Abstract
Introduction: Myelography and computed tomographic myelography (CTM) are widely used before spinal surgery. Findings that cannot be detected on magnetic resonance imaging (MRI) can sometimes be observed using myelography/CTM, which may result in changes in the surgery plans. In this study, we examined the usefulness of myelography/CTM in planning for lumbar surgery.
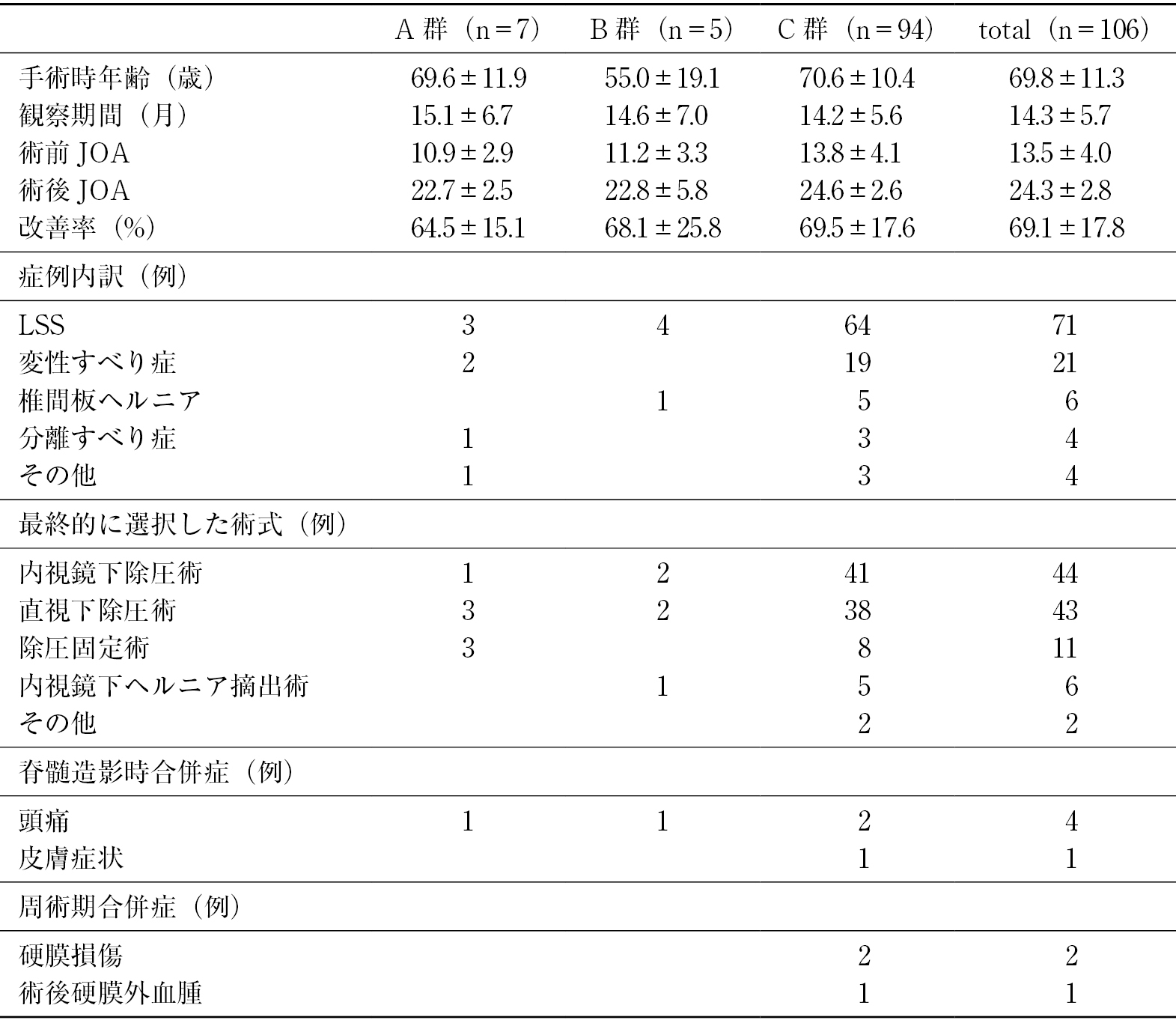
Methods: A total of 106 patients who underwent preoperative myelography were categorized into three groups: Group A, operation plans were changed or the decision to operate was taken after myelography/CTM; Group B, although new findings were observed on myelography/CTM, operation plans were not changed; and Group C, there were no new findings compared with MRI.
Results: Seven (6.6%) patients were classified into Group A: dynamic stenosis and increased decompression levels detected in three cases using myelography; lumbar spinal instability and presence of interbody fusions in three cases using myelography; and superior facet syndrome using CTM, leading to surgery in one case. Five cases (4.7%) were classified into Group B: ossification of the yellow ligament was detected on CTM in three cases; lumbar spondylosis, which was not identified on X-ray or MRI, was detected on CTM in one case; and a nerve root anomaly that could not be recognized on MRI was detected on CTM in one case. Ninety-four (88.7%) cases were classified into Group C.
Conclusions: Myelography/CTM aids in the recognition of the dynamic factors and understanding the pathophysiology of nerve root compression. It is a useful radiographic modality in planning for lumbar surgery.