Abstract
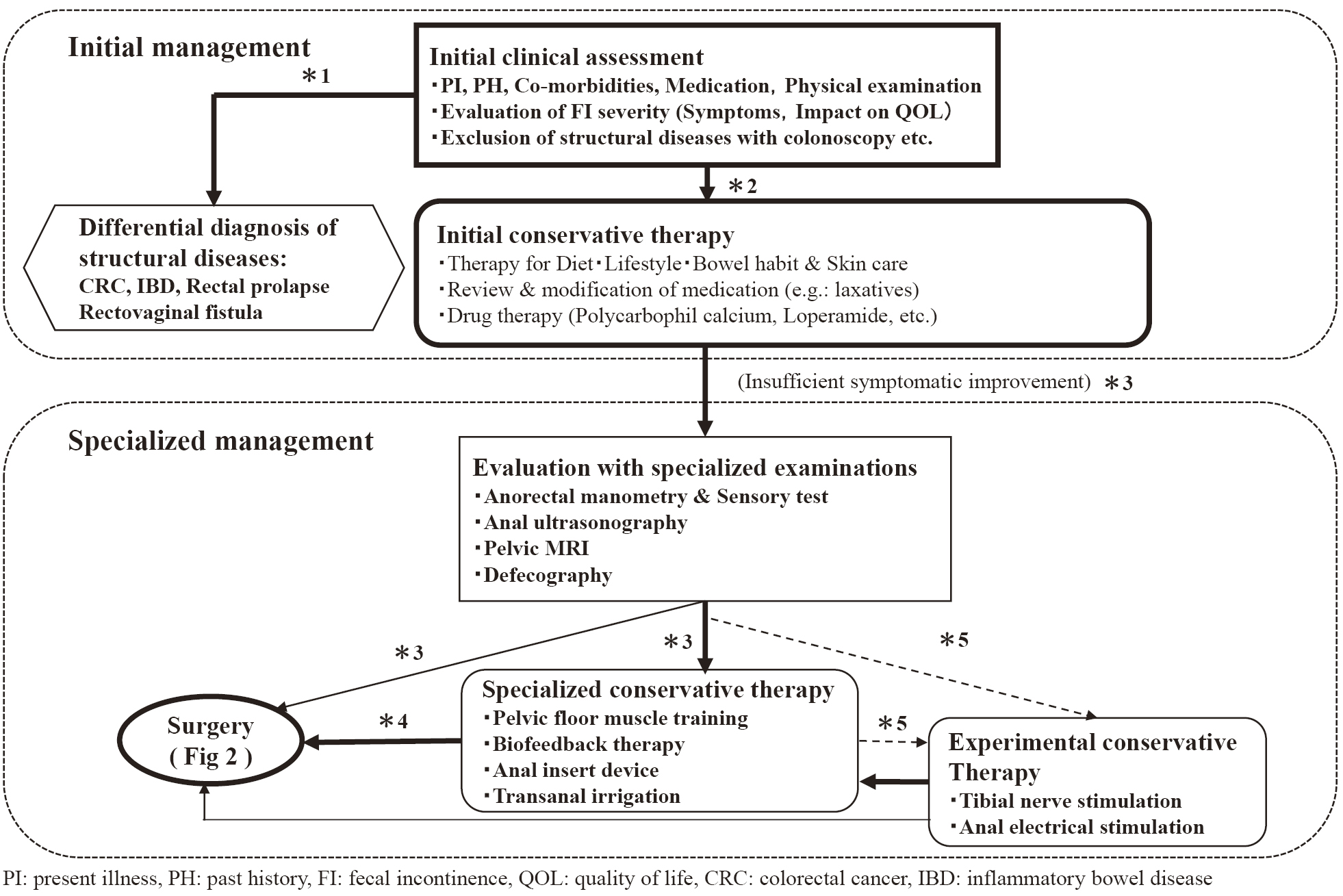
Fecal incontinence (FI) is defined as involuntary or uncontrollable loss of feces. Gas incontinence is defined as involuntary or uncontrollable loss of flatus, while anal incontinence is defined as the involuntary loss of feces or flatus. The prevalence of FI in people over 65 in Japan is 8.7% in the male population and 6.6% among females. The etiology of FI is usually not limited to one specific cause, with risk factors for FI including physiological factors, such as age and gender; comorbidities, such as diabetes and irritable bowel syndrome; and obstetric factors, such as multiple deliveries, home delivery, first vaginal delivery, and forceps delivery. In the initial clinical evaluation of FI, the factors responsible for individual symptoms are gathered from the history and examination of the anorectal region. The evaluation is the basis of all medical treatments for FI, including initial treatment, and also serves as a baseline for deciding the need for a specialized defecation function test and selecting treatment in stages. Following the general physical examination, together with history taking, inspection (including anoscope), and palpation (including digital anorectal and vaginal examination) of the anorectal area, clinicians can focus on the causes of FI. For the clinical evaluation of FI, it is useful to use Patient-Reported Outcome Measures (PROMs), such as scores and questionnaires, to evaluate the symptomatic severity of FI and its influence over quality of life (QoL).