Abstract
A next generation fetal electrocardiogram (ECG) that can assess fetal well-being
accurately is required in clinical settings. We developed a fetal ECG monitoring system
that acts via the maternal abdominal wall and measured the ECG in our clinical studies. To
assess the accuracy of the clinical fetal ECG monitoring records, it was necessary to
confirm that the waveforms obtained by the indirect lead had the same accuracy as those by
the direct lead. This study is translational research in which a murine fetal ECG system
with the direct lead that we had already developed was applied and pregnant rabbits that
had enough space to place electrodes on the maternal abdominal surface were used. In this
study, fetal ECG was measured using the direct and indirect lead simultaneously using
pregnant rabbits. The R-squared value between the RR-intervals obtained by the direct lead
and those by the indirect lead of the same fetus was used to determine the reliability of
the clinically developed fetal ECG monitoring system. The fetal ECG waveform, both with
the direct and indirect lead, was obtained from three out of five pregnant rabbits. The
average R-squared value was 0.99. Although one of the three pregnant rabbits presented
with an atrioventricular block during the measurement, the fetal ECG waveform was
successfully extracted with both the direct and indirect lead. The results of this study
demonstrate that the fetal ECG monitoring system that acts via the maternal abdominal wall
has the same accuracy as that of the direct lead.
Highlights
We evaluated the reliability of a fetal electrocardiogram that acts via the maternal
abdominal wall of rabbits. We used three pregnant rabbits to measure and compare the direct
and indirect ECG of the same fetus simultaneously. The R-squared value between the
RR-intervals obtained by the direct lead and those by the indirect lead of the same fetuses
in three pregnant rabbits was 0.99. The results of this study demonstrate that the fetal ECG
monitoring system that acts via the maternal abdominal wall has the same accuracy as that of
the direct lead.
Introduction
A cardiotocometer, a medical device that detects fetal heart rates using noninvasive
ultrasound and calculates them consecutively, is widely used in clinical settings. The
device observes the longitudinal fetal heart rate and estimates fetal well-being. With the
device, the health of the fetal can be deduced; however, fetal malfunction cannot be
detected. Consequently, unnecessary cesarean sections have occurred due to the
false-positive rate. In addition, the device has not contributed to a reduction in the rate
of cerebral palsy.
Electrocardiogram (ECG) waveforms were first recorded by Dutch physiologist Willem
Einthoven in 1903. Since then, research has been focused on the development of devices to
measure the electrical activities of fetal hearts [1].
Unfortunately, a practical fetal ECG monitoring system has not been developed as of yet.
However, advances in technology have enabled fetal ECG to measure heart rate via the
maternal abdominal wall. We developed a fetal ECG system that acts via the maternal
abdominal wall to monitor and measure fetal ECG waveforms in our clinical studies [2].
As the system is practical in the clinical setting, the measurement data should be accurate
enough for clinical demands. We must understand how the accuracy of the ECG monitoring
system that acts via the maternal wall compares to that of the direct lead. A fetal ECG can
be obtained by the direct lead in mice [3], but mouse
maternal abdomens do not have enough space to place an adequate number of electrodes for the
measurement of the fetal ECG waveforms. As a result, in mice, the accuracy of fetal ECG
waveforms obtained via the maternal wall cannot be assessed by comparing those with the
direct lead. Therefore, we used rabbits for this translational study from our mouse studies
and to our clinical studies. The aim of this study was to assess the accuracy of the ECG
waveform output of a fetus simultaneously measured using the direct and indirect lead in
pregnant rabbits. The R-squared value between the RR-intervals obtained by the direct lead
and those by the indirect lead of the same fetus was used to determine the reliability of
the clinically developed fetal ECG monitoring system.
Materials and Methods
This study was approved by the Animal Research Committee of Tohoku University (approval
number: 2011 idou-59).
Animals
Five pregnant rabbits (Kbs: JW; Kitayama Labels Co., Ltd., Ina, Japan) at 24 days were
used in this study. All rabbits were exposed to a suitable environment for acclimatization
(a 12-hr light/dark cycle at 24°C) before experiments.
Anesthetic management
Pregnant rabbits were anesthetized intramuscularly with ketamine (10 mg Ketalar/kg;
Daiichi Sankyo, Tokyo, Japan) and xylazine (1.5 mg Seractar/kg; Bayer Pharmaceutical Co.,
Ltd., Tokyo, Japan). After intubation according to an intubation protocol by Morgan and
Glowaski [4], maintenance of anesthesia by mask
inhalation was achieved using 2% isoflurane (2 L Forane/min; Abbott Japan Co., Ltd.,
Osaka, Japan) and room air. The airway pressure was set at <15 mmHg and ventilation
frequency was set to 20 breaths/min using mechanical ventilation (ARF-900; ACOMA Medical
Industry Co., Ltd., Tokyo, Japan).
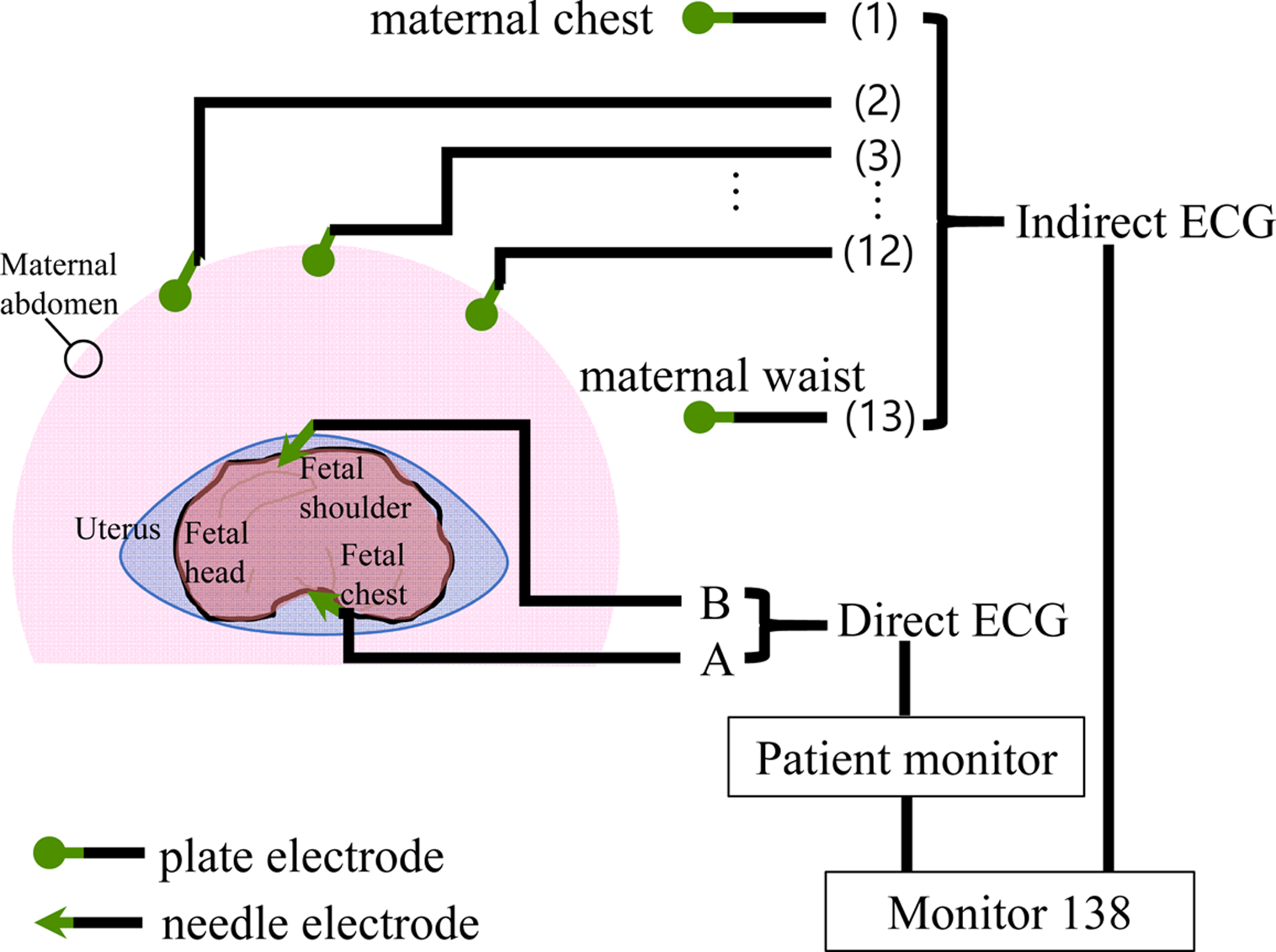
Direct ECG monitoring
After assuring that the level of anesthesia was stable, the uterus was exposed by a
maternal abdominal midline incision. One fetus was chosen to measure ECG waveforms for
each pregnant rabbit. A pair of needle electrodes were inserted into the uterus and fixed,
with one tip located near the fetus shoulder and the other tip located at the fetus chest.
The electrodes were used for the direct ECG monitoring. The signals obtained via an
in vivo monitor (BSM2303; Nihon Koden, Tokyo, Japan) were recorded in
the external channel of the fetal ECG monitor via maternal abdominal wall (Monitor 138:
Atom medical) as Apex-Base bipolar lead (Fig.
1).
Indirect ECG monitoring via the maternal abdominal wall
Immediately after the fixation of the needle electrodes for direct monitoring, abdominal
closure was carried out. Thirteen plate electrodes for the indirect ECG monitoring were
fixed on the maternal abdomen. The signals from the indirect leads were recorded in the
Monitor 138 simultaneously.
Accuracy assessment of indirect fetal ECG monitoring
Fetal cardiac electric potential obtained by the direct lead and via the maternal
abdominal wall in the same fetus was obtained in the objective device at a 1,000 Hz
sampling rate for 5 min. The R-squared value between the RR-intervals obtained by the
direct lead and those by the indirect lead of the same fetus was used to determine the
reliability of the clinically developed fetal ECG monitoring system.
Results
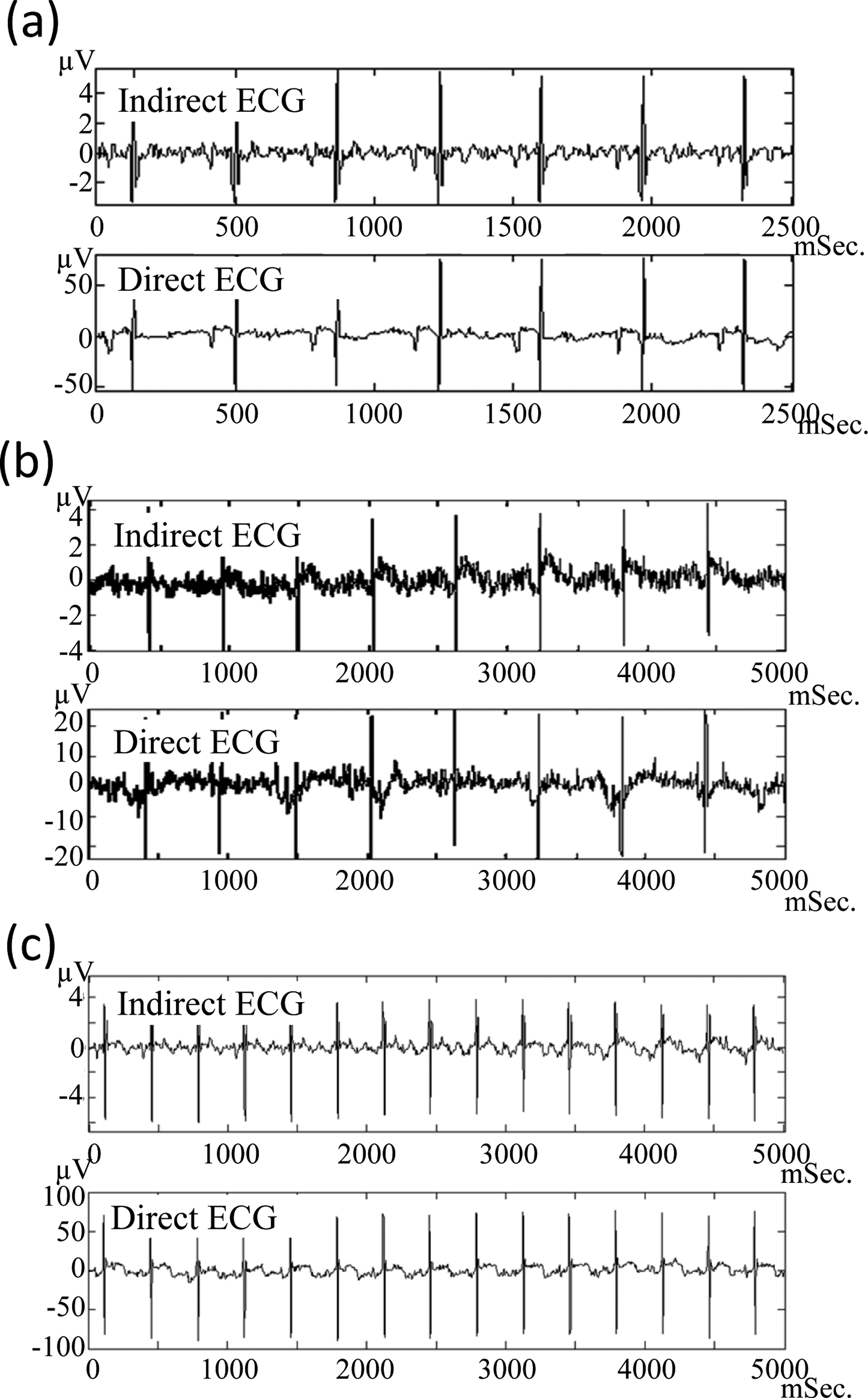
We successfully measured the fetal ECG waveform of pregnant rabbits both with the direct
and indirect monitoring systems, as we could with pregnant mice (Table 1). The maternal abdomen of the pregnant rabbits had enough
space for placing an adequate number of electrodes. Five pregnant rabbits were used in this
study. In three pregnant rabbits, extracted fetal ECG waveforms obtained via the maternal
abdomen wall were observed to be the same as those obtained with the direct lead (Fig. 2). In the other two pregnant rabbits, the fetal
ECG waveforms could be measured by direct lead until the maternal abdomens were closed.
However, the direct lead waveforms could not be extracted after the closure.
Table 1.
Indication of simultaneous measurement
| Fetus ID |
Direct ECG |
Indirect ECG |
R2 value |
| 1 |
Simultaneous fetus waveform extraction |
0.999 |
| 2 |
Measurement failure due to artifacts |
Fetus waveform extraction |
- |
| 3 |
Measurement failure due to artifacts |
Fetus waveform extraction |
- |
| 4 |
Simultaneous fetus waveform extraction |
|
0.997 |
| 5 |
Simultaneous fetus waveform extraction |
|
0.960 |
| Average |
|
|
0.99 |
ECG, electrocardiogram.
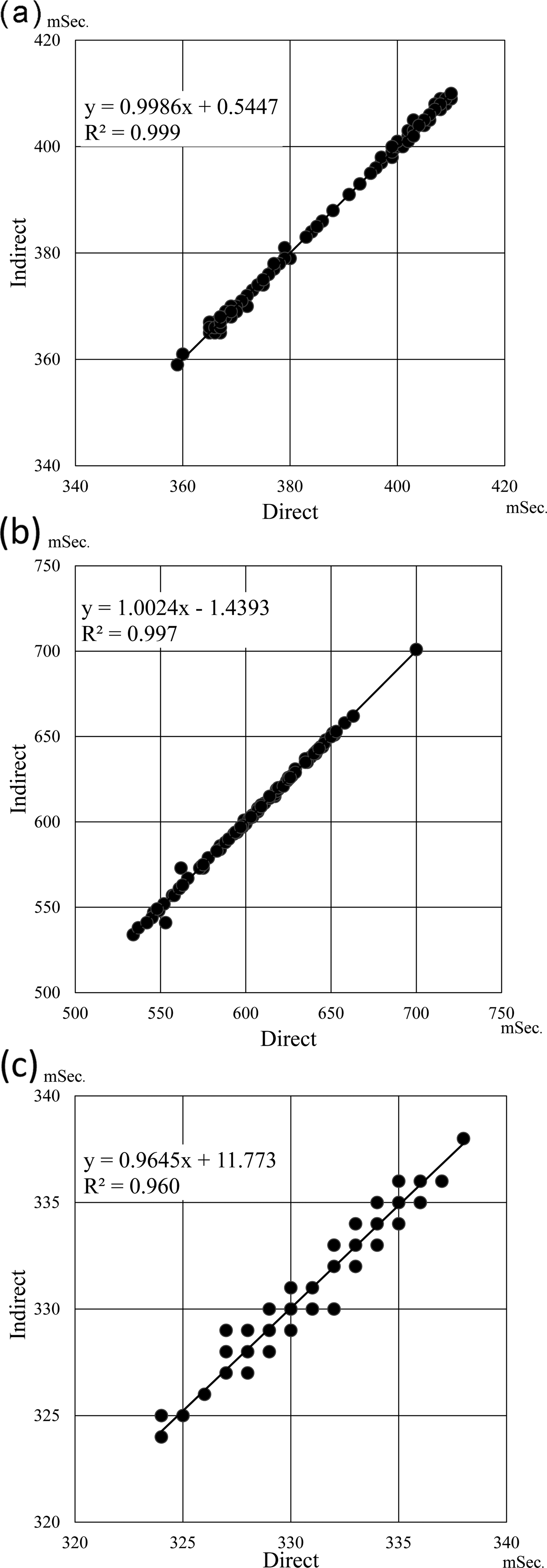
The R-squared value between the RR-intervals obtained by the direct lead and those by the
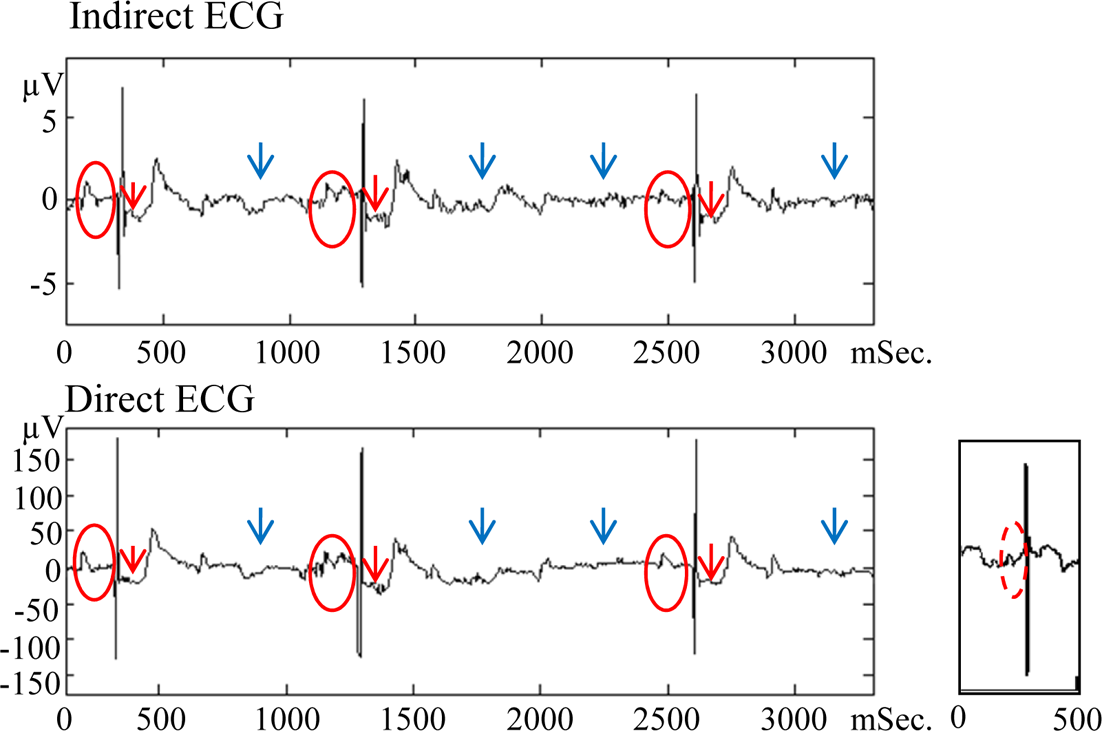
indirect lead of the same fetuses in three pregnant rabbits was 0.99 (Fig. 3). Although one of the three pregnant rabbits presented with an
atrioventricular block during the measurement, fetal ECG waveforms were successfully
extracted from both the direct and indirect lead and showed abnormal characteristics
including elongated PR-interval, ST reduction, and dropped QRS complex (Fig. 4).
Discussion
In 1980, it was attempted to calculate and monitor the fetal heart rate from a fetal ECG
obtained via the maternal abdominal wall [5].
Accordingly, the history of fetal ECG is a history of the development of data processing
technology because the development of fetal ECG continuously utilizes up-to-date
technologies such as signal-averaging, filtering, adaptive filtering, Wiener filtering, and
independent component analysis. However, bandpass filtering causes RR-interval error due to
shape distortion. Adaptive filtering increases signal distortion due to convolution and
noise. Transient high noise levels cause accuracy deterioration of the ECG signal.
However, independent component analysis as a desirable signal extraction method under loud
noise was developed by Jutten et al. in 1991 [6]. Since 2000, more research that shows the application of independent
component analysis to the extraction of fetal ECG waveforms have been reported due to its
applicability in a situation in which the signal-to-noise ratio is less than 1 [7]. However, some difficulties, including the stability of
the fetal ECG extraction, limit the clinical application of this method. Therefore,
researchers are still searching for the technical development for a novel fetal ECG. In one
study, blind source separation with the reference signal (BSSR) is used to stabilize the
independent component analysis [8].
In this study, 13 electrodes could be fixed on the pregnant rabbit abdomens as on the
human’s in clinical setting. Moreover, we demonstrated that fetal ECG waveforms obtained
with indirect leads were accurate as those with direct leads. The average R-squared value
between the RR-intervals obtained by the direct lead and those by the indirect lead with
BSSR of the same fetuses in pregnant rabbits was greater than 0.9, which showed a high
correlation coefficient.
Electrocardiogram measurement of a human fetus requires 13 electrodes to deal with the
fetal movement. In this study using pregnant rabbits, the electrocardiographic waveform of a
fetus could be detected with a pair of electrodes placed near the fetus (Fig. 1). Only a pair of electrodes were needed for the
measurement because there was little chance of fetal movement disturbing the measurement due
to the short periods of measurement, namely 5 min, and the spatial limitation by the
multiple pregnancy. Concomitantly, ECGs of multiple fetuses can be simultaneously measured
if the electrodes are fixed in an appropriate manner.
Mobitz type I atrioventricular block could be diagnosed as the PR-interval gradually
extended and the R wave disappeared eventually (Fig.
4). The cardiotocograph used in the clinical setting cannot classify such fetal
arrhythmias because ultrasound cannot detect the electrical excitation of the myocardium. As
a matter of fact, rabbits are commonly used for reproductive toxicity studies.
Classification of fetal myocardium dysfunctions in rabbits will contributes to the
development of fetal medicine.
Cardiotocograph used in the clinical setting cannot detect the risk of fetal cerebral
hemorrhage [9] because an average of 5 RR-intervals
can be calculated from cardiotocography data. One RR-interval should be obtained to diagnose
fetal malfunction. Although we successfully calculated fetal RR-intervals per every one
heartbeat from indirect fetal ECG in our clinical studies using the same test device used in
this study, it is unknown whether the system can detect the risk of fetal cerebral
hemorrhage [8]. In a mice study, we estimated fetal
autonomic nervous activities, a risk indicator of onset and severe outcome of cerebral
hemorrhage, which is a cause of cerebral palsy, by subtracting fetal RR-intervals obtained
from indirect ECG [3]. This study using rabbits showed
that the ECG system with the indirect lead is reliable as that with the direct lead.
Consequently, this translational research using rabbits shows that the clinical fetal ECG
system using the indirect lead can detect the risk of fetal cerebral hemorrhage as the mouse
fetal ECG system using the direct lead could.
In this study, both direct and indirect fetal ECGs successfully showed abnormal
characteristics. Consequently, fetal malfunction including arrhythmia and cerebral
hemorrhage could be diagnosed using an ECG that acts via the maternal abdominal wall, as in
adults.
Conclusions
The average R-squared value between the RR-intervals obtained by the direct lead and those
by the indirect lead with BSSR of the same fetuses in pregnant rabbits was greater than 0.9,
which showed a high correlation coefficient. Our signal analysis for fetal ECG was
demonstrated to be reliable in this study.
Funding
This work was supported by the Ministry of Education, Culture, Sports, Science and
Technology (MEXT) [Coordination, Support and Training Program for Translational Research;
grant numbers: 1200008]
Acknowledgments
We would like to thank all the members of staff at the institute for animal experimentation
tohoku university graduate school of medicine who took care of animals. We would like to
express my gratitude to Dr. Sachiko HORIE for her generous support.
References
- 1. Cremer,
M.
1906. Ueber die direkte ableitung der aktionsstrome des menschlichen herzens
vom oesophagus und uber das elek- trokardiogramm des fotus. Separatabdruck aus: Münchener
medizinischen Wochenschrif. 17:
811–813.
- 2. Sato,
N., Hoshiai,
T., Ito,
T., Owada,
K.,
Chisaka, H.,
Aoyagi, A.,
Sugawara,
J., Yaegashi,
N.,
Okamura, K.
and Kimura,
Y.
2011. Successful detection of the fetal electrocardiogram
waveform changes during various states of singletons.
Tohoku J. Exp. Med.
225: 89–94.
- 3. Minato,
T., Ito,
T.,
Kasahara,
Y., Ooshio,
S.,
Fushima, T.,
Sekimoto,
A.,
Takahashi,
N., Yaegashi,
N. and
Kimura,
Y.
2018. Relationship between Short term variability (STV) and
onset of cerebral hemorrhage at ischemia–reperfusion load in fetal growth restricted
(FGR) mice. Front. Physiol.
9: 478.
- 4. Morgan, T.
J. and Glowaski,
M. M.
2007. Teaching a new method of rabbit
intubation. J. Am. Assoc. Lab. Anim.
Sci.
46: 32–36.
- 5. Crawford, J.
W.
1986. Limitations of current fetal monitoring
technology. J. Perinat. Med.
14: 379–383.
- 6. Jutten,
C. and
Herault,
J.
1991. Blind separation of sources, part I: An adaptive
algorithm based on neuromimetic architecture. Signal
Process.
24: 1–10.
- 7. Cichocki,
A. and
Amari,
S.
2002. Adaptive Blind Signal and Image Processing. Wiley, New
York.
- 8. Sato,
M., Kimura,
Y., Chida,
S., Ito,
T.,
Katayama,
N., Okamura,
K. and
Nakao,
M.
2007. A novel extraction method of fetal electrocardiogram
from the composite abdominal signal. IEEE Trans. Biomed.
Eng.
54: 49–58.
- 9. Vintzileos, A.
M., Nochimson,
D. J.,
Guzman, E.
R., Knuppel,
R. A.,
Lake, M. and
Schifrin, B.
S.
1995. Intrapartum electronic fetal heart rate monitoring
versus intermittent auscultation: a meta-analysis.
Obstet. Gynecol.
85: 149–155.