotinic acetylcholine receptor (rs1051730) [56, 86]. Fetal genes that had significant interactions with maternal active smoking during pregnancy were GSTT1 [27] and fat mass and obesity-associated protein (FTO) (rs9939609) [85]. One study found that the effects of an increased risk of LBW were nonsignificant, but there was a significant decrease in birth weight [73].
4. Literature gaps, current birth cohort studies, and future directions
4.1. Literature gaps
This review shows that there are many kinds of gene-environment interactions between different types of environmental and lifestyle-related chemical exposure during pregnancy and adverse fetal growth. Additionally, the authors have previously observed gene-chemical interactions between health conditions before delivery and adverse health outcomes in children after birth in the Hokkaido Study on Environment and Children’s Health (hereafter, the Hokkaido Study), a prospective birth cohort study, in Japan [49–51, 61–63, 70, 88–97] (Supplementary Table 6). However, there is limited information worldwide that can be reliably used for the purposes of early risk assessment, predictions, and chemical precaution. In research on environmental and lifestyle-related chemical exposure during pregnancy, various environmental and lifestyle-related chemicals interact to adversely affect fetal growth.
It has been hypothesized that environmental and lifestyle-related chemical exposure in the fetal period and in early postnatal life leads to a higher risk of NCDs in adulthood. Thus far, many previous epidemiological studies have only focused on children or adults in limited periods of time. It is, thus, critical to perform prospective birth cohort studies focused on the course of human life to examine the chronical health effects of identified environmental risk factors in the long term.
Given that environmental and lifestyle-related chemical exposure during pregnancy involves complex biological mechanisms related to adverse fetal growth and chronic adverse health conditions in infancy, childhood, and adulthood, life course epidemiology is the best available approach for identifying the gene-environment interactions related to these outcomes.
4.2. Current epidemiological studies using birth cohorts to study gene-environment interactions
Until a few decades ago, it was difficult to analyze large amounts of data for a single genetic polymorphism. However, the widespread use of genetic evaluation methods, such as genome-wide association studies, as well as reduced costs of genetic evaluation have made it possible to obtain data on hundreds of thousands of genetic polymorphisms for a large number of study participants. However, it remains difficult to obtain data on environmental and lifestyle-related chemical exposure for a large number of participants due to the high costs of environmental evaluation and measurement technology. Nonetheless, it is expected that it will be possible in the future to obtain environmental exposure data for a large number of participants by disseminating environmental evaluation methods, reducing evaluation costs, and developing statistical methods.
A large number of candidate genes addressing the association between environmental and lifestyle-related chemical exposure during pregnancy and adverse fetal growth have been previously studied, but the results have been inconsistent. The identification, validation, and verification of gene-environment interactions require a large birth cohort with a significant number of DNA samples from mothers and children. Collaborative studies of small cohorts including DNA samples are needed as well. Currently, large-scale birth cohort and birth cohort collaborative studies are ongoing worldwide to assess environmental health risks. We introduce their current statuses below.
4.2.1. Birth cohort consortiums and large birth cohorts addressing environmental health risks in Europe
Because studies that utilize a single cohort to study the effects of environmental and lifestyle-related chemical exposure on genetic susceptibility to diseases are not comprehensive with regard to the entire human population, cohort studies with a large sample size have been launched, and certain single cohorts have been combined.
The Danish National Birth Cohort (DNBC) and the Norwegian Mother and Child Cohort Study (MoBa) are two large, famous birth cohorts in Europe that study environmental health risks. In 1996, the DNBC began by recruiting approximately 100,000 women that were early in pregnancy and by 1999 the project covered all regions of Denmark [98]. A major feature of the DNBC is its focus on exposure to maternal alcohol consumption, coffee intake, smoking, nicotine substitute usage, and exposure to possible environmental toxins [99]. MoBa began in 1999 and consists of more than 120,000 pregnant women [100, 101]. A major feature of MoBa is its focus on detecting gene-environment interactions through environmental exposure [100, 101]. Genetic analysis has been performed in both the DNBC [102] and the MoBa [103] studies.
Approximately one decade after the establishment of DNBC and MoBa, a movement of collaboration and consortium of small European birth cohorts focused on environmental health risks began. In particular, the Environmental Health Risks in European Birth Cohorts (ENRIECO) project is one of the oldest pioneering projects in which many birth cohorts sought an integrated assessment of environmental health risks. ENRIECO is a collaborative cohort consortium started in 2009 that consists of 37 cohort studies following more than 350,000 mother-child pairs in 19 European countries [104, 105]. A major feature of this project is its focus on a variety of environmental exposures, such as air pollution, water contamination, numerous chemicals, radiation, noise, and occupational hazards [104]. The success of ENRIECO has also led to the launch of other birth cohort consortiums. The “Long-term Exposure to Air Pollution and Pregnancy Outcomes” (LEAP) study in Italy includes 211,853 mother-child pairs from 2007–2013 population-based birth cohorts and it was established to more accurately examine the levels of air pollution exposure [106]. The LifeCycle Project, which began in 2017 and includes over 250,000 mother-child pairs in a birth cohort network of 11 European countries, aims to identify the novel markers of early-life stressors that affect health trajectories throughout the life course [107]. The major features of the LifeCycle Project are its focus on lifestyle and urban environmental exposures and the elucidation of epigenetic pathways [107]. At present, there are few reports on gene-environment association using the genetic analysis of ENRIECO, LEAP, and the LifeCycle Project.
4.2.2. Birth cohort consortiums and large birth cohorts assessing environmental health risks in the United States, Canada, and the Caribbean
The history of birth cohort cooperation and large birth cohort studies on environmental health risks began in the United States about 10 years before the establishment of the ENRIECO project in Europe. To discover environmental health risks and consequently prevent disease in children, the United States Congress enacted the Children’s Health Act of 2000, which directed the National Institute of Child Health and Human Development to conduct the National Children’s Study (NCS) [108–110]. The NCS was to be conducted in a nationally representative, prospective cohort of 100,000 children, which would be followed from conception to 21 years of age [108–110]. As a pilot study to assess the feasibility of the NCS, the Vanguard Study was started in 2007, enrolling approximately 5,000 children in 40 counties across the United States [108, 109]. General recruitment for the NCS was supposed to complete in 2014 [110]. The major features of the NCS were its focus on chemical exposures and the elucidation of gene-environment interactions [108–110]. However, the NCS was ended in 2014 because its study design was not feasible [110]. However, the interest in ENRIECO and NCS led to the launch of other birth cohort consortiums in Canada. In 2010, a collaborative study between Canada and India called the South Asian Birth Cohort Study (START) was established to investigate the environmental and genetic bases of adiposity in children up to five years of age among 750 South Asian children recruited from highly divergent environments, namely urban Canada and rural and urban India [111]. A major feature of START is its focus on exposure to maternal smoking and diet, its interest in gene-environment interactions related to childhood obesity, and its targeting of South Asian populations [111]. At present, there are few reports on gene-environment association using the genetic analysis of START. Similar studies have been performed in the United States and the Caribbean. Following the end of the NCS, the Environmental Influences on Child Health Outcomes (ECHO) program, a collaborative consortium of 81 birth cohorts of over 90,000 participants in the United States, was established in 2016 to evaluate the rates of childhood asthma incidence due to environmental factors [112]. However, few studies on gene-environment association using the genetic analysis of the ECHO program have been reported thus far. In addition, the Children’s Respiratory and Environmental Workgroup (CREW), a collaborative consortium of 12 birth cohorts of over 50,000 participants in the United States, has been established to evaluate the risks of childhood asthma and airway diseases due to prenatal and early-life environmental exposures, including genetic analysis [113, 114]. The major features of ECHO and CREW are their focus on pollutant and toxin exposure and their elucidation of genetic effects such as epigenetic pathways [110, 111].
In the Republic of Suriname, which is located on the northeastern coast of South America and is bordered by Brazil, Guyana, French Guiana, and the Atlantic Ocean, the Caribbean Consortium for Research in Environmental and Occupational Health (CCREOH) cohort study aims to use a cumulative risk approach to examine the impact of exposure to organic and inorganic neurotoxicants, including mercury, lead, and multiple organophosphate pesticides, on 1,200 Surinamese pregnant women and their offspring [115]. The major feature of the CCREOH study is its focus on numerous organic and inorganic toxicants exposures [115]. Genetic analysis has not been performed in the CCREOH study.
4.2.3. Birth cohort consortiums and large birth cohorts assessing environmental health risks in Asia
In Asia, the history of large birth cohort consortiums and large birth cohorts on environmental health risks began in Japan, Korea, and continent-wide at roughly the same time as the establishment of the ENRIECO project in Europe. In particular, the Japan Environment and Children’s Study (JECS), a nationwide birth cohort study that started its recruitment in 2011 and has included approximately 100,000 mothers, is ongoing to elucidate the environmental factors that affect children’s health and development [116–118]. The Korean Children’s Environmental Health Study (Ko-CHENS), a nationwide birth cohort study that started its recruitment in 2015 and has included approximately 65,000 mothers, is ongoing to examine the relationship between environmental exposures and adverse health effects [119]. The major features of these two birth cohorts are their focus on environmental and lifestyle-related chemical exposures and gene-environment interactions related to adverse health outcomes [116, 119]. Genetic analysis has not been performed in both the JECS and the Ko-CHENS studies.
The Birth Cohort Consortium of Asia (BiCCA), which consists of over 30 birth cohorts in more than 15 Asian countries, was established in 2011 [120] through the cooperation of the Taiwan Birth Panel Study (TBPS) in Taiwan [121], the Mothers and Children’s Environmental Health Study (MOCEH) in Korea [122], and the Hokkaido Study in Japan [92, 93]. A major feature of BiCCA is its focus on a variety of adverse health outcomes in pregnancy and after birth [117]. Genetic analysis has been performed in the TBPS [123] and the MOCHE [124] studies but not in the BiCCA studies.
The Japan Birth Cohort Consortium (JBiCC) was established in 2019 by the Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study (TMM BirThree Cohort Study) in Miyagi and Iwate [125], the Chiba Study of Mother and Children’s Health (C-MACH) in Chiba [126], the Child Health and Development Birth Cohort (Seiiku Boshi Cohort) of the National Center for Child Health and Development in Tokyo [127], the Hamamatsu Birth Cohort for Mothers and Children (HBC) Study in Shizuoka [128], the babies’ and their parents’ longitudinal observation in Suzuki Memorial Hospital on Intrauterine period (BOSHI) study in Miyagi [129], and the Hokkaido Study in Hokkaido [92, 93]. The major features of the JBiCC are its focus on a variety of adverse health outcomes in Japanese children and its methods of validating the study results from a specific birth cohort using another birth cohort. Genetic analysis, including epigenetic analysis, has been performed in the TMM BirThree [130] and C-MACH [131] studies, while such analyses have not been performed in the Seiiku Boshi Cohort, HBC, and BOSHI studies.
4.3. Future directions
In the future, it will be possible to use big data on birth cohorts to further investigate gene-environment interactions. In addition, replication and validation using a large sample size is crucial for the interpretation of results from epidemiological studies on gene-environment interactions.
Future studies on the gene-environment interactions related to birth outcomes and chronic adverse health conditions in infancy, childhood, and adulthood hold tremendous promise for precision medicine [132–134], precision public health [135–137], and preemptive medicine which is a novel medical concept that has been proposed in Japan [138, 139] (Fig. 2).

Our current knowledge supports the understanding that adverse fetal growth is caused by a complex interplay of multiple factors, including environmental exposures, genetic factors, and gene-environment interactions. Therefore, studies that only deal with one or two factors at a time will not be able to fully examine the biological mechanisms underlying the development of adverse fetal growth. This demonstrates the need for large-scale prospective birth cohort studies to identify the relationships between exposure to as during pregnancy, mother-child genetic susceptibility, and the development of child outcomes at birth and after birth. The identification of these key risk factors will allow us to gain important insights into the biological mechanisms by which environmental exposures and genetic susceptibility affect certain biological functions, as well as the risk of certain adverse health outcomes at birth and after birth. The identification of these mechanisms will contribute to the development of new paradigms for public health and precautions for adverse health outcomes at birth and after birth.
5. Conclusion
This review was conducted in an attempt to understand the state of the science on gene-environment interactions as they relate to adverse fetal growth, with a particular focus on environmental and lifestyle-related chemical exposure during pregnancy. A total of 68 epidemiological studies were identified, with 62 finding evidence to suggest gene-environment interactions related to adverse fetal growth. However, some of the findings were contradictory, which may have been due to differences in the levels of environmental exposure, the participant sample sizes, and the study designs used to test for gene-environment interactions.
We hope that the current knowledge of gene-environment interactions will help guide further studies on the joint effects of mother-child genetic factors and exposure to environmental and lifestyle-related chemicals during pregnancy. We hope that this knowledge will assist in precision medicine, preemptive medicine, and precision public health to reduce the adverse health effects in populations including high-risk groups as much as possible.
Abbreviations
BiCCA
Birth Cohort Consortium of Asia
BrTHM
brominated trihalomethane
CCREOH
Caribbean Consortium for Research in Environmental and Occupational Health
C-MACH
Chiba Study of Mother and Children’s Health
CREW
Children’s Respiratory and Environmental Workgroup
CYP
cytochrome P450
DNA
deoxyribonucleic acid
DNBC
Danish National Birth Cohort
DOHaD
Developmental Origins of Health and Disease
ECHO
Environmental Influences on Child Health Outcomes
ENRIECO
Environmental Health Risks in European Birth Cohorts
GST
glutathione S-transferase
HBC Study
Hamamatsu Birth Cohort for Mothers and Children
IUGR
intrauterine growth restriction
JECS
Japan Environment and Children’s Study
Ko-CHENS
Korean Children’s Environmental Health Study
LBW
low birth weight
LEAP
Long-term Exposure to Air Pollution and Pregnancy Outcomes
MoBa
Norwegian Mother and Child Cohort Study
MOCEH
Mothers and Children’s Environmental Health Study
NCD
non-communicable disease
NCS
National Children’s Study
PB
preterm birth
SGA
small-for-gestational-age
START
South Asian Birth Cohort Study
TBPS
Taiwan Birth Panel Study
TMM BirThree Cohort Study
Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study
Declarations
Ethical approval and consent to participate
Not applicable because of review article.
Consent for publication
Not applicable.
Availability of data and materials
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Funding
This study was supported by the Grant-in-Aid for Scientific Research from the Japanese Ministry of Health, Labour and Welfare (grant number: MH19189425 to Reiko Kishi); the Japan Society for the Promotion of Science; the Ministry of Education, Culture, Sports, Science and Technology (grant numbers: 20K10445 to Sumitaka Kobayashi; 17K01825 to Fumihiro Sata; 19H01071 and 21K19618 to Reiko Kishi); Japan Agency for Medical Research and Development (AMED) (grant number: 21gk0110039h0003 to Reiko Kishi and Fumihiro Sata); and Ministry of Internal Affairs and Communications (grant number: MI10001 to Reiko Kishi).
Authors’ contributions
SK conceived and wrote the paper. FS and RK contributed to the writing of the manuscript. All authors have reviewed the final version of the manuscript and approved its submission to this journal.
Acknowledgements
The authors would like to thank their colleagues (Professor Chihiro Miyashita, Drs. Sachiko Itoh, Hisanori Fukunaga, Keiko Yamazaki, Yu Ait Bamai, Takeshi Yamaguchi, Hideyuki Masuda, Naomi Tamura, Mariko Itoh, Nami Kawate; Ms. Rahel M. Ketema of the Center for Environmental and Health Sciences, Hokkaido University; and Professor Atsuko Ikeda-Araki and Dr. Kritika Poudel of the Faculty of Health Sciences, Hokkaido University) for valuable discussions. The authors appreciate the anonymous reviewers whose suggestions and comments have greatly improved this review paper.
References
- 1. Barker DJ. In utero programming of cardiovascular disease. Theriogenology. 2000;53(2):555–74.
- 2. Barker DJ, Osmond C. Infant mortality, childhood nutrition, and ischaemic heart disease in England and Wales. Lancet. 1986;1:1077–81.
- 3. Barker DJ. In utero programming of chronic disease. Clin Sci. 1998;95:115–28.
- 4. Garmendia ML, Corvalan C, Uauy R. Assessing the public health impact of developmental origins of health and disease (DOHaD) nutrition interventions. Ann Nutr Metab. 2014;64:226–30.
- 5. Selevan SG, Kimmel CA, Mendola P. Identifying critical windows of exposure for children’s health. Environ Health Perspect. 2000;108 Suppl 3(Suppl 3):451–5.
- 6. Lemasters GK, Perreault SD, Hales BF, Hatch M, Hirshfield AN, Hughes CL, et al. Workshop to identify critical windows of exposure for children’s health: reproductive health in children and adolescents work group summary. Environ Health Perspect. 2000;108 Suppl 3(Suppl 3):505–9.
- 7. Pryor JL, Hughes C, Foster W, Hales BF, Robaire B. Critical windows of exposure for children’s health: the reproductive system in animals and humans. Environ Health Perspect. 2000;108 Suppl 3(Suppl 3):491–503.
- 8. Pinkerton KE, Joad JP. The mammalian respiratory system and critical windows of exposure for children’s health. Environ Health Perspect. 2000;108 Suppl 3(Suppl 3):457–62.
- 9. Matthews TJ, MacDorman MF, Thoma ME. Infant mortality statistics from the 2013 period linked birth/infant death data set. Natl Vital Stat Rep. 2015;64(9):1–30.
- 10. Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJ. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis. JAMA. 2002;288(6):728–37.
- 11. de Kieviet JF, Piek JP, Aarnoudse-Moens CS, Oosterlaan J. Motor development in very preterm and very low-birth-weight children from birth to adolescence: a meta-analysis. JAMA. 2009;302(20):2235–42.
- 12. D’Onofrio BM, Class QA, Rickert ME, Larsson H, Långström N, Lichtenstein P. Preterm birth and mortality and morbidity: a population-based quasi-experimental study. JAMA Psychiatry. 2013;70(11):1231–40.
- 13. Clausson B, Lichtenstein P, Cnattingius S. Genetic influence on birthweight and gestational length determined by studies in offspring of twins. BJOG. 2000;107(3):375–81.
- 14. Grunnet L, Vielwerth S, Vaag A, Poulsen P. Birth weight is nongenetically associated with glucose intolerance in elderly twins, independent of adult obesity. J Intern Med. 2007;262(1):96–103.
- 15. Kistka ZAF, DeFranco EA, Ligthart L, Willemsen G, Plunkett J, Muglia LJ, et al. Heritability of parturition timing: an extended twin design analysis. Am J Obstet Gynecol. 2008;199(1):43.e1–5.
- 16. Lunde A, Klungsøyr Melve K, Gjessing HK, Skjaerven R, Irgens LM. Genetic and environmental influences on birth weight, birth length, head circumference, and gestational age by use of population-based parent-offspring data. Am J Epidemiol. 2007;165(7):734–41.
- 17. Plunkett J, Feitosa MF, Trusgnich M, Wangler MF, Palomar L, Kistka ZAF, et al. Mother’s genome or maternally-inherited genes acting in the fetus influence gestational age in familial preterm birth. Hum Hered. 2009;68(3):209–19.
- 18. Wu W, Witherspoon DJ, Fraser A, Clark EAS, Rogers A, Stoddard GJ, et al. The heritability of gestational age in a two-million member cohort: implications for spontaneous preterm birth. Hum Genet. 2015;134(7):803–8.
- 19. Arfsten DP, Silbergeld EK, Loffredo CA. Fetal ADH2*3, maternal alcohol consumption, and fetal growth. Int J Toxicol. 2004;23(1):47–54.
- 20. Barišić A, Kolak M, Peterlin A, Tul N, Gašparović Krpina M, Ostojić S, et al. DNMT3B rs1569686 and rs2424913 gene polymorphisms are associated with positive family history of preterm birth and smoking status. Croat Med J. 2020;61(1):8–17.
- 21. Bonou SG, Levallois P, Giguère Y, Rodriguez M, Bureau A. Prenatal exposure to drinking-water chlorination by-products, cytochrome P450 gene polymorphisms and small-for-gestational-age neonates. Reprod Toxicol. 2017;73:75–86.
- 22. Chand S, Mustafa MD, Banerjee BD, Guleria K. CYP17A1 gene polymorphisms and environmental exposure to organochlorine pesticides contribute to the risk of small for gestational age. Eur J Obstet Gynecol Reprod Biol. 2014;180:100–5.
- 23. Danileviciute A, Grazuleviciene R, Paulauskas A, Nadisauskiene R, Nieuwenhuijsen MJ. Low level maternal smoking and infant birthweight reduction: genetic contributions of GSTT1 and GSTM1 polymorphisms. BMC Pregnancy Childbirth. 2012;12:161.
- 24. Delpisheh A, Topping J, Reyad M, Tang A, Brabin BJ. Prenatal alcohol exposure, CYP17 gene polymorphisms and fetal growth restriction. Eur J Obstet Gynecol Reprod Biol. 2008;138(1):49–53.
- 25. Delpisheh A, Brabin L, Topping J, Reyad M, Tang AW, Brabin BJ. A case-control study of CYP1A1, GSTT1 and GSTM1 gene polymorphisms, pregnancy smoking and fetal growth restriction. Eur J Obstet Gynecol Reprod Biol. 2009;143(1):38–42.
- 26. Infante-Rivard C. Drinking water contaminants, gene polymorphisms, and fetal growth. Environ Health Perspect. 2004;112(11):1213–6.
- 27. Infante-Rivard C, Weinberg CR, Guiguet M. Xenobiotic-metabolizing genes and small-for-gestational-age births: interaction with maternal smoking. Epidemiology. 2006;17(1):38–46.
- 28. Infante-Rivard C. Caffeine intake and small-for-gestational-age birth: modifying effects of xenobiotic-metabolising genes and smoking. Paediatr Perinat Epidemiol. 2007;21(4):300–9.
- 29. Levallois P, Giguère Y, Nguile-Makao M, Rodriguez M, Campagna C, Tardif R, et al. Disinfection by-products exposure and intra-uterine growth restriction: Do genetic polymorphisms of CYP2E1or deletion of GSTM1 or GSTT1 modify the association? Environ Int. 2016;92–93:220–31.
- 30. Moreno-Banda G, Blanco-Muñoz J, Lacasaña M, Rothenberg SJ, Aguilar-Garduño C, Gamboa R, et al. Maternal exposure to floricultural work during pregnancy, PON1 Q192R polymorphisms and the risk of low birth weight. Sci Total Environ. 2009;407(21):5478–85.
- 31. Pereyra S, Bertoni B, Sapiro R. Interactions between environmental factors and maternal-fetal genetic variations: strategies to elucidate risks of preterm birth. Eur J Obstet Gynecol Reprod Biol. 2016;202:20–5.
- 32. Sharma E, Mustafa M, Pathak R, Guleria K, Ahmed RS, Vaid NB, et al. A case control study of gene environmental interaction in fetal growth restriction with special reference to organochlorine pesticides. Eur J Obstet Gynecol Reprod Biol. 2012;161(2):163–9.
- 33. Tsai HJ, Liu X, Mestan K, Yu Y, Zhang S, Fang Y, et al. Maternal cigarette smoking, metabolic gene polymorphisms, and preterm delivery: new insights on GxE interactions and pathogenic pathways. Hum Genet. 2008;123(4):359–69.
- 34. Tsai HJ, Hong X, Chen J, Liu X, Pearson C, Ortiz K, et al. Role of African ancestry and gene-environment interactions in predicting preterm birth. Obstet Gynecol. 2011;118(5):1081–9.
- 35. Von Linsingen R, Gelmini GF, Bicalho MDG, De Carvalho NS. MICA-129 A/G dimorphism, its relation to soluble mica plasma level and spontaneous preterm birth: a case-control study. J Reprod Immunol. 2018;129:9–14.
- 36. Wang X, Zuckerman B, Pearson C, Kaufman G, Chen C, Wang G, et al. Maternal cigarette smoking, metabolic gene polymorphism, and infant birth weight. JAMA. 2002;287(2):195–202.
- 37. Xie C, Jin R, Zhao Y, Lin L, Li L, Chen J, et al. Paraoxonase 2 gene polymorphisms and prenatal phthalates’ exposure in Chinese newborns. Environ Res. 2015;140:354–9.
- 38. Xie C, Wen X, Niu Z, Ding P, Liu T, He Y, et al. Combinations of CYP2A6*4 and glutathione S-transferases gene polymorphisms modify the association between maternal secondhand smoke exposure during pregnancy and small-for-gestational-age. Nicotine Tob Res. 2015;17(12):1421–7.
- 39. Zheng X, Feingold E, Ryckman KK, Shaffer JR, Boyd HA, Feenstra B, et al. Association of maternal CNVs in GSTT1/GSTT2 with smoking, preterm delivery, and low birth weight. Front Genet. 2013;4:196.
- 40. Aagaard-Tillery K, Spong CY, Thom E, Sibai B, Wendel G Jr, Wenstrom K, et al. Pharmacogenomics of maternal tobacco use: metabolic gene polymorphisms and risk of adverse pregnancy outcomes. Obstet Gynecol. 2010;115(3):568–77.
- 41. Ames J, Warner M, Mocarelli P, Brambilla P, Signorini S, Siracusa C, et al. AHR gene-dioxin interactions and birthweight in the Seveso second generation health study. Int J Epidemiol. 2018;47(6):1992–2004.
- 42. Cantonwine D, Hu H, Téllez-Rojo MM, Sánchez BN, Lamadrid-Figueroa H, Ettinger AS, et al. HFE gene variants modify the association between maternal lead burden and infant birthweight: a prospective birth cohort study in Mexico City, Mexico. Environ Health. 2010;9:43.
- 43. Duarte-Salles T, Mendez MA, Morales E, Bustamante M, Rodríguez-Vicente A, Kogevinas M, et al. Dietary benzo(a)pyrene and fetal growth: effect modification by vitamin C intake and glutathione S-transferase P1 polymorphism. Environ Int. 2012;45:1–8.
- 44. Harley KG, Huen K, Aguilar Schall R, Holland NT, Bradman A, Barr DB, et al. Association of organophosphate pesticide exposure and paraoxonase with birth outcome in Mexican-American women. PLoS One. 2011;6(8):e23923.
- 45. Hogervorst J, Vesper HW, Madhloum N, Gyselaers W, Nawrot T. Cord blood acrylamide levels and birth size, and interactions with genetic variants in acrylamide-metabolising genes. Environ Health. 2021;20(1):35.
- 46. Hong YC, Lee KH, Son BK, Ha EH, Moon HS, Ha M. Effects of the GSTM1 and GSTT1 polymorphisms on the relationship between maternal exposure to environmental tobacco smoke and neonatal birth weight. J Occup Environ Med. 2003;45(5):492–8.
- 47. Huang KH, Chou AK, Jeng SF, Ng S, Hsieh CJ, Chen MH, et al. The impacts of cord blood cotinine and glutathione-S-transferase gene polymorphisms on birth outcome. Pediatr Neonatol. 2017;58(4):362–9.
- 48. Hur J, Kim H, Ha EH, Park H, Ha M, Kim Y, et al. Birth weight of Korean infants is affected by the interaction of maternal iron intake and GSTM1 polymorphism. J Nutr. 2013;143(1):67–73.
- 49. Kobayashi S, Sata F, Sasaki S, Braimoh TS, Araki A, Miyashita C, et al. Combined effects of AHR, CYP1A1, and XRCC1 genotypes and prenatal maternal smoking on infant birth size: biomarker assessment in the Hokkaido study. Reprod Toxicol. 2016;65:295–306.
- 50. Kobayashi S, Sata F, Miyashita C, Sasaki S, Ban S, Araki A, et al. Dioxin-metabolizing genes in relation to effects of prenatal dioxin levels and reduced birth size: the Hokkaido study. Reprod Toxicol. 2017;67:111–6.
- 51. Kobayashi S, Sata F, Sasaki S, Braimoh TS, Araki A, Miyashita C, et al. Modification of adverse health effects of maternal active and passive smoking by genetic susceptibility: dose-dependent association of plasma cotinine with infant birth size among Japanese women-the Hokkaido study. Reprod Toxicol. 2017;74:94–103.
- 52. Kwon EJ, Shin JS, Kim BM, Shah-Kulkarni S, Park H, Kho Y, et al. Prenatal exposure to perfluorinated compounds affects birth weight through GSTM1 polymorphism. J Occup Environ Med. 2016;58(6):e198–205.
- 53. Lamichhane DK, Leem JH, Park CS, Ha M, Ha EH, Kim HC, et al. Associations between prenatal lead exposure and birth outcomes: modification by sex and GSTM1/GSTT1 polymorphism. Sci Total Environ. 2018;619–620:176–84.
- 54. Lee BE, Hong YC, Park H, Ha M, Koo BS, Chang N, et al. Interaction between GSTM1/GSTT1 polymorphism and blood mercury on birth weight. Environ Health Perspect. 2010;118(3):437–43.
- 55. Lee YM, Hong YC, Ha M, Kim Y, Park H, Kim HS, et al. Prenatal bisphenol-A exposure affects fetal length growth by maternal glutathione transferase polymorphisms, and neonatal exposure affects child volume growth by sex: from multiregional prospective birth cohort MOCEH study. Sci Total Environ. 2018;612:1433–41.
- 56. Leermakers ETM, Rob Taal H, Bakker R, Steegers EAP, Hofman A, Jaddoe VWV. A common genetic variant at 15q25 modifies the associations of maternal smoking during pregnancy with fetal growth: the generation R study. PLoS One. 2012;7(4):e34584.
- 57. Naidoo P, Naidoo RN, Ramkaran P, Muttoo S, Asharam K, Chuturgoon AA. Maternal miRNA-146a G/C rs2910164 variation, HIV/AIDS and nitrogen oxide pollution exposure collectively affects foetal growth. Hum Exp Toxicol. 2019;38(1):82–94.
- 58. Naidoo P, Naidoo RN, Ramkaran P, Chuturgoon AA. Effect of maternal HIV infection, BMI and NOx air pollution exposure on birth outcomes in South African pregnant women genotyped for the p53 Pro72Arg (rs1042522). Int J Immunogenet. 2020;47(5):414–29.
- 59. Nansook P, Naidoo RN, Muttoo S, Asharam K, Ramkaran P, Phulukdaree A, et al. IL-17A[G197G]-association between NOx and gestational age in a South African birth cohort. Int J Immunogenet. 2018;45(2):54–62.
- 60. Nukui T, Day RD, Sims CS, Ness RB, Romkes M. Maternal/newborn GSTT1 null genotype contributes to risk of preterm, low birthweight infants. Pharmacogenetics. 2004;14(9):569–76.
- 61. Sasaki S, Kondo T, Sata F, Saijo Y, Katoh S, Nakajima S, et al. Maternal smoking during pregnancy and genetic polymorphisms in the Ah receptor, CYP1A1 and GSTM1 affect infant birth size in Japanese subjects. Mol Hum Reprod. 2006;12(2):77–83.
- 62. Sasaki S, Sata F, Katoh S, Saijo Y, Nakajima S, Washino N, et al. Adverse birth outcomes associated with maternal smoking and polymorphisms in the N-nitrosamine-metabolizing enzyme genes NQO1 and CYP2E1. Am J Epidemiol. 2008;167(6):719–26.
- 63. Sasaki S, Limpar M, Sata F, Kobayashi S, Kishi R. Interaction between maternal caffeine intake during pregnancy and CYP1A2 C164A polymorphism affects infant birth size in the Hokkaido study. Pediatr Res. 2017;82(1):19–28.
- 64. Shin B, Kwon JA, Park EK, Kang S, Kim S, Park E, et al. Prenatal exposure to parabens affects birth outcomes through maternal glutathione S-transferase (GST) polymorphisms: from the mothers and kids environmental health (MAKE) study. Int J Environ Res Public Health. 2021;18(6):3012.
- 65. Slama R, Gräbsch C, Lepeule J, Siroux V, Cyrys J, Sausenthaler S, et al. Maternal fine particulate matter exposure, polymorphism in xenobiotic-metabolizing genes and offspring birth weight. Reprod Toxicol. 2010;30(4):600–12.
- 66. Suh YJ, Kim BM, Park BH, Park H, Kim YJ, Kim H, et al. Cytochrome P450IA1 polymorphisms along with PM(10) exposure contribute to the risk of birth weight reduction. Reprod Toxicol. 2007;24(3–4):281–8.
- 67. Thompson LM, Yousefi P, Peñaloza R, Balmes J, Holland N. Genetic modification of the effect of maternal household air pollution exposure on birth weight in Guatemalan newborns. Reprod Toxicol. 2014;50:19–26.
- 68. Wu T, Hu Y, Chen C, Yang F, Li Z, Fang Z, et al. Passive smoking, metabolic gene polymorphisms, and infant birth weight in a prospective cohort study of Chinese women. Am J Epidemiol. 2007;166(3):313–22.
- 69. Yang P, Cao WC, Zhou B, Zheng TZ, Deng YL, Luo Q, et al. Urinary biomarker of prenatal exposure to disinfection byproducts, maternal genetic polymorphisms in CYP2E1 and GSTZ1, and birth outcomes. Environ Sci Technol. 2019;53(20):12026–34.
- 70. Yila TA, Sasaki S, Miyashita C, Braimoh TS, Kashino I, Kobayashi S, et al. Effects of maternal 5,10-methylenetetrahydrofolate reductase C677T and A1298C polymorphisms and tobacco smoking on infant birth weight in a Japanese population. J Epidemiol. 2012;22(2):91–102.
- 71. Zhou B, Yang P, Gong YJ, Zeng Q, Lu WQ, Miao XP. Effect modification of CPY2E1 and GSTZ1 genetic polymorphisms on associations between prenatal disinfection by-products exposure and birth outcomes. Environ Pollut. 2018;243(Pt B):1126–1133.
- 72. Danileviciute A, Grazuleviciene R, Vencloviene J, Paulauskas A, Nieuwenhuijsen MJ. Exposure to drinking water trihalomethanes and their association with low birth weight and small for gestational age in genetically susceptible women. Int J Environ Res Public Health. 2012;9(12):4470–85.
- 73. Grazuleviciene R, Danileviciute A, Nadisauskiene R, Vencloviene J. Maternal smoking, GSTM1 and GSTT1 polymorphism and susceptibility to adverse pregnancy outcomes. Int J Environ Res Public Health. 2009;6(3):1282–97.
- 74. Grazuleviciene R, Nieuwenhuijsen MJ, Danileviciute A, Nadisauskiene R, Buinauskiene J. Gene-environment interaction: maternal smoking and contribution of GSTT1 and GSTM1 polymorphisms to infant birth-weight reduction in a Kaunas cohort study. J Epidemiol Community Health. 2010;64(7):648.
- 75. Hao Y, Yan L, Pang Y, Yan H, Zhang L, Liu J, et al. Maternal serum level of manganese, single nucleotide polymorphisms, and risk of spontaneous preterm birth: a nested case-control study in China. Environ Pollut. 2020;262:114187.
- 76. Kogevinas M, Bustamante M, Gracia-Lavedán E, Ballester F, Cordier S, Costet N, et al. Drinking water disinfection by-products, genetic polymorphisms, and birth outcomes in a European mother-child cohort study. Epidemiology. 2016;27(6):903–11.
- 77. Zhao N, Wu W, Feng Y, Yang F, Han T, Guo M, et al. Polymorphisms in oxidative stress, metabolic detoxification, and immune function genes, maternal exposure to ambient air pollution, and risk of preterm birth in Taiyuan, China. Environ Res. 2021;194:110659.
- 78. Gloria-Bottini F, Magrini A, Cozzoli E, Bergamaschi A, Bottini E. ADA genetic polymorphism and the effect of smoking on neonatal bilirubinemia and developmental parameters. Early Hum Dev. 2008;84(11):739–43.
- 79. Gloria-Bottini F, Bottini E. Smoking and the correlation between birth weight and placental weight. Evidence of interaction with maternal haptoglobin phenotype. Eur J Obstet Gynecol Reprod Biol. 2015;185:136–9.
- 80. Karahalil B, Emerce E, Kocabaş NA, Akkaş E. Associations between GSTM1 and OGG1 Ser326Cys polymorphisms and smoking on chromosomal damage and birth growth in mothers. Mol Biol Rep. 2011;38(5):2911–8.
- 81. Kordas K, Ettinger AS, Lamadrid-Figueroa H, Tellez-Rojo MM, Hérnandez-Avila M, Hu H, et al. Methylenetetrahydrofolate reductase (MTHFR) C677T, A1298C and G1793A genotypes, and the relationship between maternal folate intake, tibia lead and infant size at birth. Br J Nutr. 2009;102(6):907–14.
- 82. Price TS, Grosser T, Plomin R, Jaffee SR. Fetal genotype for the xenobiotic metabolizing enzyme NQO1 influences intrauterine growth among infants whose mothers smoked during pregnancy. Child Dev. 2010;81(1):101–14.
- 83. Taylor GM, Alexander FE, D’Souza SW. Interactions between fetal HLA-DQ alleles and maternal smoking influence birthweight. Paediatr Perinat Epidemiol. 2006;20(5):438–48.
- 84. Brand JS, Gaillard R, West J, McEachan RRC, Wright J, Voerman E, et al. Associations of maternal quitting, reducing, and continuing smoking during pregnancy with longitudinal fetal growth: Findings from Mendelian randomization and parental negative control studies. PLoS Med. 2019;16(11):e1002972.
- 85. Marsh JA, Pennell CE, Warrington NM, Mook-Kanamori D, Briollais L, Lye SJ, et al. Fat mass and obesity-associated obesity-risk genotype is associated with lower foetal growth: an effect that is reversed in the offspring of smoking mothers. J Dev Orig Health Dis. 2012;3(1):10–20.
- 86. Tyrrell J, Huikari V, Christie JT, Cavadino A, Bakker R, Brion MJ, et al. Genetic variation in the 15q25 nicotinic acetylcholine receptor gene cluster (CHRNA5-CHRNA3-CHRNB4) interacts with maternal self-reported smoking status during pregnancy to influence birth weight. Hum Mol Genet. 2012;21(24):5344–58.
- 87. Huang H, Clancy KBH, Burhance C, Zhu Y, Madrigal L. Women who deliver twins are more likely to smoke and have high frequencies of specific SNPs: results from a sample of African-American women who delivered preterm, low birth weight babies. Am J Hum Biol. 2015;27(5):605–12.
- 88. Kobayashi S, Sata F, Sasaki S, Ban S, Miyashita C, Okada E, et al. Genetic association of aromatic hydrocarbon receptor (AHR) and cytochrome P450, family 1, subfamily A, polypeptide 1 (CYP1A1) polymorphisms with dioxin blood concentrations among pregnant Japanese women. Toxicol Lett. 2013;219(3):269–78.
- 89. Kobayashi S, Sata F, Miyashita C, Miura R, Azumi K, Kobayashi S, et al. Gender-specific association of exposure to non-dioxin-like polychlorinated biphenyls during pregnancy with methylation levels of H19 and long interspersed nuclear element-1 in cord blood in the Hokkaido study. Toxicology. 2017;390:135–45.
- 90. Kobayashi S, Sata F, Hanaoka T, Braimoh TS, Ito K, Tamura N, et al. Association between maternal passive smoking and increased risk of delivering small-for-gestational-age infants at full-term using plasma cotinine levels from The Hokkaido Study: a prospective birth cohort. BMJ Open. 2019a;9(2):e023200.
- 91. Kobayashi S, Sata F, Goudarzi H, Araki A, Miyashita C, Sasaki S, et al. Associations among perfluorooctanesulfonic/perfluorooctanoic acid levels, nuclear receptor gene polymorphisms, and lipid levels in pregnant women in the Hokkaido study. Sci Rep. 2021;11(1):9994.
- 92. Kishi R, Araki A, Minatoya M, Hanaoka T, Miyashita C, Itoh S, et al. The Hokkaido birth cohort study on environment and children’s health: cohort profile-updated 2017. Environ Health Prev Med. 2017;22(1):46.
- 93. Kishi R, Ikeda-Araki A, Miyashita C, Itoh S, Kobayashi S, Ait Bamai Y, et al. Hokkaido birth cohort study on environment and children’s health: cohort profile 2021. Environ Health Prev Med. 2021;26(1):59.
- 94. Nishimura Y, Moriya K, Kobayashi S, Araki A, Sata F, Mitsui T, et al. Association between ESR1 polymorphisms and second to fourth digit ratio in school-aged children in the Hokkaido study. Steroids. 2019;141:55–62.
- 95. Nishimura Y, Moriya K, Kobayashi S, Araki A, Sata F, Mitsui T, et al. Association of exposure to prenatal phthalate esters and bisphenol A and polymorphisms in the ESR1 gene with the second to fourth digit ratio in school-aged children: data from the Hokkaido study. Steroids. 2020;159:108637.
- 96. Braimoh TS, Kobayashi S, Sata F, Sasaki S, Goudarzi H, Yila TA, et al. Association of prenatal passive smoking and metabolic gene polymorphisms with child growth from birth to 3years of age in the Hokkaido birth cohort study on environment and children’s health. Sci Total Environ. 2017;605–606:995–1002.
- 97. Kobayashi S, Sata F, Ikeda-Araki A, Miyashita C, Goudarzi H, Iwasaki Y, et al. Associations among maternal perfluoroalkyl substance levels, fetal sex-hormone enzymatic gene polymorphisms, and fetal sex hormone levels in the Hokkaido study. Reprod Toxicol. 2021;105:221–31.
- 98. Olsen J, Melbye M, Olsen SF, Sørensen TI, Aaby P, Andersen AM, et al. The Danish National Birth Cohort--its background, structure and aim. Scand J Public Health. 2001;29(4):300–7.
- 99. Nybo Andersen AM, Olsen J. The Danish National Birth Cohort: selected scientific contributions within perinatal epidemiology and future perspectives. Scand J Public Health. 2011;39(7 Suppl):115–20.
- 100. Magnus P, Irgens LM, Haug K, Nystad W, Skjaerven R, Stoltenberg C, et al. Cohort profile: the Norwegian Mother and Child Cohort Study (MoBa). Int J Epidemiol. 2006;35(5):1146–50.
- 101. Magnus P, Birke C, Vejrup K, Haugan A, Alsaker E, Daltveit AK, et al. Cohort Profile Update: The Norwegian Mother and Child Cohort Study (MoBa). Int J Epidemiol. 2016;45(2):382–8.
- 102. Ghisari M, Long M, Røge DM, Olsen J, Bonefeld-Jørgensen EC. Polymorphism in xenobiotic and estrogen metabolizing genes, exposure to perfluorinated compounds and subsequent breast cancer risk: A nested case-control study in the Danish National Birth Cohort. Environ Res. 2017;154:325–33.
- 103. Myking S, Myhre R, Gjessing HK, Morken NH, Sengpiel V, Williams SM, et al. Candidate gene analysis of spontaneous preterm delivery: new insights from re-analysis of a case-control study using case-parent triads and control-mother dyads. BMC Med Genet. 2011;12:174.
- 104. Vrijheid M, Casas M, Bergström A, Carmichael A, Cordier S, Eggesbø M, et al. European birth cohorts for environmental health research. Environ Health Perspect. 2012;120(1):29–37.
- 105. Gehring U, Casas M, Brunekreef B, Bergström A, Bonde JP, Botton J, et al. Environmental exposure assessment in European birth cohorts: results from the ENRIECO project. Environ Health. 2013;12:8.
- 106. Spadea T, Pacelli B, Ranzi A, Galassi C, Rusciani R, Demaria M, et al. An Italian network of population-based birth cohorts to evaluate social and environmental risk factors on pregnancy outcomes: the LEAP study. Int J Environ Res Public Health. 2020;17(10):3614.
- 107. Jaddoe VWV, Felix JF, Andersen AMN, Charles MA, Chatzi L, Corpeleijn E, et al. The LifeCycle Project-EU Child Cohort Network: a federated analysis infrastructure and harmonized data of more than 250,000 children and parents. Eur J Epidemiol. 2020;35(7):709–24.
- 108. Landrigan PJ, Trasande L, Thorpe LE, Gwynn C, Lioy PJ, D’Alton ME, et al. The National Children’s Study: a 21-year prospective study of 100,000 American children. Pediatrics. 2006;118(5):2173–86.
- 109. Kimmel CA, Collman GW, Fields N, Eskenazi B. Lessons learned for the National Children’s Study from the National Institute of Environmental Health Sciences/U.S. Environmental Protection Agency Centers for Children’s Environmental Health and Disease Prevention Research. Environ Health Perspect. 2005;113(10):1414–8.
- 110. Landrigan PJ, Baker DB. The National Children’s Study—end or new beginning? N Engl J Med. 2015;372(16):1486–7.
- 111. Anand SS, Vasudevan A, Gupta M, Morrison K, Kurpad A, Teo KK, et al. Rationale and design of South Asian birth cohort (START): a Canada-India collaborative study. BMC Public Health. 2013;13:79.
- 112. Johnson CC, Chandran A, Havstad S, Li X, McEvoy CT, Ownby DR, et al. US childhood asthma incidence rate patterns from the ECHO consortium to identify high-risk groups for primary prevention. JAMA Pediatr. 2021;e210667.
- 113. Gern JE, Jackson DJ, Lemanske RF Jr, Seroogy CM, Tachinardi U, Craven M, et al. The children’s respiratory and environmental workgroup (CREW) birth cohort consortium: design, methods, and study population. Respir Res. 2019;20(1):115.
- 114. Ober C, McKennan CG, Magnaye KM, Altman MC, Washington C 3rd, Stanhope C, et al. Expression quantitative trait locus fine mapping of the 17q12-21 asthma locus in African American children: a genetic association and gene expression study. Lancet Respir Med. 2020;8(5):482–92.
- 115. Zijlmans W, Wickliffe J, Hindori-Mohangoo A, MacDonald-Ottevanger S, Ouboter P, Landburg G, et al. Caribbean consortium for research in environmental and occupational health (CCREOH) cohort study: influences of complex environmental exposures on maternal and child health in Suriname. BMJ Open. 2020;10(9):e034702.
- 116. Kawamoto T, Nitta H, Murata K, Toda E, Tsukamoto N, Hasegawa M, et al. Rationale and study design of the Japan environment and children’s study (JECS). BMC Public Health. 2014;14:25.
- 117. Kobayashi S, Sata F, Murata K, Saijo Y, Araki A, Miyashita C, et al. Dose-dependent associations between prenatal caffeine consumption and small for gestational age, preterm birth, and reduced birthweight in the Japan environment and children’s study. Paediatr Perinat Epidemiol. 2019;33(3):185–94.
- 118. Kobayashi S, Kishi R, Saijo Y, Ito Y, Oba K, Araki A, et al. Association of blood mercury levels during pregnancy with infant birth size by blood selenium levels in the Japan environment and children’s study: a prospective birth cohort. Environ Int. 2019;125:418–29.
- 119. Jeong KS, Kim S, Kim WJ, Kim HC, Bae J, Hong YC, et al. Cohort profile: beyond birth cohort study - the Korean children’s environmental health study (Ko-CHENS). Environ Res. 2019;172:358–66.
- 120. Kishi R, Zhang JJ, Ha EH, Chen PC, Tian Y, Xia Y, et al. Birth cohort consortium of Asia: current and future perspectives. Epidemiology. 2017;28(Suppl 1):S19–34.
- 121. Hsieh CJ, Hsieh WS, Su YN, Liao HF, Jeng SF, Taso FM, et al. The Taiwan birth panel study: a prospective cohort study for environmentally-related child health. BMC Res Notes. 2011;4:291.
- 122. Kim BM, Ha M, Park HS, Lee BE, Kim YJ, Hong YC, et al. The mothers and children’s environmental health (MOCEH) study. Eur J Epidemiol. 2009;24(9):573–83.
- 123. Hsieh CJ, Liao HF, Wu KY, Hsieh WS, Su YN, Jeng SF, et al. CYP1A1 Ile462Val and GSTT1 modify the effect of cord blood cotinine on neurodevelopment at 2 years of age. Neurotoxicology. 2008;29(5):839–45.
- 124. Koh TK, Park H, Hong YC, Ha M, Kim Y, Lee BE, et al. Association between prenatal polycyclic aromatic hydrocarbons and infantile allergic diseases modified by maternal glutathione S-transferase polymorphisms: results from the MOCEH birth cohort. Ann Occup Environ Med. 2021;33:e12.
- 125. Kuriyama S, Metoki H, Kikuya M, Obara T, Ishikuro M, Yamanaka C, et al. Cohort profile: Tohoku medical megabank project birth and three-generation cohort study (TMM BirThree Cohort Study): rationale, progress and perspective. Int J Epidemiol. 2020;49(1):18–19m.
- 126. Sakurai K, Miyaso H, Eguchi A, Matsuno Y, Yamamoto M, Todaka E, et al. Chiba study of mother and children’s health (C-MACH): cohort study with omics analyses. BMJ Open. 2016;6(1):e010531.
- 127. Morisaki N, Fujiwara T, Horikawa R. The impact of parental personality on birth outcomes: a prospective cohort study. PLoS One. 2016;11(6):e0157080.
- 128. Takagai S, Tsuchiya KJ, Itoh H, Kanayama N, Mori N, Takei N, et al. Cohort profile: Hamamatsu birth cohort for mothers and children (HBC Study). Int J Epidemiol. 2016;45(2):333–42.
- 129. Metoki H, Ohkubo T, Watanabe Y, Nishimura M, Sato Y, Kawaguchi M, et al. Seasonal trends of blood pressure during pregnancy in Japan: the babies and their parents’ longitudinal observation in Suzuki memorial hospital in intrauterine period study. J Hypertens. 2008;26(12):2406–13.
- 130. Yasuda J, Kinoshita K, Katsuoka F, Danjoh I, Sakurai-Yageta M, Motoike IN, et al. Genome analyses for the Tohoku Medical Megabank Project towards establishment of personalized healthcare. J Biochem. 2019;165(2):139–58.
- 131. Miyaso H, Sakurai K, Takase S, Eguchi A, Watanabe M, Fukuoka H, et al. The methylation levels of the H19 differentially methylated region in human umbilical cords reflect newborn parameters and changes by maternal environmental factors during early pregnancy. Environ Res. 2017;157:1–8.
- 132. Beckmann JS, Lew D. Reconciling evidence-based medicine and precision medicine in the era of big data: challenges and opportunities. Genome Med. 2016;8(1):134.
- 133. Carrasco-Ramiro F, Peiró-Pastor R, Aguado B. Human genomics projects and precision medicine. Gene Ther. 2017;24(9):551–61.
- 134. Ramaswami R, Bayer R, Galea S. Precision medicine from a public health perspective. Annu Rev Public Health. 2018;39:153–68.
- 135. Kee F, Taylor-Robinson D. Scientific challenges for precision public health. J Epidemiol Community Health. 2020;74(4):311–4.
- 136. Khoury MJ, Iademarco MF, Riley WT. Precision public health for the era of precision medicine. Am J Prev Med. 2016;50(3):398–401.
- 137. Khoury MJ, Bowen MS, Clyne M, Dotson WD, Gwinn ML, Green RF, et al. From public health genomics to precision public health: a 20-year journey. Genet Med. 2018;20(6):574–82.
- 138. Imura H. Life course health care and preemptive approach to non-communicable diseases. Proc Jpn Acad Ser B Phys Biol Sci. 2013;89(10):462–73.
- 139. Itoh H, Hayashi K, Miyashita K. Pre-emptive medicine for hypertension and its prospects. Hypertens Res. 2019;42(3):301–5.
