Case Report
Bear attack injuries including canalicular lacerations and amputated finger: report of 2 cases
 https://ror.org/03rq2h425
https://ror.org/03rq2h425 2025 Volume 49 Pages 43-47
Details
2025 Volume 49 Pages 43-47
We report on two cases of bear attack injuries involving a nasal fracture, canalicular laceration, and an amputated finger. Emergency surgeries, including wound washing, canaliculus repair, and amputated finger replantation, were performed. In one case, canalicular laceration was detected six months post-operatively, which required multiple re-operations. In another case, the post-operative course of the replanted finger was uneventful for the first 10 days; however, necrosis occurred suddenly on post-operative day 11 and required additional surgery. Our cases suggest that we should carefully assess for canalicular laceration in the setting of facial injury on arrival, and that for amputated finger injury by bear attack, observation after replantation surgery should be longer than typically recommended in previously reported cases.
鼻骨骨折, 涙小管断裂, 小指切断などを受傷した2例のクマによる外傷の治療を経験した. 緊急で創洗浄および創閉鎖, 鼻骨骨折の整復, 涙小管断裂の再建および切断指再接着などを施行した. 1例において受傷6か月後に涙小管断裂が見つかり, 以降2度の涙小管の修復を要した. また,切断指を伴う症例において経過良好であった接着指が術後11日目に壊死し, 皮弁による再建を要した. 2例を通じ, クマによる顔面の外傷では初期評価において涙小管断裂の有無を確認することや切断指の場合には再接着後, 通常よりも長期間の観察が重要であることなどが示唆された.
The number of bear sightings in the Shimane Prefecture reached a record high in these last three months by 1.6 times year-to-year1), as was also seen nationwide. Bears are naturally cautious animals that generally prefer to avoid humans; however, when they are protecting their young or feel they are feared, they can become aggressive2). The number of bear attacks is expected to increase as the number of bear sightings increases over the years. Herein, we report two cases of injuries from bear attacks.
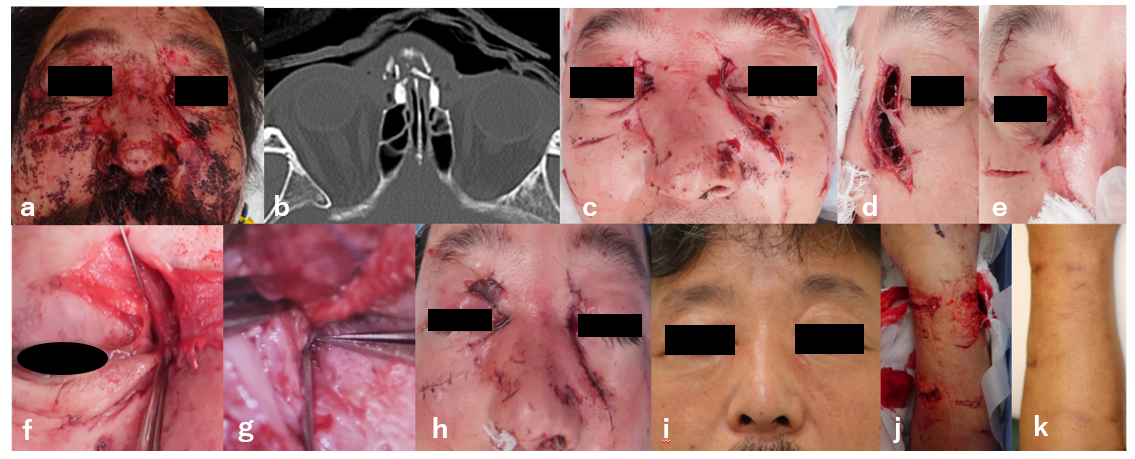
Case 1: A 44-year-old man without notable medical history was attacked by a bear while mushroom hunting in November, 20XX and was referred to our hospital for treatment. On his arrival, vital signs were normal but multiple lacerations on the face and both forearms were observed (Figure 1a,e-f). X-ray of facial bones revealed a nasal fracture. Emergency surgery, including thorough irrigation of the wound with 10 liters of saline and reduction of the nasal bone fracture, was performed under general anesthesia (Figure 1b). Prophylactic cefazolin 1g every six hours was started on arrival and was continued for seven days post-operatively. The wound culture on arrival was negative for any bacterial growth. The patient was discharged on post-operative day 11. Follow-up at three months post-operatively showed epiphora in his right eye, but his symptoms were reportedly improving so the decision was made to continue with observation. However, at the six-month follow-up visit, he was found to have persistent epiphora without improvement. Surgery for his epiphora was planned for nine months after the index operation, and microscopic examination revealed a common canalicular laceration. Anastomosis of the laceration was performed; a silicone tube was placed inside to prevent obstruction and removed three months post-operatively. Four and a half months after the canalicular repair, the epiphora had recurred and another operation was performed. Obstruction of the repaired canaliculus due to scar formation was observed, and subsequently scar resection, canaliculus anastomosis to the lacrimal sac, and silicone tube placement were performed (Figure 1i-l). The silicone tube was removed three months post-operatively and there were no signs of recurrence (Figure 1m,n).

Case 2; A 51-year-old healthy forestry worker who was attacked by a mother bear defending her cubs, with multiple lacerations on the face and forearms and an amputated finger of the left 5th digit (Figure 2a, Figure 3a), was transferred to the hospital by helicopter on March, 20XX. On arrival, vital signs were normal other than a blood pressure of 205/104 mmHg. X-ray of the facial bones revealed a comminuted nasal fracture and partial distal phalangeal involvement of the amputated portion (Figure 2b, Figure 3b). Emergency repair surgeries, including thorough irrigation, canalicular repair of the right eye with silicone tube placement, reduction of the nasal bone and septum, and replantation of the digit with a venous graft, were performed under general anesthesia (Figure 2c-h, Figure 3c-e). Piperacillin/tazobactam were selected as prophylactic antibiotics and started at a dosage of 4.5g every six hours. Wound cultures from the nose and forearm were positive for Staphylococcus epidermidis but those from the amputated finger were negative. The facial wounds healed without any complications. On examination, the replanted digit displayed a slightly congestive appearance up to two days post-operatively, and thus the decision was made to make a fish-mouth incision to promote active bleeding and reduce congestion. Digit survival was confirmed by bleeding from the fish-mouth incision. The patient subsequently had fresh-colored bleeding after a pin-prick which was performed each day for the next 10 days post-operatively (Figure 3f-i). However, on post-operative day 11, necrosis of the replanted portion occurred with no bleeding noted. (Figure 3j,k). Purulent discharge was also observed arising from the necrotic digit. The digit was reconstructed using an oblique triangular flap on 14 days post-operatively (Figure 3l-o). No major complications were noted at follow-up visit six weeks post-operatively.

Although bears used to emerge from hibernation in mid-April2), there have been reports of bears coming out earlier nationwide, as was seen in case 2 which occurred in March. As seen in case 1, bear attacks are common during wild plant picking from September to November3), whereas in case 2, the patient was injured by a bear protecting her cubs, which is consistent with the natural aggressive behavior of bears2). Facial injuries account for 90% of bear attack injuries, reflecting bears’ tendencies to target victims’ faces. Arms are also commonly targeted body parts, which victims often use to protect themselves4). Both cases involved injuries to both the face and arms. The extent of damage from facial injuries caused by bears is often deeper than it may appear, sometimes involving canalicular laceration4) or optic nerve avulsion5) that can result in persistent epiphora or visual impairment. Therefore, careful initial assessment is important to clarify the presence of ocular involvement. Indeed, in case 1, canalicular laceration could not be detected until six months after trauma. Successful repair of canalicular laceration has been reported when performed within a week after the injury. If repair is done later than one month after the injury, increased risk of canalicular obstruction due to scarring has been reported6,7). Indeed this was seen in case 1, where the canalicular laceration was found six months after initial injury and required repair surgery twice.
The replanted digit in case 2 suddenly became necrotic on 11 days post-operatively, which is a very rare manifestation, given that complications after replantation surgery generally occur within 48 hours8). Moreover, the average period of neovascularization in the replanted digit is approximately seven days, after which the incidence of complications decreases8). There are currently no reports of any finger amputations secondary to bear attacks. However, there are reports on finger amputations from dog attacks, where the infection rate increases by a factor of 1.5 when the hand is involved compared to other body parts9).
There is one report on bear attacks regarding a bitten arm, in which the bear bite to the arm resulted in osteomyelitis10). Although the wound culture of the digit in case 2 was negative on arrival, local infection might have occurred in the digit, which could ultimately have been what led to the necrosis. Presence of purulent discharge also supports this idea. Thus, longer observation is recommended after replantation of a finger amputated by a bear bite.
The bacteriology of bear bite wounds does not seem to show a predominance of any specific bacteria including Staphylococcus epidermidis11) which was positive in case 2. Thus, empirical broad-spectrum agents with activity against Staphylococcus aureus and aerobic gram-negative rods are generally recommended11) as was done in case 1 and 2. Whether immediate wound closure should be performed in bear bite injuries is a concern for surgeons in terms of infection. For example, in dog bites, in contrast to injuries of the hand, facial injuries are known to be less likely to be infected because of adjacent robust perfusion and vascularity, which allows for prompt primary closure of the wound after thorough irrigation and administration of antibiotics12,13). Additionally, ample perfusion aids in shortening the healing course in facial injuries compared to injuries in the upper extremities4). Indeed, the facial injuries in both cases manifested in rapid healing without infection after primary closure of the wounds.
Our cases suggest that careful initial assessment for ocular involvement, such as canalicular laceration, and longer observation periods after replantation surgery of the amputated finger are important in injuries from bear attacks.
We would like to express our special appreciation and thanks to the staff of advanced emergency and critical care center in Shimane Prefectural Central Hospital and Dr. Olivia Cheng, MD(Weill Cornell Medicine, NewYork Presbyterian Brooklyn Methodist Hospital)for the primary care and language and grammatical editing, respectively.