Abstract
症例は65歳の女性で,近医で上腹部の腫瘤を指摘されて当院へ紹介された.腹部正中やや左寄りに可動性良好な手拳大の腫瘤を触れ,腹部USで内部に液体成分と乳頭状充実性成分が混在する球形腫瘤を認めた.CTでは膵頭部に直径約7 cm大の球形単房性囊胞性腫瘤を認め,囊胞壁から内腔に増殖する不整形充実成分が存在し,腫瘤尾側の主膵管拡張を認めた.腹部MRI所見では囊胞内に出血が示唆され,MRCPでは拡張した尾側の主膵管は,膵頭部で腫瘤の圧排により先細りとなっていた.Mucinous cystic neoplasmやsolid pseudo-papillary neoplasmなどを疑い,幽門輪温存膵頭十二指腸切除術を行った.病理所見は膵管内管状乳頭腫瘍であり,臨床的に分枝膵管発生と考えられた.術後合併症なく約3年間無再発生存中である.非典型的な画像所見を呈した分枝膵管発生の膵管内管状乳頭腫瘍を報告する.
Translated Abstract
We describe a case of a 65-year-old woman who was referred to our hospital because of a palpable mass in her upper abdomen. A mass with a mixture of cystic and solid components was identified by abdominal US. CT showed a round-shaped cystic tumor 7 cm in diameter on the head of the pancreas. Irregular solid components were observed in the cystic lumen and main pancreatic duct (MPD) distal to the tumor was dilated. MRI revealed that the fluid in the cyst was blood. On MRCP, dilated MPD was tapered by the tumor. Based on these findings, we suspected mucinous cyst neoplasm, intraductal papillary mucinous neoplasm, or solid pseudopapillary neoplasm, and performed pylorus-preserving pancreaticoduodenectomy. By postoperative pathological examination yielded a diagnosis of intraductal tubulopapillary neoplasm (ITPN). The patient had no postoperative complications and is alive after 3 years, without recurrence. We report a case of ITPN in the branch duct of the pancreas that showed atypical images.
はじめに
Intraductal tubulopapillary neoplasm(以下,ITPNと略記)は,2009年にYamaguchiら1)が提唱した概念で,2010年WHO分類に膵管内腫瘍の一つとして新しく掲載された.ITPNは,ほとんどが主膵管に発生する腫瘍で,典型例の画像的特徴や臨床像などは明らかにされつつあるが,そのかぎりではない症例も存在する.今回,我々は分枝膵管に発生し,典型的な画像所見を示さず術前診断に苦慮したITPNの症例を経験したので報告する.
症例
患者:65歳,女性
主訴:左上腹部腫瘤
現病歴:半年ほど前から体動時に腹腔内で固まりが移動する感覚があったが,放置していた.症状が持続するため近医で相談したところ,左上腹部の腫瘤を指摘され,精査目的に当科へ紹介された.
既往歴:特記事項なし.
家族歴:特記事項なし.
嗜好歴:喫煙なし.アルコール:缶ビール1缶/日
来院時現症:身長154 cm,体重42 kg,BMI 17.7 kg/m2
腹部は平坦・軟で,仰臥位で左上腹部に腫瘤による腹壁の隆起を認めた.腫瘤は手拳大,球形で硬かったが,可動性は良好であった.右側臥位で腫瘤は上腹部右側に移動し,座位では臍部まで下降した.
血液検査所見:末梢血検査に異常を認めず,生化学検査でも膵酵素,肝胆道系酵素などに異常を認めなかった.腫瘍マーカーは,CA19-9は102.8 U/mlと上昇していたが,CEA,エラスターゼ1は正常値であった.
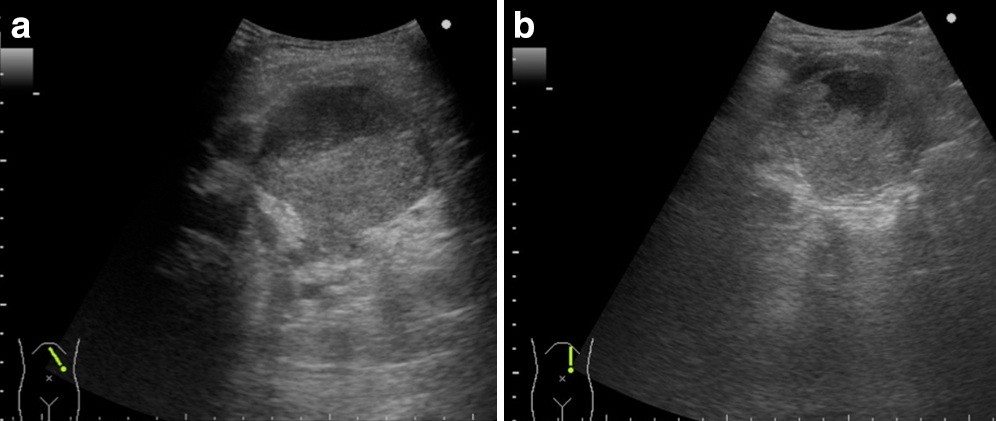
腹部超音波検査所見:腫瘤は約7 cm大の球形腫瘤として描出され,腫瘤内部は液体成分と乳頭状増殖を示す充実成分が占めていた(Fig. 1a, b).
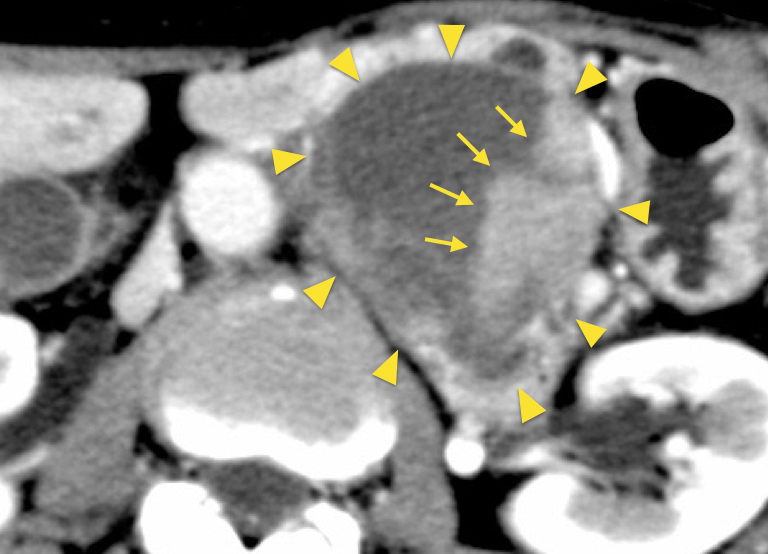
腹部造影CT所見:水平断で,左上腹部に直径約7 cm大の球形単房性囊胞性腫瘤を認めた.囊胞壁には,内腔側に増殖する造影効果を伴う不整形充実成分が存在した(Fig. 2).冠状断では,腫瘤より尾側の主膵管の拡張が認められ(Fig. 3a),腫瘤によって門脈から上腸間膜静脈は左側へ圧排されており,腫瘤の局在は膵頭部であった(Fig. 3b).
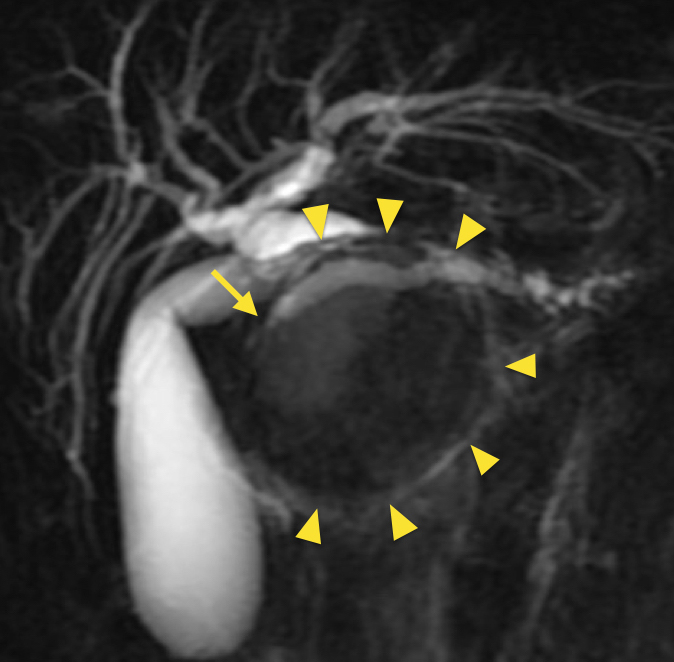
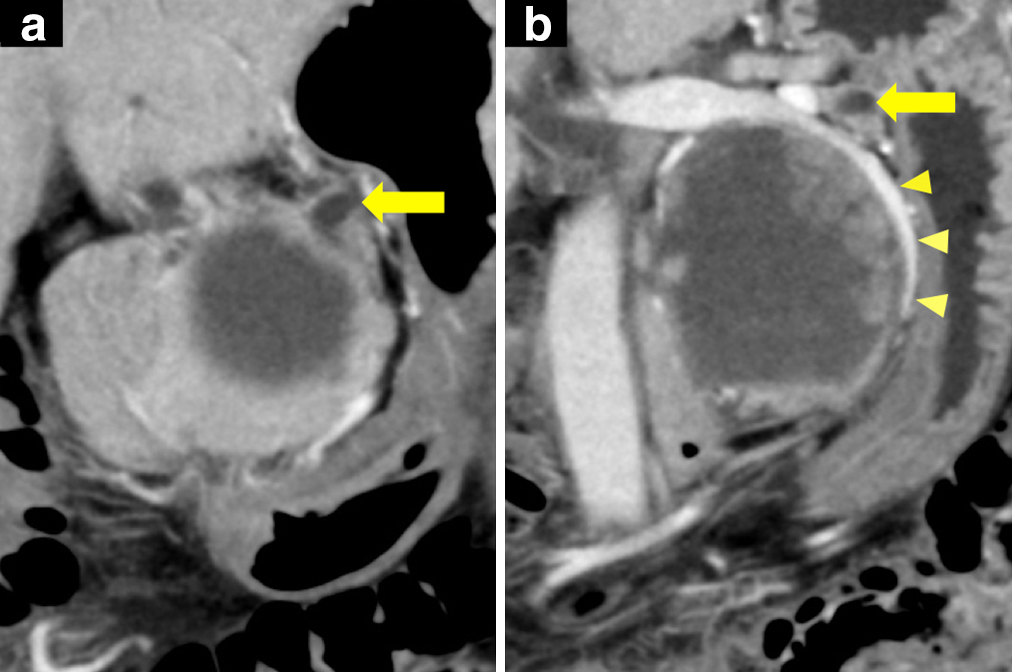
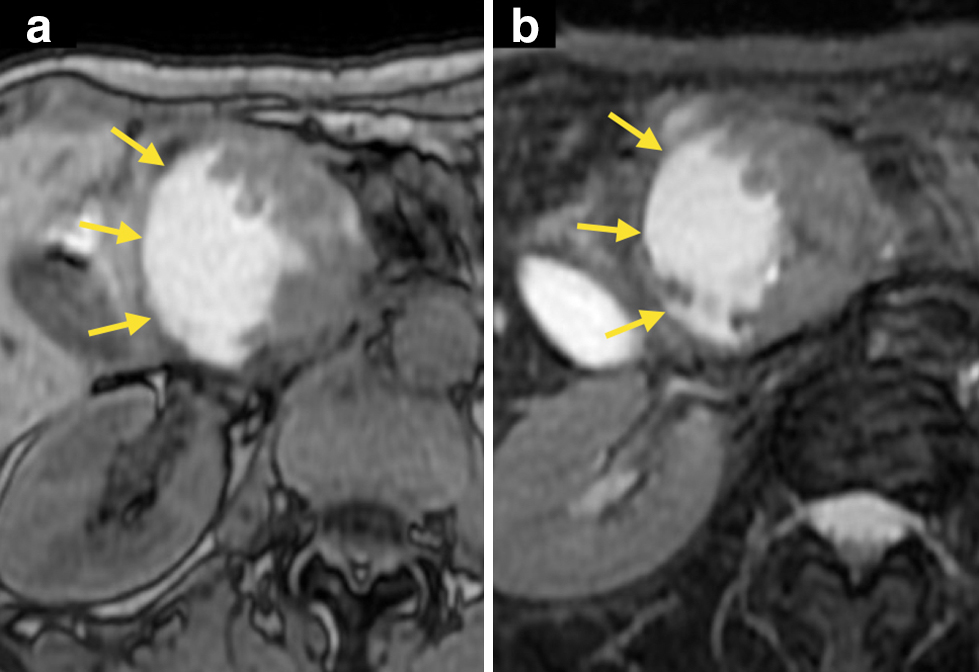
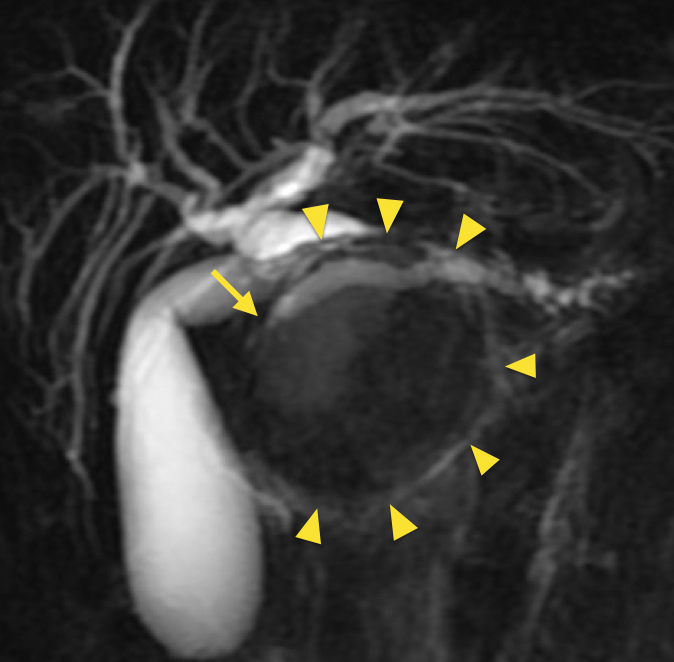
腹部造影MRI所見:MRI撮像時には,腫瘤は椎体の右側に移動しており,可動性に富む膵頭部の腫瘤であることが示唆された.腫瘤内の液体成分は,T1強調画像,T2強調画像でともに高信号を呈し,血液の存在が示唆された(Fig. 4a, b).腫瘤内の充実成分は,拡散強調画像で高信号を呈し,ダイナミック造影では早期から後期にかけて造影効果の増強を認めた.MRCPでは,膵頭部で腫瘤による圧排を受けた主膵管は,体尾部では拡張しており,腫瘤の腹側を走行する部分から膵頭側に向かって先細り状となっていた(Fig. 5).
以上の検査結果から,術前診断はmucinous cystic neoplasm,solid-pseudopapillary neoplasm,intraductal papillary mucinous neoplasmなどが考えられ,通常型の浸潤性膵管癌は否定的であった.いずれにしても切除の適応であり,ERCPおよびEUS-FNAは,検査結果によって治療方針を変更しえるものでないと考え,検査に伴う侵襲や合併症を回避するため,これらの検査は行わずに手術を行う方針とした.
手術所見:腫瘍は手拳大・球形で周囲への浸潤はなく,可動性は良好であった.術前画像診断通り腫瘍は膵頭部に存在し,上腸間膜動脈(superior mesenteric artery;SMA)および上腸間膜静脈(superior mesenteric vein;以下,SMVと略記)を圧排していたが浸潤はなかった.膵体尾部の主膵管は拡張し,膵実質は菲薄化し硬化していた.SMVの直上で膵臓を切離し,1群リンパ節郭清を伴う幽門輪温存膵頭十二指腸切除術を行った.再建はPPPD-II-A-2とした.
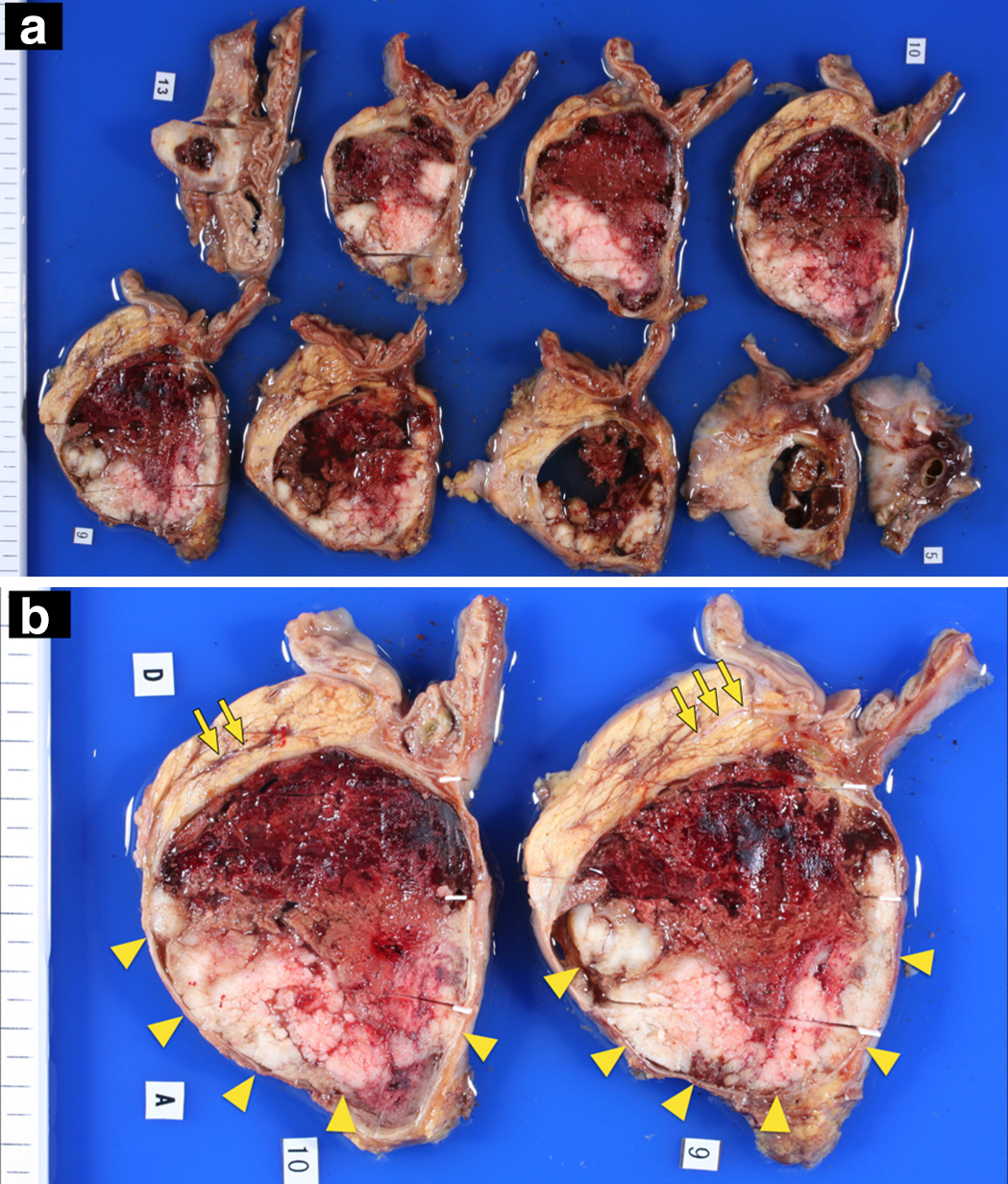
切除標本肉眼的所見:腫瘤は膵実質を圧排するように発育しており,割面では出血を伴った単房性囊胞性病変で,囊胞壁に沿って結節性に増殖した白色充実性腫瘍部分と,陳旧性血液貯留部分から構成され,肉眼的に明らかな粘液産生を認めなかった(Fig. 6a).圧排された主膵管は腫瘤の被膜外に認められ,分枝膵管から発生したものと考えられた(Fig. 6b).
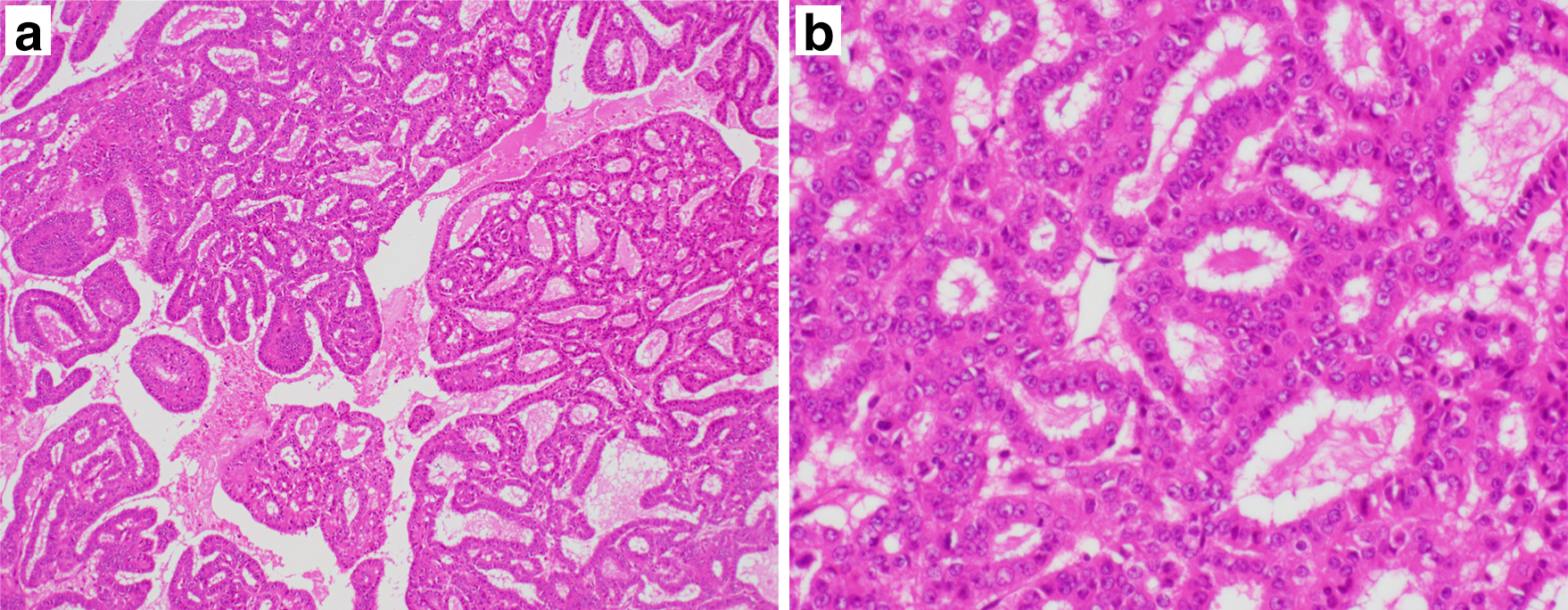
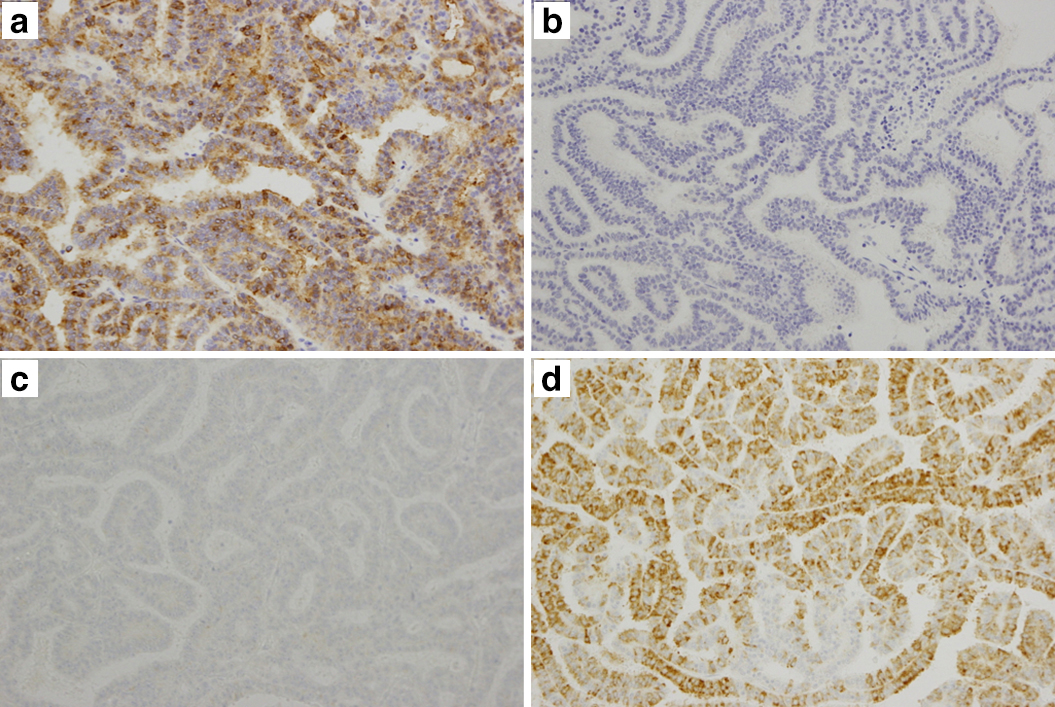
病理組織学的検査所見:囊胞は1層の円柱上皮で裏うちされており,浸潤性増殖は認められなかった.弱拡大では,細い線維性間質を有する腫瘍細胞が乳頭管状に増殖し,膵管内を占居していた(Fig. 7a).強拡大では,腫瘍細胞は好酸性の細胞質と明瞭な核小体を有し,腫大不整形核,核重積を伴っていた.腫瘍全体を標本化し,粘液の有無を検索したが,粘液産生はみられなかった(Fig. 7b).免疫組織学的所見として,MUC1およびMUC6染色は陽性,MUC2およびMUC5AC染色,抗トリプシン抗体は陰性であり,非浸潤性ITPNと診断された(Fig. 8).リンパ節転移を認めなかった.
術後経過:術後合併症なく,術後24日目に退院した.術後2年11か月間無再発生存中である.
考察
ITPNは,これまでintraductal tubular carcinoma(以下,ITCと略記)と呼ばれていた腫瘍を基盤とし,その定義概念を見直したもので,2009年にYamaguchiら1)によって提唱された概念である.ITPNはITCを包括し,さらには従来の分類でintraductal papillary mucinous neoplasm(IPMN)と診断されていた腫瘍の一部を含んでいる.Tubulopapillaryな増殖を特徴とする膵管内腫瘍で,粘液非産生性である.2010年に示された新WHO分類2)でこの概念が採用され,膵癌取扱い規約でも第7版3)で初めてITPNが分類された.
ITPNの肉眼的特徴としては,①膵管内に充満する結節状の腫瘍である,②粘液産生は認められない,ことが知られている.病理形態学的所見としては,③tubulopapillary growth patternを呈する,④細胞質は好酸性で明らかな粘液産生を示さない,⑤一様に高度異型上皮のみから構成される,⑥微小な壊死巣が多発する,ことが挙げられる.免疫組織化学的特徴としては,⑦MUC2およびMUC5ACが陰性,⑧抗トリプシン抗体が陰性,であることが明らかになっている.また,分子生物学的特徴として,⑨27%の症例で,PIK3CAなどを含むPIK3K pathwayの遺伝子に変異を認める4),⑩KRASおよびBRAFの変異を認めない,ことがわかっている.これらの特徴は,ITPNと通常型膵癌,腺房細胞癌との鑑別に重要である.
Yamaguchiら1)が,2009年に本邦から10例のITPNをはじめて報告して以来,2018年までに医学中央雑誌(キーワード:「膵管内管状乳頭腫瘍」or「intraductal tubulopapillary neoplasm」)とPubMed(キーワード:「intraductal tubulopapillary neoplasm」,「pancreas」)での検索で,本邦ITPN報告例は30例1)5)~22)であった(Table 1).自験例を含めた31例で臨床的特徴をみてみると,年齢は35~80歳,男女比は17:14で,膵頭部病変を有するものが22例と多い.非浸潤性病変が13例(41.9%),浸潤性病変が18例(58.1%)と浸潤性も少なくはなく,大きさは,非浸潤性が平均4.0 cmなのに対して,浸潤性は平均6.9 cmと大きい.リンパ節転移は1例のみと極めて少なく,再発や死亡の記載が明らかなものは5例1)7)11)17)で長期生存例も多く,予後は比較的良好といえる.
Table 1
Clinicopathological features of ITPN reported in Japan
| Case |
Author |
Year |
Age |
Sex |
Location |
Size (cm) |
2-tone duct sign |
MPD dilation |
Operation |
Invasion/Metastasis |
Prognosis |
| 1 |
Yamaguchi1) |
2009 |
60 |
F |
H |
6.0 |
abrupt disruption (Positive in a representative image) |
Positive in a representative image |
PPPD |
No |
Alive (7 mo) |
| 2 |
Yamaguchi1) |
2009 |
35 |
F |
B |
1.0 |
NR |
NR |
DP |
No |
Alive (42 mo) |
| 3 |
Yamaguchi1) |
2009 |
68 |
F |
H |
2.5 |
NR |
NR |
PD |
No |
Alive (12 mo) |
| 4 |
Yamaguchi1) |
2009 |
53 |
M |
B |
2.0 |
NR |
NR |
DP |
No |
Recurrence at 12 mo
Alive (18 mo) |
| 5 |
Yamaguchi1) |
2009 |
60 |
F |
H |
4.5 |
NR |
NR |
PPPD |
No |
Alive (9 mo) |
| 6 |
Yamaguchi1) |
2009 |
73 |
F |
H |
5.2 |
NR |
NR |
PD |
No |
Alive (10 mo) |
| 7 |
Yamaguchi1) |
2009 |
72 |
M |
B |
1.0 |
NR |
NR |
DP |
Stromal invasion |
Alive (14 mo) |
| 8 |
Yamaguchi1) |
2009 |
44 |
M |
H |
6.0 |
NR |
NR |
PPPD |
Stromal invasion |
Alive (66 mo) |
| 9 |
Yamaguchi1) |
2009 |
48 |
M |
HBT |
15.0 |
NR |
NR |
TP |
Multiple liver metastasis |
Dead (7 mo) |
| 10 |
Yamaguchi1) |
2009 |
70 |
M |
HB |
4.0 |
NR |
NR |
Sub-TP |
No |
Alive (24 mo) |
| 11 |
Shibasaki5) |
2012 |
61 |
M |
HBT |
11.5 |
abrupt disruption |
Positive |
TP |
Invasion to pancreas parenchyma |
Alive (14 mo) |
| 12 |
Jokoji6) |
2012 |
66 |
M |
BT |
1.8 |
abrupt disruption |
Positive |
DP |
Stromal invasion |
Alive (15 mo) |
| 13 |
Urata7) |
2012 |
78 |
F |
B |
2.2 |
cork-of-wine-bottle sign |
Positive |
DP |
Invasion to pancreas parenchyma |
Recurrence at 34 mo
Alive (43 mo) |
| 14 |
Matsushita8) |
2013 |
47 |
F |
H |
1.8 |
abrupt disruption |
Positive |
PD |
Minor invasion |
Alive (30 mo) |
| 15 |
Kasugai9) |
2013 |
69 |
F |
HBT |
12.0 |
cork-of-wine-bottle sign |
Positive |
TP |
No |
Alive (24 mo) |
| 16 |
Ito10) |
2014 |
75 |
M |
B |
1.8 |
cork-of-wine-bottle sign |
Positive |
DP |
Invasion to pancreatic duct |
NR |
| 17 |
Matsuda11) |
2014 |
71 |
M |
BT |
9.0 |
abrupt disruption |
Positive |
DP |
Portal vein tumor thrombus |
Dead (21.5 mo) |
| 18 |
Furuhata12) |
2014 |
74 |
M |
H |
7.0 |
NR |
NR |
NR |
Duodenal invasion |
NR |
| 19 |
Tajima13) |
2015 |
80 |
M |
HB |
0.5 |
abrupt disruption |
NR |
NR |
No |
Alive (12 mo) |
| 20 |
Takayama14) |
2015 |
54 |
F |
H |
5.0 |
cork-of-wine-bottle sign |
Positive |
PD |
Duodenal invasion |
Alive (over 10 mo) |
| 21 |
Yoshida15) |
2015 |
75 |
M |
H |
1.2 |
Negative |
Negative |
PD |
No |
NR |
| 22 |
Kitaguchi16) |
2015 |
61 |
M |
H |
1.2 |
abrupt disruption |
Positive |
SSPPD |
Stromal invasion |
Alive (22 mo) |
| 23 |
Kitaguchi16) |
2015 |
75 |
F |
B |
10.0 |
NR |
NR |
DP |
Yes (details unknown) |
Alive (51 mo) |
| 24 |
Kitaguchi16) |
2015 |
67 |
M |
HBT |
6.5 |
NR |
NR |
TP |
Yes (details unknown) |
Alive (84 mo) |
| 25 |
Nagai17) |
2016 |
61 |
M |
HB |
14.0 |
cork-of-wine-bottle sign |
Positive |
TP |
Splenic vein tumor thrombus |
Recurrence at 36 mo
Alive (41 mo) |
| 26 |
Date18) |
2016 |
54 |
F |
H |
5.5 |
abrupt disruption |
Positive |
PD |
Yes (details unknown) |
Alive (24 mo) |
| 27 |
Fujimoto19) |
2017 |
74 |
M |
HB |
17.5 |
abrupt disruption |
Positive |
TP |
Invasion to pancreas parenchyma, Serosal invasion, Retropenitoneal invasion, Lymph node metastasis |
Alive (9 mo) |
| 28 |
Sakurai20) |
2017 |
64 |
M |
HBT |
7.5 |
Negative |
Negative |
TP |
Stromal invasion |
Alive (24 mo) |
| 29 |
Umemura21) |
2017 |
50 |
F |
B |
1.5 |
abrupt disruption |
Positive |
DP |
No |
Alive (24 mo) |
| 30 |
Inomata22) |
2018 |
55 |
F |
H |
5.0 |
Negative |
Negative |
PPPD |
No |
Alive (34 mo) |
| 31 |
Our case |
|
65 |
F |
H |
7.2 |
Negative |
Positive |
PPPD |
No |
Alive (35 mo) |
Size is represented by the maximum width of the tumor.
B indicates body; BT, body and tail; DP, distal pancreatectomy; F, female; H, head; HB, head and body; HBT, head, body and tail; M, male; mo, months; MPD, main pancreatic duct; NR, not reported; PD, pancreaticoduodenectomy; PPPD, pylorus-preserving pancreaticoduodenectomy; TP, total pancreatectomy.
一般にITPNは主膵管に発生することが多いため,腫瘍を挟んで主膵管のupstream(尾側)のみが拡張し,充実性の腫瘍が主膵管内にはまり込んでいるようにみえるとされている.すなわち,MRCPあるいはERCPで,腫瘍周囲に膵液が同定される場合はcork-of-wine-bottle signと呼ばれ,同定できない場合はabrupt disruptionと呼ばれる途絶様にみえる.いずれも,腫瘍部分と膵管拡張部分がはっきりと区別され,造影CTでは前者が“白”で後者が“黒”となり,T2強調画像やMRCP,ERCPでは前者が“黒”で後者が“白”となる(2-tone duct sign)23)24).2-tone duct signの検査感度は高くない24)が,ITPNの特徴的画像所見とされており,本邦報告例の約半数で認められている.
本邦報告例の中で,画像検査所見および切除標本肉眼的所見からITPNが分枝膵管発生と診断された症例は2例15)22)であった.自験例を含めて,いずれも2-tone duct signを欠いているが,その理由は異なる.自験例以外の2例では,主膵管が拡張しておらず,2-tone duct signを示さなかった.一方で自験例では,主膵管は圧排され偏位し,尾側膵管は拡張しているが,主膵管発生例のような途絶ではなく,膵頭側へ先細りとなる形態であったために,2-tone duct signを示さなかった.
また,本症例では充実成分よりも出血による液体成分の方が腫瘍内部を多く占居する単房性囊胞の画像所見を呈した.これは,腫瘍内に相当量の出血があったためであるが,出血を伴ったITPN症例は過去には2例のみ12)14)で,これらはいずれも出血壊死部分は大きくなかったため,液体成分はさほど目立たなかった.
以上の2点が過去の報告にはみられない特異な所見であった.
本症例は,分枝膵管発生,腫瘍内への相当量の出血によって,非典型例の示す新たな画像を呈しており,今後のITPN診断において重要と考え報告した.
なお,本論文の要旨は第47回日本膵臓学会大会・第20回国際膵臓学会・第6回アジアオセアニア膵臓学会(2016年8月,仙台)で報告した.
利益相反:なし
文献
- 1) Yamaguchi H, Shimizu M, Ban S, Koyama I, Hatori T, Fujita I, et al. Intraductal tubulopapillary neoplasms of the pancreas distinct from pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasm. Am J Surg Pathol. 2009;33:1164–1172.
- 2) Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO Classification of Tumors of the Digestive System. 4th Edition. Lyon: International Agency for Research on Cancer; 2010. p. 304–313.
- 3) 日本膵臓学会編.膵癌取扱い規約.第7版.東京:金原出版;2016. p. 69.
- 4) Basturk O, Berger MF, Yamaguchi H, Adsay V, Askan G, Bhanot UK, et al. Pancreatic intraductal tubulopapillary neoplasm is genetically distinct from intraductal papillary mucinous neoplasm and ductal adenocarcinoma. Mod Pathol. 2017 Dec;30(12):1760–1772.
- 5) 柴﨑 泰, 坂口 孝宣, 稲葉 圭介, 鈴木 昌八, 馬場 聡, 今野 弘之.膵全摘にて根治した膵intraductal tubulopapillary neoplasmの1例.日本臨床外科学会雑誌.2012;73:2061–2067.
- 6) Jokoji R, Tsuji H, Tsujimoto M, Shinno N, Tori M. Intraductal tubulopapillary neoplasm of pancreas with stromal osseous and cartilaginous metaplasia; a case report. Pathol Int. 2012;62:339–343.
- 7) Urata T, Naito Y, Nagamine M, Izumi Y, Tonaki G, Iwasaki H, et al. Intraductal tubulopapillary neoplasm of the pancreas with somatic BRAF mutation. Clin J Gastroenterol. 2012;5:413–420.
- 8) 松下 克則, 森本 脩邦, 元木 祥行, 岡野 美穂, 足立 真一, 平尾 隆文,ほか.術前診断が困難であったITPNの1例.日本消化器外科学会雑誌.2013;46:196–202.
- 9) Kasugai H, Tajiri T, Takehara Y, Mukai S, Tanaka J, Kudo SE. Intraductal tubulopapillary neoplasms of the pancreas: case report and review of the literature. J Nippon Med Sch. 2013;80(3):224–229.
- 10) 伊藤 裕幸, 今井 仁, 矢崎 利典, 市川 仁志, 永田 順子, 小嶋 清一郎,ほか.小膵癌との鑑別が困難であった膵ITPNの1例.Progress of Digestive Endoscopy.2014;84(1):200–201, 21.
- 11) 松田 正道, 渡邊 五朗, 橋本 雅司, 佐々木 一成, 田村 哲男, 今村 網男,ほか.門脈内腫瘍栓を伴ったintraductal tubulopapillary neoplasm浸潤癌の1例.膵臓.2014;29(4):729–735.
- 12) Furuhata A, Minamiguchi S, Mikami Y, Kodama Y, Sumiyoshi S, Adachi S, et al. Intraductal tubulopapillary neoplasm with expansile invasive carcinoma of the pancreas diagnosed by endoscopic ultrasonography-guided fine needle aspiration: a case report. Diagn Cytopathol. 2014;42(4):314–320.
- 13) Tajima S. Intraductal tubulopapillary neoplasm of the pancreas suspected by endoscopic ultrasonography-fine-needle aspiration cytology: report of a case confirmed by surgical specimen histology. Diagn Cytopathol. 2015;43(12):1003–1006.
- 14) Takayama S, Maeda T, Nishihara M, Kanazawa A, Chong HS, Oka H. A case of intraductal tubulopapillary neoplasm of pancreas with severe calcification, a potential pitfall in diagnostic imaging. Pathol Int. 2015 Sep;65(9):501–506.
- 15) Yoshida Y, Matsubayashi H, Sasaki K, Kanemoto H, Uesaka K, Ono H, et al. Intraductal tubulopapillary neoplasm of the pancreatic branch duct showing atypical images. J Dig Dis. 2015;16:357–361.
- 16) Kitaguchi K, Kato Y, Kojima M, Okubo S, Takahashi D, Okada R, et al. A resected case of intraductal tubulopapillary neoplasm of the pancreas: report of a case. Int Surg. 2015;100(2):281–286.
- 17) 永井 英雅, 湯浅 典博, 竹内 英司, 後藤 康友, 三宅 秀夫, 宮田 完志,ほか.膵全摘を施行した脾静脈内腫瘍栓を伴った膵管内管状乳頭腫瘍の1例.日本臨床外科学会雑誌.2016;77(3):650–656.
- 18) Date K, Okabayashi T, Shima Y, Iwata J, Sumiyoshi T, Kozuki A, et al. Clinicopathological features and surgical outcomes of intraductal tubulopapillary neoplasm of the pancreas: a systematic review. Langenbecks Arch Surg. 2016;401:439–447.
- 19) Fujimoto Y, Tomimaru Y, Tamura H, Noguchi K, Nagase H, Hamabe A, et al. Pancreatic intraductal tubulopapillary neoplasm with associated invasive cancer successfully treated by total pancreatectomy: a case report. Oncol Lett. 2017 Jul;14(1):153–158.
- 20) 櫻井 翼, 江上 拓哉, 長尾 祐一, 山内 潤身, 中島 洋, 鬼塚 幸治,ほか.膵全摘を施行したAFP産生性intraductal tubulopapillary neoplasmの1例.日本消化器外科学会雑誌.2017;50(7):552–562.
- 21) Umemura A, Ishida K, Nitta H, Takahara T, Hasegawa Y, Makabe K, et al. A rare case of intraductal tubulopapillary neoplasm of the pancreas rupturing and causing acute peritonitis. Case Rep Gastroenterol. 2017;11:661–666.
- 22) Inomata K, Kitago M, Obara H, Fujii-Nishimura Y, Shinoda M, Yagi H, et al. Concurrent presentation of an intraductal tubulopapillary neoplasm and intraductal papillary mucinous neoplasm in the branch duct of the pancreas, with a superior mesenteric artery aneurysm: a case report. World J Surg Oncol. 2018;16:83.
- 23) 市川 新太郎, 本杉 宇太郎.膵管内管状乳頭状腫瘍(ITPN)の画像診断.臨床放射線.2015;60(8):985–990.
- 24) Motosugi U, Yamaguchi H, Furukawa T, Ichikawa T, Hatori T, Fujita I, et al. Imaging studies of intraductal tubulopapillary neoplasms of the pancreas: 2-tone duct sign and cork-of-wine-bottle sign as indicators of intraductal tumor growth. J Comput Assist Tomogr. 2012;36:710–717.