Abstract
Medical research spurred by radiation exposure is a critically important theme for modern society. Accordingly, studies of this contemporary problem should be based on a perspective that is focused on that origin, medical investigations into the effects of radiation exposure on survivors of the atomic bombs. Therefore, we organized and evaluated survey programs and research of atomic bomb survivors that have been conducted by ABCC (Atomic Bomb Casualty Commission) –RERF (Radiation Effects Research Foundation) and RIRBM (Research Institute for Radiation Biology and Medicine) between 1949 and 1975.
ABCC established a set of carefully defined cohorts and launched an integrated research program based on three phases of pure research. That work has formed the foundation for the research that the RERF is engaged in today. And among surveys and studies worldwide that have generated fundamental data on radiation protection standards, the findings of ABCC-RERF surveys and studies have provided important information. It has thus provided various international research organizations (WHO (World Health Organization), ICRP (International Commission on Radiological Protection), UNSCEAR (United Nations Scientific Committee on the Effects of Atomic Radiation), etc.) with important information and indicators.
RIRBM has pursued studies and surveys that are distinct from the undertakings led by ABCC-RERF. RIRBM was able to do something that ABCC-RERF would have found difficult to implement: namely, flexibly launching projects on themes that directly met the needs of the local society at the time.
Atomic bomb survivors’ medical data continue to grow, from the bombing to the present, and to the future. Data sharing, joint research, and collaboration by research institutions in this field will be effective ways to foster rationally coordinated surveys and studies.
INTRODUCTION
Medical studies of atomic bomb survivors in Japan began immediately after the atomic bombs were dropped in August 1945. These studies were led by the Japanese military, which generally recognized on August 7, 1945 that the “new bomb” dropped was an atomic device6), and that the symptoms experienced by its survivors were caused by exposure to radiation. However, facing imminent defeat at this chaotic moment, Japan was at that time not able to implement a large-scale, systematic survey backed by adequate levels of consideration and preparation. Consequently, comprehensive Japanese research on this matter had to wait for a special committee for atomic bomb disaster investigations, which was inaugurated in September 1945 and engaged in research until March 1948 under the aegis of the Academic Research Council of Japan (the predecessor to the Science Council of Japan, or SCJ). The findings of the committee were published in the Investigation Report on Atomic Bomb Disaster by the Japan Society for the Promotion of Science (JSPS) in 1953, that is, after the Occupation had ended and Japan had regained its independence8).
The United States (U.S.) was in charge of the key studies conducted by the victorious nations in the war. Although these investigations did not begin until after the formal signing of Japan’s surrender in September 1945, as the nation that dropped the atomic bombs, the U.S. side knew the nature of the bomb and was prepared to deal with the harmful effects of exposure to radiation from these blasts. The following three studies are well known.
1. The Manhattan District Atomic Bomb Investigating Group: The related survey began in September 1945. The preliminary report was released in December 1945 and the final report was released in April 19464).
2. The US Strategic Bombing Survey: This survey was conducted from October to December 1945. The preliminary report was released in December 1945 and the final report was released on June 30, 194610).
3. The Armed Forces Joint Commission for Investigating Effects of the Atomic Bomb in Japan: This project was organized by the GHQ Army Medical Association, the Manhattan District Atomic Bomb Investigating Group, and the Japanese Research Group (represented by Dr. Masao Tsuzuki) on September 22, 1945, with the survey being completed in December 1945. The report was published (but not disclosed) in September 1946 and it was later publicly released by the American Atomic Energy Commission on April 19, 19519).
These early surveys are believed to have provided suggestions for the direction of subsequent investigations and research by the U.S. In other words, they alerted the U.S. regarding the importance of the biological effects of radiation exposure on the human body and the delayed onset of those effects, and hence, the extreme importance of sustained, long-term studies and research. This was the impetus behind the creation of the Atomic Bomb Casualty Commission (ABCC), the predecessor to the Radiation Effects Research Foundation (RERF)7).
Because the effects of radiation on the human body are not marked by a set of specific symptoms, it is difficult to determine whether those effects are caused by radiation, and it is considered almost impossible to identify their underlying causes, even today. This view heightened the necessity for epidemiological surveys designed to track groups of survivors of radiation exposure over extended periods and observe whether the characteristic effects would become widely manifest3,7). The ABCC and RERF were largely responsible for such surveys over the more-than-60 years immediately following the end of World War II to the present day. Their epidemiological studies, research, and data are now vital resources for investigators concerned with contemporary issues in radiation exposure. Moreover, as research institutions, the ABCC and its successor, the RERF, have collaborated with Japan and Japanese investigators and have not been engaged solely under the direction of the U.S. Nonetheless, during the period that the ABCC was active (1947 to 1975), it was naturally under the strong influence of the U.S. due to its historical background and organizational structure.
In that respect, Japan lagged behind in studies on radiation effects, but not because of any inertia or indolence on the part of the Japanese. In the postwar years, Japan as a nation was caught in a turbulent period of social and political upheaval stemming from its wartime defeat, and Hiroshima and Nagasaki, the two cities destroyed by the atomic bombs, were only in the early stages of efforts to rebuild their devastated cities. These factors largely prevented Japan from moving forward even with important medical research on this subject. Moreover, prior to the signing of the Treaty of Peace with Japan in San Francisco in 1952, Japan, as an occupied nation integrated into the fabric of the Cold War, was not able to fully take the initiative in these research undertakings or in the compilation of relevant data. Nonetheless, in the sites affected by the atomic bombs, it did launch studies and research that also addressed the problems associated with medical care for the survivors. To that end, the Atomic Bomb Disease Institute at Nagasaki University and the Nagasaki Atomic Bomb Casualty Council were established in Nagasaki, while the Hiroshima Atomic Bomb Casualty Council was set up in Hiroshima. Furthermore, in 1961, the Research Institute for Radiation Biology and Medicine (RIRBM) was established at Hiroshima University. However, in those early days RIRBM did not have access to sufficient funding, nor did it have a well-developed research environment or a comprehensive research program with a long-term outlook, and thus had to look for research strategies different from those pursued by the preexistent ABCC.
In this study, we analyzed the survey programs and studies on atomic bomb survivors in Hiroshima with consideration for the conditions faced by the ABCC and the RIRBM at the time and, on that basis, explored the implications for future research on the human health effects of radiation exposure.
MATERIALS AND METHODS
We organized and evaluated surveys of atomic bomb survivors that have been conducted by the ABCC-RERF and the RIRBM. Both institutions are still in operation and continue to produce extensive research to this day. Therefore, this paper first summarizes the overall programs conducted to date at each institution and then, primarily, examines the important surveys and research on atomic bomb survivors that they performed during their first 30 years of operation, that is, up to 1975, when the ABCC was reorganized by the RERF.
The current RERF has inherited the ABCC’s research (especially research since 1955). However, the reorganization of the ABCC into the RERF in 1975 was a major change for the laboratory. The related expenses, according to the RERF website, have been described as follows:
“Funds for RERF’s operation continue to be provided by both governments, by Japan through the Ministry of Health, Labour and Welfare, and by the U.S. through the Department of Energy.”
In addition, of course, there have been changes in operational management and research activities. Therefore, in this study, we examined the ABCC era (especially 1955–1975), which we regard as the first phase. The period after 1975 (the second phase) will be future work.
A. ABCC
In terms of the ABCC, we primarily organized and evaluated the Technical Reports (represented by “TR” in the report numbering) and Annual Reports published by this institution. We evaluated summaries of the Technical Reports issued between 1959 and 1975. A total of 777 Technical Reports were examined, of which 632 were research reports. In addition, we summarized the research topics on atomic bomb survivors conducted by this research institute and its implementation period.
B. RIRBM
Our analysis of the studies by the RIRBM was based on Annual Reports and other documentation published by that institution. The RIRBM was established in 1961 and its predecessor was the Atomic Radiation Basic Medical Research Facility, which was affiliated to the Hiroshima University’s School of Medicine. Our analysis includes the inaugural issue of the RIRBM because the inaugural Annual Report was issued in 1960 when the facility was still in operation11). Specifically, for the annual report from the first issue to the 16th issue (1961–1975), we confirmed 370 research articles and analyzed 165 articles among them.
RESULTS
A. Survey program
A-1. ABCC-RERF
(1) ABCC-RERF Cohorts
The following is a brief history of the formation of the fixed cohorts that the ABCC-RERF utilized as a platform for its research. The ABCC compiled its Master File based on the following surveys:
1. (Hiroshima population samples) Hiroshima atomic bomb survivor survey, 1946 (Survey by Hiroshima City, August 10, 1945–)
2. (Hiroshima population samples) Japan-U.S. joint survey team records (September to December 1945)
3. (Nagasaki population samples) survey samples used by Nagasaki University’s Prof. Raisuke Shirabe (November 1945)
4. (Hiroshima population samples) 1950 national census and incidental surveys (October 1950)
5. Additionally, data collected by Neel et al. from genetic surveys started in 1948.
Using the Master File, the fixed cohorts referred to as Master Samples were established from 1956 to 1961. The cohort members were selected on the basis of the following conditions:
1. Be residents of Hiroshima or Nagasaki.
2. Have Japanese nationality.
3. Have legal domicile in Hiroshima, Nagasaki, or certain surrounding districts.
4. Be a confirmed atomic bomb survivor or non-exposed person.
This is also the foundation for research led by the RERF currently.
(2) Summary of the Main ABCC-RERF Survey Programs
We summarized the main programs of the ABCC-RERF research (Figure 1). The ABCC implemented studies in line with the recommendations of the 1955 Francis Report, and the RERF has continued to conduct the main Life Span Study (LSS) and Adult Health Study (AHS) up to the present day, amassing over 60 years of data in the process.
From the outset, the ABCC was also highly interested in genetic effects and the effects on the children of atomic bomb survivors. As shown in Figure 1, the RERF has inherited these interests of the ABCC. Furthermore, it has expanded the number of projects and continued with studies that reflect trends in the diversification of research.
The ABCC surveys and research studies published prior to 1955 were not implemented under a system of the kind that the RERF utilizes today. For example, early-period ABCC researchers Woodbury and Kastenbaum cited problems with the reliability of collected data. Woodbury conducted comparative studies of mortality rates for atomic bomb survivors and non-exposed cohorts from 1950 to 1954; the findings of that research were deemed important because they suggested that the variance in mortality rates was attributable to differences in the radiological dosage of exposure. Objections to this conclusion, however, arose because the study itself was not based on comparisons of fixed cohorts5). In effect, interest in the epidemiological questions grew even as important points were confirmed regarding the health effects from exposure to radiation. Given these circumstances, in 1955 the ABCC enacted sweeping changes to its research framework. This was documented in the Report of an ad hoc committee for appraisal of the ABCC Program [TR33-59]1), which was referred to as the Francis Report because Thomas Francis Jr. was the Committee’s Chairperson. The report contained the following four key recommendations, as cited by Dr. Masayoshi Matsuzaka5) and noted in the provisional research plan [TR9-60]2) for the ABCC-JNIH Adult Health Study.
1. Formulate a firm plan (unified study plan) for core, long-term research programs.
(The unified study plan consisted mainly of the (a) Life Span Study (LSS; ST-100), (b) Adult Health Study (AHS; ME-200), and (c) Pathological Study.
2. Define fixed samples (fixed cohorts) and treat them as unchanging sample populations for long-term study.
3. Treat research samples (fixed cohorts) as a subset of the total master sample.
4. Build a core research plan that consists of the following three stages:
4-1. Statistical mortality survey
4-2. Clinical studies complemented by morbidity studies based on field surveys
4-3. Pathological studies
To summarize, in 1955, the ABCC essentially adopted the concept of fixed cohorts for continuous, long-term monitoring. Furthermore, that platform has been inherited and sustained by its successor, the RERF.
A-2. RIRBM
(1) The Identification of Atomic Bomb Survivor Populations by the RIRBM
Unlike the ABCC-RERF, the RIRBM did not pursue research based on the use of fixed cohorts. Instead, in the process of conducting numerous studies and surveys and assisting Hiroshima City and Hiroshima Prefecture with their public surveys of atomic bomb survivors, it compiled its own databases on atomic bomb survivors, one of which was the Database of Atomic Bomb Survivors in Hiroshima Prefecture (ABS). This database was created with the cooperation of Hiroshima City and Hiroshima Prefecture and involved reviewing and comparing the findings as well as survey questionnaire forms from atomic bomb survivor surveys conducted in the 1960s and 1970s. In 1969, Hiroshima City launched a program of demographic surveys of atomic bomb survivors, and that program is still ongoing. The RIRBM has assisted in conducting those surveys and organizing the data. The accomplishments of this program are reflected in its ABS. Unlike the approach taken with cohorts, these data resources have not been narrowed down to specific districts within Hiroshima City but are the result of an effort to identify the conditions for atomic bomb survivors in the wider geographical area.
RIRBM studies and surveys have been conducted under the cooperation of investigators specialized in many fields. One early and valuable example is the “ground zero reconstruction” survey, which was launched in 1968. This was an RIRBM-led survey aimed primarily at facilitating sociological and social medicine-related research and also supported by Hiroshima City and Hiroshima Prefecture. It was limited in geographical scope to a radius of 0.5–2.0 kilometers from the blast center. Utilizing the data and findings from this survey, Hiroshima City later launched its earlier-noted program of demographic surveys of atomic bomb survivors. In 1972, the RIRBM expanded on that Hiroshima program with an internal project for a comprehensive medical study of atomic bomb survivors living near the blast center. This was a highly specialized and valuable study of atomic bomb survivors living within a half-a-kilometer radius from the blast center. These surveys and studies are illustrated with the flow chart in Figure 2.

The above information highlights the following features regarding the RIRBM’s data on atomic bomb survivors, including its ABS:
1. Surveys have been implemented with close cooperation sought from Hiroshima City, Hiroshima Prefecture, and other local communities, generating data that provide the basis for medical studies.
2. The RIRBM database is based on unique studies either initiated by the RIRBM or involving the organization in some way.
3. Knowledge has also been obtained through collaboration in different areas of research, including the fields of social medicine, sociology, and medicine.
However, there have been concerns about the rigor of data reviews and the qualitative uniformity of the data. That said, it would be hasty to conclude on those grounds that the data lack scientific value. Although it is important to develop an understanding of the overall picture, one must not overlook the minor, unique cases and the database offers such cases.
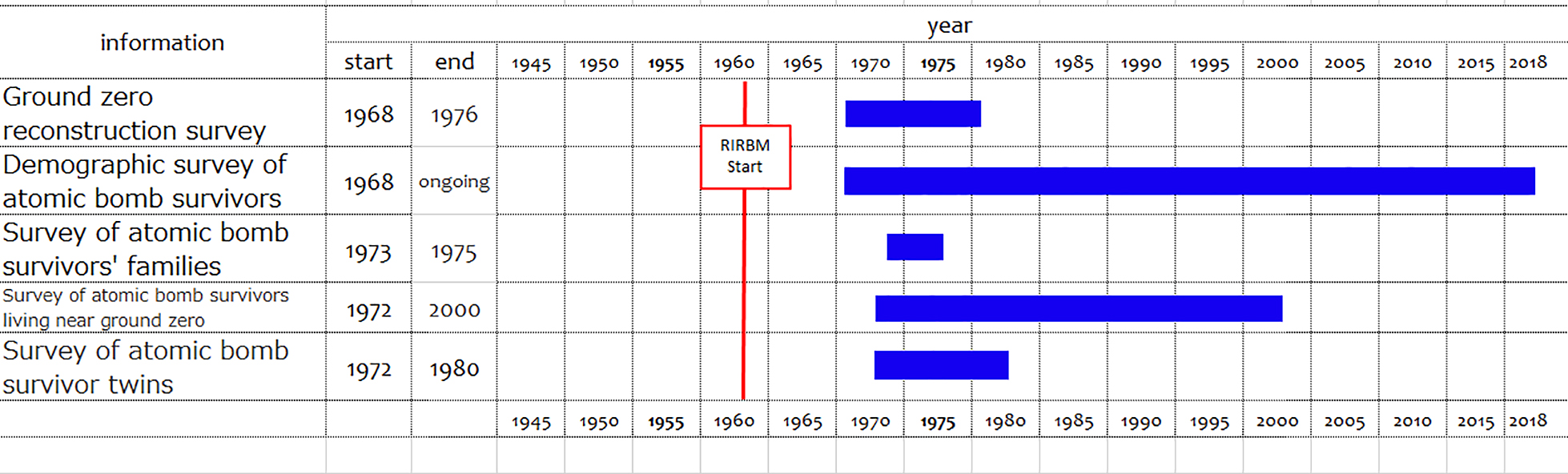
(2) An Overview of the Main RIRBM Surveys
Since its founding, the RIRBM has launched its studies and surveys of atomic bomb survivors in collaboration with Hiroshima University’s School of Medicine. However, as Figure 3 shows, the surveys for the systematic collection of data on atomic bomb survivors were implemented around 1970. Because the RIRBM and the ABCC frequently engaged in researcher exchange, RIRBM researchers are certain to have had opportunities for firsthand exposure to ABCC studies based on fixed cohorts. From that perspective, it is noteworthy that the RIRBM chose different strategies for atomic bomb survivor information and research framework development that differed from the approaches taken by the ABCC.
B. Research
B-1. ABCC-RERF: Technical Reports
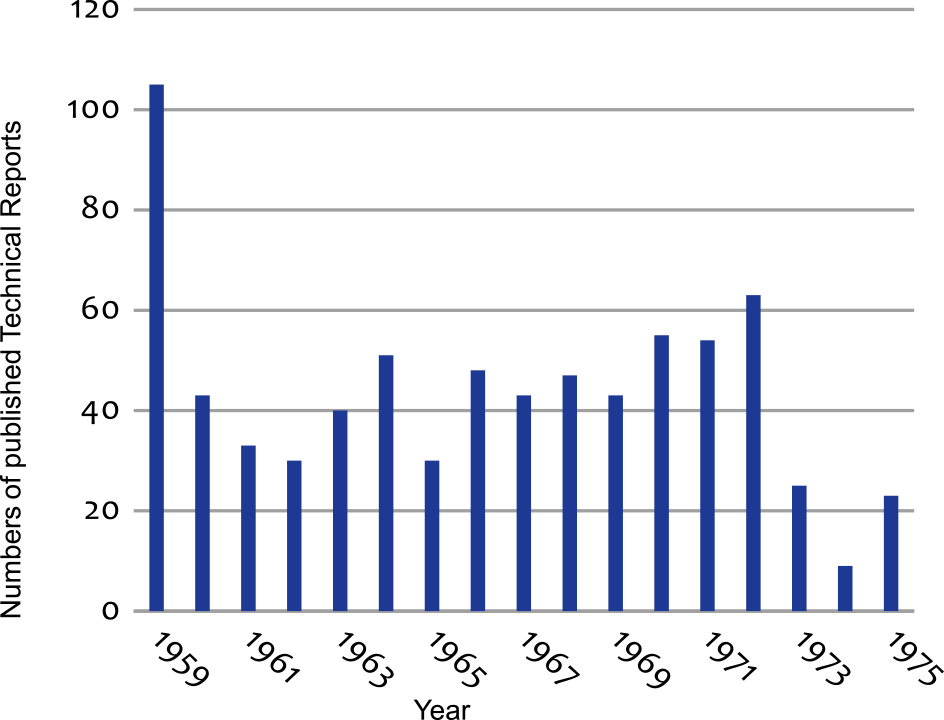
Figure 4 illustrates the trends in the number of Technical Reports published by the ABCC from 1959 to 1975. Early on, the ABCC began issuing Technical Reports that documented their research. Notably, in 1957, it began producing these reports in both Japanese and English. This was important as a gesture aimed at explaining the commission’s scientific studies of atomic bomb survivors to members of the Japanese society (including the Hiroshima and Nagasaki communities).
B-2. RIRBM: Trends in RIRBM Research
The RIRBM did not have any opportunity to establish a research framework reflecting the changes and organizational structure recommended in the Francis Report for ABCC-RERF. Instead, it had research projects for each of its internal divisions and laboratories. Although simple comparisons with the research conducted by the ABCC-RERF are not possible, examining both in parallel is worthwhile. First, the differences between the two research approaches are meaningful in themselves. Moreover, both institutions respected each other’s differences. Another point is that teams of ABCC-RERF and RIRBM researchers often collaborated with each other. This was beneficial whenever their respective research projects shared a similar scope, and also enabled them to minimize overlap in their research endeavors. The RIRBM did not apply the “fixed cohort” concept and it pursued its research without a unified research plan for various themes. We examined its research accomplishments, paying attention to these points.
As noted earlier, the RIRBM’s first Annual Report in 1960 was actually issued while its predecessor, the Institute for Nuclear Radiation Research, was still in operation. By 1975, the RIRBM had issued 16 Annual Reports containing references to and reports on a cumulative total of 170 research papers (Figure 5).
B-3. Comparison of the titles in ABCC’s Technical Reports and RIRBM’s Annual Report
The ABCC’s Technical Reports covered research with diverse content. Furthermore, almost all studies maintained a fundamental focus on the fixed cohorts described earlier. Figure 6A illustrates the percentage of titles in the Technical Reports that contained the following key words: radiation, leukemia, cancer (tumor, carcinoma), genetic, chromosome, and hematology. As a result of text analysis, the six most frequently used keywords were selected. Although these six terms symbolized fairly well-known themes relevant to the health effects on atomic bomb survivors, they did not occur very frequently (36.9% of all of the titles examined). The percentage of RIRBM’s Annual Report titles including the same six themes is 35.3%, similar to those in the ABCC reports (Figure 6B).

Among the six key words, “cancer” and “genetics” appeared in titles of the ABCC’s Technical Reports more than twice, compared with their appearance in the RIRBM annual report titles (Figure 6). On the other hand, “hematology” and “leukemia” appeared in titles of the RIRBM’s Annual Report at a higher percentage compared to those in the ABCC’s Technical Reports (Figure 6). In particular, the word “leukemia” was used in the tiles of the RIRBM’s Annual Report at an almost two-fold higher percentage (15.9%) than in the ABCC’s Technical Reports (9.3%).
It should be noted that there were 59 papers in the ABCC’s Technical Reports covering leukemia-related subjects including the comparative analysis with Nagasaki, autopsy study, and serialization at the time of the current study, while 27 papers were in the RIRBM’s Annual Reports. Considering that research undertakings at the RIRBM’s facilities were smaller in scale than the research done at the ABCC, it seems that the RIRBM’s research environment attracted significant interest in leukemia research.
DISCUSSION
In this study, we analyzed the titles of the ABCC’s Technical Reports and the RIRBM’s Annual Reports to reveal the difference in the research direction of these two institutions. The percentages of the titles in both the ABCC’s Technical Reports and the RIRBM’s Annual Reports, including these six keywords that symbolized the health effects on atomic bomb survivors, are not very high (around 35%). This is not to imply that low frequencies of occurrence are synonymous with a lack of research. The reason for the relatively low frequencies was that, in addition to these important and comprehensive themes, the ABCC and RIRBM also had projects on many more themes that were often linked with the foundational themes. Among the six key words, “cancer” and “genetics” appeared in titles of the ABCC’s Technical Reports more frequently compared to the RIRBM Annual Reports. The ABCC established by the country where the atomic bomb was dropped was able to predict the human effects of radiation to some extent from the beginning. Therefore, these two subjects could be important for the ABCC from the beginning. On the other hand, “hematology” and “leukemia” were used more frequently in titles of the RIRBM’s Annual Report compared to the ABCC’s Technical Reports. Since it was difficult for the RIRBM to make predictions and long-term plans without enough resources, the institute might try to solve immediate problems in the area. The direction of the research projects of these two institutions from their background may lead to the different usages of the key words concerning the health effects of the atomic bomb.
After the Second World War, there was a considerable gap in resources available for researchers in Japan and the U.S. In 1955, ten years after the atomic bombings, the ABCC formulated an integrated study plan that would facilitate the continuation of its research activities into the 21st century. Several deeply interrelated factors are believed to have made this possible. For example, the ABCC had access to the findings of U.S. atomic bomb research predating the actual use of the bomb in Japan in August 1945, as well as the findings of three early surveys of atomic bomb survivors in which the U.S. was involved. Another factor was the involvement of and assistance from the National Academy of Sciences (NAS) and the U.S. Department of Energy (DOE), both of which had a major influence on the ABCC operations. Under these influences, the ABCC was capable of investigating the information and analytical findings from collected biosamples and the fixed cohorts it had defined, and producing highly reliable, evidence-based research. On the other hand, it was very difficult, if not impossible, at that time for Japan to take the initiative with, or independently pursue, large-scale, high-quality epidemiological surveys or scientific studies on the health effects of exposure to radiation. Otherwise, it is conceivable that Japanese institutions would have acted to devise their own research themes in close cooperation with targeted communities and implement surveys through close interaction with atomic bomb survivors.
Despite its success in the large-scale program, the U.S.-derived ABCC faced exceptional difficulty in establishing communication with the communities affected by the atomic bombs. In that respect, the situation was profoundly different for the RIRBM. Hiroshima University’s School of Medicine and Hospital had been set up in Hiroshima, the site of the first atomic bombing and, as such, enjoyed strong ties with local physicians and medical societies. RIRBM was established within this setting and engaged in studies and surveys backed by close ties to the local community, the university, and the university hospital. Moreover, although its projects were relatively small in scale, they sought to investigate issues of importance that were in keeping with the expectations of the Japanese society, the Hiroshima community, and the atomic bomb survivors themselves. Leukemia was a topic of considerable concern for the Japanese society, Hiroshima, and the locale affected by the atomic bomb. At the time, Hiroshima University Hospital had expanded its patient wards with aid from the U.S. government in 1961 and actively expanded its medical care for atomic bomb survivors. As an institution that had its facilities adjacent to, and engaged in collaboration with researchers from, the Hiroshima University’s School of Medicine and Hospital, RIRBM was engaged in leukemia surveys and studies that were of value as medical research aimed at meeting the expectations of society.
In addition, RIRBM was able to conduct surveys of atomic bomb survivors living in districts outside Hiroshima that were not directly impacted by the bombing and to study as well as to provide long-term medical care to atomic bomb survivors who were exposed near the blast center. Moreover, Hiroshima-based surveys and studies (not limited to studies led by the RIRBM) enjoyed stronger influence because of their close proximity to the local government institutions that governed the welfare of atomic bomb survivors, for example, through recommendations for legislative action on the provision of aid and medical care to the survivors. Unlike the ABCC-RERF, the RIRBM did not employ fixed cohorts or establish a unified research program. However, it was arguably better-positioned to implement the surveys and studies that local society needed at that time. This was a crucial factor and basis for the RIRBM’s founding mission and is unquestionably the backbone underpinning its research activities today.
CONCLUSIONS
The most important initial research leading to the current understanding of radiation effects is a set of studies led by the ABCC, which started over 70 years ago. Yet, in reality, elucidating the full impact of the bombings is still a difficult challenge that has not been achieved. However, the understanding of that difficulty—how and why it has been difficult scientifically and socially—would be beneficial for current research in this field including studies on the current “Fukushima” problem and possibly other future problems associated with radiation protection. This would further help define the relevance and value of scientific research to society.
REFERENCES
- 1 Atomic Bomb Casualty Commission. 1959. Present Status. Technical Report 33–59 (Report of Ad Hoc Committee for Appraisal of ABCC Program). 1–4. https://www.rerf.or.jp/library/scidata/tr_all/1959-33.pdf
- 2 Atomic Bomb Casualty Commission. 1960. Technical Report 9–60 (ABCC-JNIH adult health study. Provisional research plan). 1.
- 3 The Hiroshima International Council for Health Care of the Radiation-Exposed. 2012. Targets and research program. Health effects from exposure to radiation from the atomic bomb. Revised second edition. 14–19.
- 4 The Manhattan District Atomic Bomb Investigating Groups. 1946. Final Report of Findings of the Manhattan District Atomic Bomb Investigating Groups at Hiroshima and Nagasaki. https://www-sdc.med.nagasaki-u.ac.jp/abcenter/manhattan/index_e.html
- 5 Matsuzaka, M. and Kimura, H. 1978. Research notes on the former ABCC. Nagasaki Medical Journal Issue 3: 313–318. https://ci.nii.ac.jp/naid/40002767194
- 6 Niizuma, S. 1945. Lieutenant Colonel Niizuma Seiichi’s documents: Joint study group under Imperial Headquarters Inquiry Commission (draft). August 7. 1945. Compiled (Hiroshima Peace Memorial Museum collection).
- 7 Radiation Effects Research Foundation, 1978. The Atomic Bomb Casualty Commission 1947–1975: A General Report on ABCC-JNIH Joint Research Program. https://catalog.hathitrust.org/Record/009753591
- 8 Science Council of Japan, editor. 1953. The Investigation Report on Atomic Bomb Disaster. Japan Society for the Promotion of Science
- 9 United States Atomic Energy Commission. 1951. (NP-3036) Medical Effects of Atomic Bombs in Japan, Army Institute of Pathology [United States Atomic Energy Commission]. https://digital.library.unt.edu./ark:/67531/metadc1019601/
- 10 United States Strategic Bombing Survey. 1946. The Effects of Atomic Bombs on Hiroshima and Nagasaki. Chairman’s Office. https://docs.rwu.edu/cgi/viewcontent.cgi?referer=https://www.google.co.jp/&httpsredir=1&article=1000&context=rwu_ebooks
- 11 Watanabe, S. 1960. The establishment of the Institute for Nuclear Radiation Research. Proceedings of The Institute for Nuclear Radiation Research (Hiroshima University School of Medicine), first edition. 1–2.