Abstract
The purposes of this study are to conduct paleodemographic and paleopathological analyses of medieval human skeletons from Japan and to clarify their life and death situations. The materials used here were individuals from the Yuigahama-chusei-shudan-bochi site (Seika-ichiba location) (i.e. YCSB-SI), located along the Yuigahama seashore of the southern end of Kamakura City. Several new findings regarding the life and death situations of YCSB-SI were obtained: (1) YCSB-SI exhibited a younger age-at-death distribution than other skeletal series; (2) the frequency of caries lesions in YCSB-SI was 5%, females exhibited more caries lesions than males and this group exhibited the lowest caries prevalence rate among Japanese populations; (3) the frequencies of enamel hypoplasia were 67% in the upper central incisors and 73% in the lower canines, which were almost equal to those of non-medieval series; and (4) the presence of weapon-related traumas on the cranium and limb bones from YCSB-SI was demonstrated. It is inferred from the present and previously reported data that population concentration in Kamakura impacted negatively on the lives of the inhabitants, possibly by malnutrition, increase of infectious diseases, and occasionally death by violence, and that all the results can be consistently explained by assuming urbanization and severe living conditions in medieval Kamakura.
Introduction
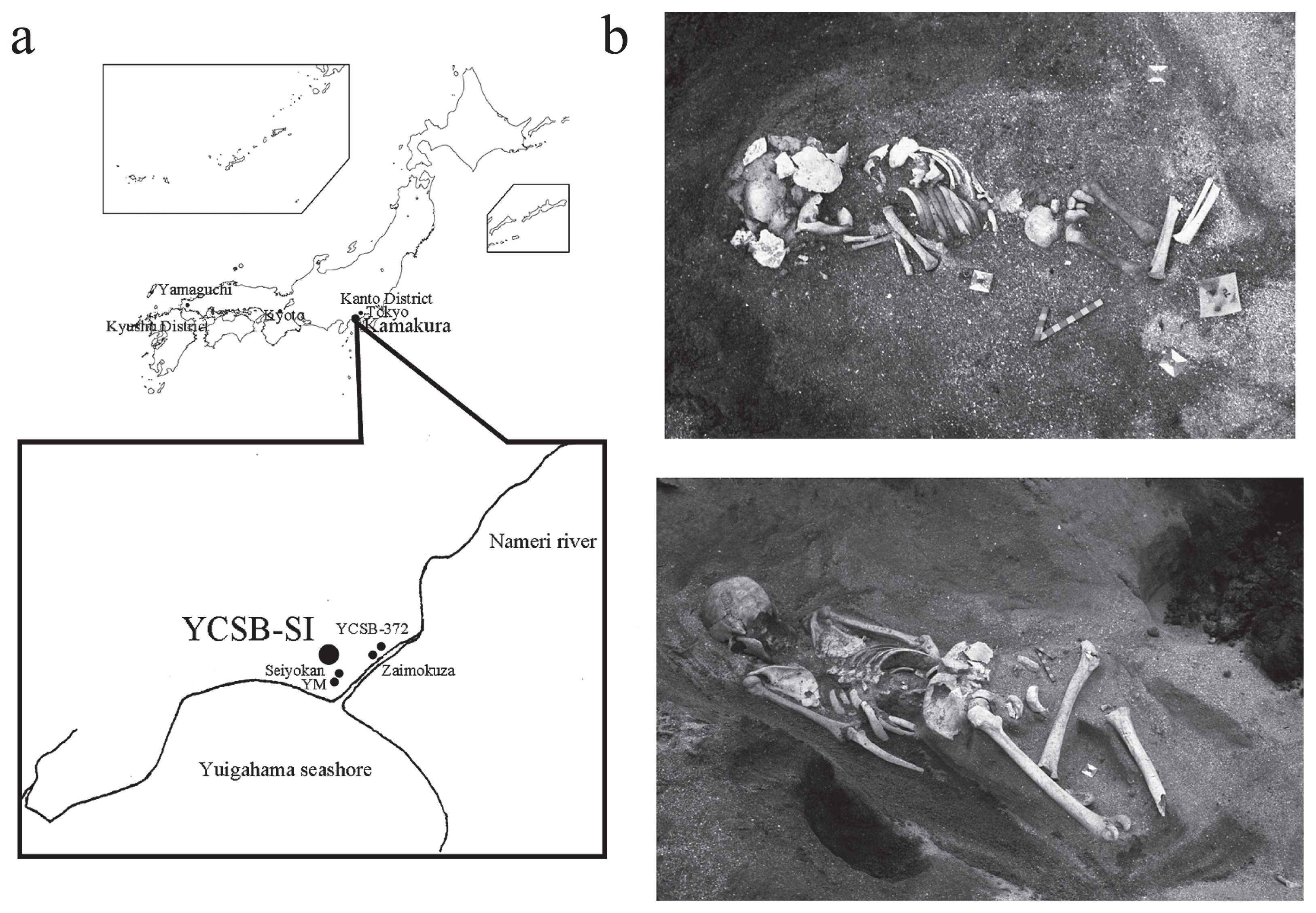
The medieval period of Japan spans nearly 400 years, from 1185 to 1573 AD. This period was characterized by the rise of the warrior class to political power, and the establishment of military governments, and coincides approximately with the period of rules of the Kamakura and Muromachi Shogunates. The first systematic study of medieval Japanese human skeletons was conducted by Suzuki et al. (1956) on 910 skeletal remains from the burial site at Zaimokuza in Kamakura City, the center of a military government in the medieval period (Figure 1). More than half of the skeletons had weapon-related traumas and were considered to be victims of a war that had occurred in 1333 AD.
In recent decades thousands of medieval human skeletons have been excavated from the archaeological sites of Seiyokan, Yuigahama-minami (i.e. YM), and Yuigahama-chusei-shudan-bochi (No. 372 location) (i.e. YCSB-372) in Kamakura (Morimoto et al., 1984; Hirata et al., 2002; Matsushita, 2002; Hirata and Nagaoka, 2005) and there has been remarkable progress both in the studies of Japanese population history and in bioarchaeology. The first author of this paper (T.N.) and colleagues analyzed them and indicated several new findings regarding paleodemography and paleopathology of the medieval Japanese: (1) the paleodemographic study of the YM and YCSB-372 series demonstrated a higher proportion of deaths in young individuals than the Edo period (1603–1867 AD) Japanese and implied severe living conditions in medieval Kamakura due to malnutrition and warfare (Nagaoka et al., 2006; Nagaoka and Hirata, 2008); (2) the paleopathological study of the YM site revealed the first evidence for leprosy and tuberculosis in medieval Japan (Hirata et al., 2011) and less frequent degenerative changes in spines than the Okhotsk and Kumejima skeletal series (Shimoda et al., 2012); and (3) the presence of cut marks on the crania from the Seiyokan, YM, and YCSB-372 sites strongly suggested the prevalence of violence in medieval Japan (Hirata et al., 2004; Nagaoka et al., 2009, 2010). These studies have revealed the life and death situations of the urban inhabitants of medieval Japan from multiple perspectives and a tentative hypothesis is that the medieval people suffered from poor health due to malnutrition and interpersonal violence.
However, the validity of the hypothesis has not been tested and there has not yet been an integrated study of paleodemography and paleopathology focussing on another medieval population. This study applied bioarchaelogical analyses to a new series of human skeletal remains from medieval Kamakura and confirmed whether reproducible results can be obtained from it. The purposes of this study are (1) to observe and describe the human skeletal remains from the Yuigahama-chusei-shudan-bochi site (Seika-ichiba location) (i.e. YCSB-SI) in Kamakura; (2) to estimate the sex and the age at death of each individual and reconstruct the demographic structure; (3) to examine the prevalence and occurrence of dental caries, antemortem tooth loss, and enamel hypoplasia; and (4) to examine weapon-related traumas and describe their morphology, distribution, and frequency.
Materials
The materials used here were individuals from the grave site of YCSB-SI, located along the Yuigahama seashore of the southern end of Kamakura City in Japan, adjacent to the medieval sites of Zaimokuza, Seiyokan, YM, and YCSB-372 (Figure 1). A survey of the YCSB-SI site was undertaken in 1986 by the Kamakura Board of Education and tens of human skeletons were collected. Ohkouchi (1986) published a brief report on the YCSB-SI site and considered that the human skeletons dated back to the 14–15th centuries AD from the pottery sequence and other archaeological remains. Human skeletal remains were dug up by Iwataro Morimoto, professor emeritus at St. Marianna University School of Medicine and have been kept in storage at St. Marianna University, but there has not yet been a bioarchaeological report of them. The social class of the human skeletons can be considered to be commoners, as samurai were generally buried in artificial tombs dug into the rocky cliff sides.
According to Morimoto’s field notes, most of the human skeletons were found in articulated positions, not mixed with the remains of other individuals (Figure 1). The human skeletons housed in St. Marianna University are composed of entire skeletons, whose condition supports the description of Morimoto’s field notes. Although more than thousands of human skeletons have been excavated from several archaeological sites in Kamakura, most of them were mixed with other individuals and individual burials were rare. The human skeletons from the YCSB-SI site allow us to obtain information on paleodemography and the paleopathology of the medieval people, since they can be easily identified as single individuals.
Comparative samples for this study were cited from the literature on paleodemography (Nagaoka et al., 2006, 2012b; Nagaoka and Hirata, 2007, 2008), dental caries (Sakura, 1964; Fujita, 1995; Ohshima, 1996; Todaka et al., 2003), enamel hypoplasia (Sawada, 2010), and violent behavior (Suzuki et al., 1956; Hirata et al., 2004; Nagaoka et al., 2009, 2010; Nagaoka, 2012) (Table 1). The chronological ages used in the comparative samples are the Jomon (14500–300 BC), Yayoi (300 BC–300 AD), medieval (1185–1573 AD), and Edo (1603–1687 AD) periods. The chronological age of the beginning of the Jomon period is cited from Hudson (2009).
Table 1
YCSB-SI and comparative samples used in this study
1 The chronological age of the beginning of the Jomon period is cited from
Hudson (2009).
Methods
Demographic estimates of the sample were conducted under uniformitarian assumption (Weiss, 1973; Howell, 1976; Hoppa, 2002; Chamberlain, 2006).
The sex determination of individuals 15 years of age and older was carried out based on macroscopic assessment of pelvic features (preauricular sulcus, greater sciatic notch, composite arch, inferior pelvis, ischiopubic proportion, ventral arc, subpubic concavity, and medial aspect of the ischiopubic ramus) (Phenice, 1969; Bruzek, 2002) and cranial features (nuchal crest, mastoid process, orbital margin, glabella, and mental eminence) (Walker, 2008).
The age-at-death estimation for subadult skeletons was based on the diaphyseal length of limb bones (Scheuer et al., 1980), the completeness of dental crowns and roots (Moorrees et al., 1963a, b; Ubelaker, 1989), the degree of development and closure of the occipital synchondrosis (Wakebe, 1990), and the degree of ossification and epiphyseal union of the pelvis and long bones (Brothwell, 1981; Krogman and Iscan, 1986). In the case of age at death for adult individuals 15 years of age and older, chronological metamorphosis of the pubic symphysis (Todd, 1920, 1921; Brooks and Suchey, 1990; Sakaue, 2006), and chronological metamorphosis of the auricular surface of the ilium (Lovejoy et al., 1985; Buckberry and Chamberlain, 2002) were used.
This study further analyzed the iliac auricular surfaces of individuals 15 years of age and above and classified them into three age categories, 15–34, 35–54, and ≥55 years using the method of Buckberry and Chamberlain (2002) and the Bayesian theorem. The contingency tables of age and Buckberry and Chamberlain’s auricular surface stage for Japanese reference samples (Nagaoka et al., 2012b) were used to calculate the posterior probability of being a particular age conditional on being in a particular state of an age indicator. The prior probabilities used in the calculation are uniform ones, where an equal prior probability is assigned to each age category, because in this assumption the estimated age-at-death distribution of the target sample is independent of that of the reference one (Nagaoka et al., 2012a).
Observation of antemortem toot loss (AMTL) was conducted using the naked eye to assess complete absorption of dental sockets. The percentage of AMTL was calculated by dividing the number of AMTL by the sum of the number of teeth, dental sockets, and AMTL. Observation of caries lesions was conducted using the naked eye and dental instruments. Color changes in enamel without depression were excluded, because they are difficult to judge as caries lesions. The percentage of carious teeth was calculated by dividing the number of carious teeth by the number of examined teeth. Although the frequencies of AMTL and caries lesions increase with age, this study did not calculate age-specific frequencies due to the small sample size.
The frequencies of enamel hypoplasia were examined to clarify the physical condition during infancy and childhood. According to Hillson (1996), deficiencies of enamel thickness such as horizontal furrows and pits on tooth surface were identified as enamel hypoplasia. The presence or absence of hypoplasia in the upper first incisors (UI1) and lower canines (LC) that had more than half of intact crown height were recorded. Each tooth was observed macroscopically and using a 10× magnifying lens under an LED light (Panasonic, BF-425).
Unhealed cut marks by edged weapons were identified by the methods of Walker and Long (1977) and Lewis (2008). The macroscopic profile of cut marks made by stone or steel tools is V-shaped in cross section (Walker and Long, 1977). Knives always produce V-shaped profiles in cross-section without flaking of the cut mark walls, while Japanese swords produce cut marks that yield a unilateral flaking of the cut mark walls and exhibit a long, narrow, and elliptical shape from a superior view (Lewis, 2008).
Enamel hypoplasia was observed by the second author (J.S.) and all other observations were conducted by the first author (T.N.). Because the data used in the present and comparative samples were in general collected by the same observers using the same methods, the interobserver errors between them are negligible. However, the cut-mark data by Suzuki et al. (1956) and the caries-lesion data by Fujita (1995), Ohshima (1996), and Todaka et al. (2003), used for comparison, should be considered carefully, because inter-observer errors between the present and comparative data may be expected.
Results
Sex determination and age-at-death estimation
The sex and age-at-death composition of the skeletal remains of the YCSB-SI are summarized in Table 2. The sexual ratio of 16 males to 15 females indicates a skeletal population that was not sexually biased. The number of individuals is 51, which consists of 13 subadult skeletons, 28 adult skeletons, and 10 of unknown age.
Table 2
Age and sex composition of the YCSB-SI human skeletons
| Age in years |
Sex |
| Male |
Female |
Unknown |
Total |
| Subadult |
| 0–4 |
|
|
3 |
3 |
| 5–9 |
|
|
3 |
3 |
| 10–14 |
|
|
1 |
1 |
| 15–19 |
1 |
|
1 |
2 |
| Indeterminable subadult |
|
1 |
3 |
4 |
| Adult |
| 20–39 |
9 |
3 |
|
12 |
| 40+ |
2 |
7 |
|
9 |
| Indeterminable adult |
2 |
3 |
2 |
7 |
| Unknown |
2 |
1 |
7 |
10 |
| Total |
16 |
15 |
18 |
51 |
Table 3 shows the proportion of individuals classified into subadults and adults and compares it with the YCSB-SI and other series. In the YCSB-SI, 32% of the sample died before 20 years and the ratio of 13 subadults to 28 adults was 0.46. The proportion of deaths in subadults in YCSB-SI (32%, 13/41) is significantly less than that in Edo (56%, 116/207) (P < 0.01), but showed no significant difference with that in YCSB-372 (18%, 34/188) and YM (38%, 98/260) (P > 0.05). It is safe to say that the preservation and sampling bias are equal among medieval populations.
Table 3
Proportion of individuals classified into subadults and adults from the YCSB-SI and comparative samples
| Population |
Locality |
Period |
0–19 years |
20+ years |
Difference1 |
| Number of individuals |
Proportion of deaths |
Number of individuals |
Proportion of deaths |
| YCSB-SI |
Kamakura |
Medieval |
13 |
0.32 |
28 |
0.68 |
|
| YCSB-372 (Nagaoka and Hirata, 2008) |
Kamakura |
Medieval |
34 |
0.18 |
154 |
0.82 |
ns |
| YM (Nagaoka et al., 2006a) |
Kamakura |
Medieval |
98 |
0.38 |
162 |
0.62 |
ns |
| Edo (Nagaoka and Hirata, 2007, 2008) |
Tokyo |
Edo |
116 |
0.56 |
91 |
0.44 |
** |
1 Fisher’s exact test between YCSB-SI and comparative samples. ns: not significant;
Table 4 shows the number of individuals of each of Buckberry and Chamberlain’s stages of the auricular surface. The distribution among the seven indicator stages of individuals is, in order, 0, 4, 2, 4, 5, 0, and 0. Based on the distributions among the stages, we reconstructed the age-at-death distribution of individuals aged 15 years and above and obtained the result that the proportion of deaths in the 15–34, 35–54, and ≥55 year groups accounted for 50% (7.5/15), 33% (4.9/15), and 17% (2.6/15), respectively (Figure 2, Table 5). Although there is no significant difference between the present and comparative data in the number of individuals of each of Buckberry and Chamberlain’s stages of the auricular surface (P > 0.05) (Table 4), a comparison of these demographic profiles demonstrated similarities among the medieval and Jomon series and dissimilarities among the medieval and Edo-period series (Figure 2, Table 5). That is, the medieval and Jomon series tended to yield younger age distributions than the Edo-period series (Figure 2, Table 5).
Table 4
Number of individuals in each stage for the auricular surface from the YCSB-SI and comparative samples
1 Fisher’s exact test between YCSB-SI and comparative samples. ns: not significant.

Table 5
Comparison of the age-at-death structure aged 15 years and above among the YCSB-SI and comparative samples
| Population |
Locality |
Period |
|
Age in years |
| 15–34 |
35–54 |
55+ |
| YCSB-SI |
Kamakura |
Medieval |
Number of individuals |
7.5 |
4.9 |
2.6 |
|
|
|
Proportion of deaths |
0.50 |
0.33 |
0.17 |
| YCSB-372 (Nagaoka and Hirata, 2008) |
Kamakura |
Medieval |
Number of individuals |
53.0 |
34.6 |
26.5 |
|
|
|
Proportion of deaths |
0.46 |
0.30 |
0.23 |
| Jomon (Nagaoka et al., 2008, 2012b) |
All Japan |
Jomon |
Number of individuals |
43.3 |
22.6 |
22.1 |
|
|
|
Proportion of deaths |
0.48 |
0.26 |
0.26 |
| Edo (Nagaoka and Hirata, 2007, 2008) |
Tokyo |
Edo |
Number of individuals |
35.7 |
34.2 |
29.1 |
|
|
|
Proportion of deaths |
0.36 |
0.35 |
0.29 |
A paleopathological examination revealed the presence of cribra orbitalia, periostitis, caries lesions, AMTL, abscess cavity, and enamel hypoplasia in the YCSB-SI series (Figure 3). Here, we examined AMTL, caries lesions, and enamel hypoplasia in detail because the other cases provide only fragmentary evidence, and do not allow us to depict any pathological characteristics in the YCSB-SI series.
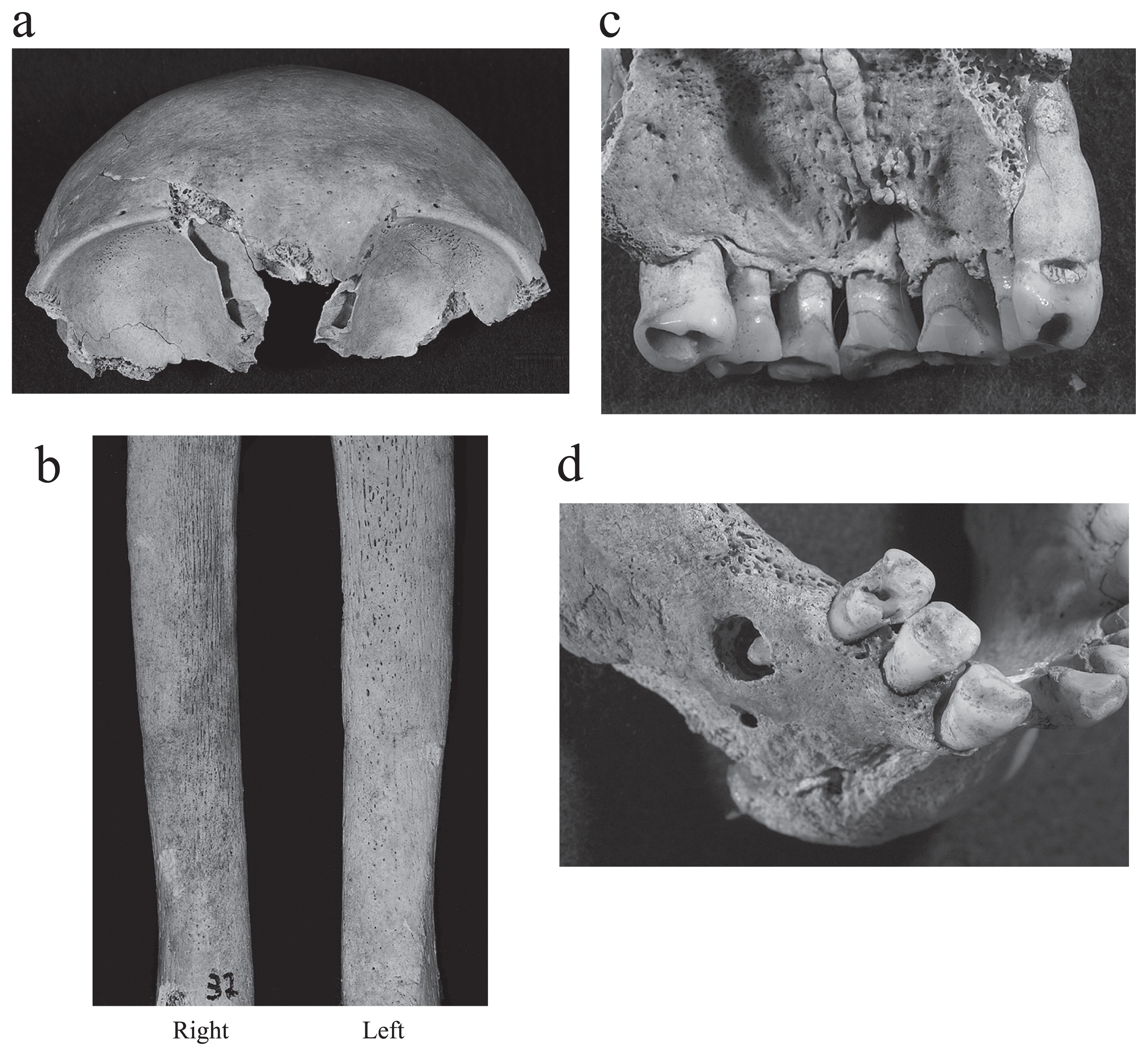
Table 6 shows the frequencies of AMTL and caries lesions in each jaw of YCSB-SI. The frequency of AMTL in the lower teeth was significantly higher in females (15%, 12/82) than in males (3%, 5/152) (P < 0.01) (Table 6, Appendix 1). The frequency of caries lesions in the lower teeth was significantly higher in females (8%, 5/62) than in males (1%, 1/142) (P < 0.05), and that in both the upper and lower teeth was also significantly higher in females (8%, 14/167) than in males (3%, 20/216) (P < 0.05) (Table 6, Appendix 1). Caries lesions were concentrated on premolars and molars and the frequent sites of caries lesions were approximal surfaces and entire crowns (Table 7). YCSB-SI exhibited significantly lower caries-lesion frequency (5%, 24/475) than the Jomon, Yayoi, Muromachi, and Edo series (P < 0.05 or P < 0.01), while the caries-lesion frequency in YCSB-SI is equivalent to that in Zaimokuza (6%, 147/2669) of the same period (P > 0.05) (Table 8). The frequencies of enamel hypoplasia of YCSB-SI were 67% (16/24) in UI1 and 73% (11/15) in LC (Table 9). There are no significant sexual differences in UI1 and LC (P < 0.05). The frequency of hypoplasia in LC of YCSB-SI was significantly lower than that of Jomon (92%, 156/169), although there were no significant differences in UI1 among the YCSB-S, Jomon, Yayoi and Edo series, and in LC among the YCSB-S, Yayoi and Edo series.
Table 6
Comparison of AMTL and dental caries between sexes of the YCSB-SI sample
| Sex |
Maxilla |
Male vs. female1 |
Mandible |
Male vs. female1 |
Maxilla + mandible |
Male vs. female1 |
| Observable |
AMTL |
AMTL frequency |
Observable |
AMTL |
AMTL frequency |
Observable |
AMTL |
AMTL frequency |
| Male |
182 |
11 |
0.06 |
|
152 |
5 |
0.03 |
|
334 |
16 |
0.05 |
|
| Female |
134 |
8 |
0.06 |
ns |
82 |
12 |
0.15 |
** |
216 |
20 |
0.09 |
ns |
| Male + female |
316 |
19 |
0.06 |
|
234 |
17 |
0.07 |
|
550 |
36 |
0.07 |
|
| Sex |
Maxilla |
Male vs. female1 |
Mandible |
Male vs. female1 |
Maxilla + mandible |
Male vs. female1 |
| Observable |
Caries |
Caries frequency |
Observable |
Caries |
Caries frequency |
Observable |
Caries |
Caries frequency |
| Male |
164 |
9 |
0.05 |
|
142 |
1 |
0.01 |
|
306 |
10 |
0.03 |
|
| Female |
107 |
9 |
0.08 |
ns |
62 |
5 |
0.08 |
* |
169 |
14 |
0.08 |
* |
| Male + female |
271 |
18 |
0.07 |
|
204 |
6 |
0.03 |
|
475 |
24 |
0.05 |
|
AMTL: antemortem tooth loss.
1 Fisher’s exact test between sexes: ns: not significant;
Table 7
Location of caries lesions of the YCSB-SI sample
| Position |
Maxilla and mandible |
| I1 |
I2 |
C |
P3 |
P4 |
M1 |
M2 |
M3 |
Total |
Frequency |
| Male |
| Occlusal |
0 |
0 |
0 |
0 |
1 |
0 |
0 |
1 |
2 |
0.20 |
| Approximal |
0 |
0 |
0 |
2 |
0 |
0 |
3 |
0 |
5 |
0.50 |
| Buccolingal |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0.00 |
| Plural surfaces |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0.00 |
| Entire crown |
0 |
0 |
0 |
1 |
1 |
1 |
0 |
0 |
3 |
0.30 |
| Root |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0.00 |
| Female |
| Occlusal |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
1 |
2 |
0.14 |
| Approximal |
0 |
0 |
1 |
0 |
1 |
2 |
1 |
0 |
5 |
0.36 |
| Buccolingal |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0.00 |
| Plural surfaces |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0.00 |
| Entire crown |
0 |
0 |
2 |
1 |
1 |
1 |
1 |
1 |
7 |
0.50 |
| Root |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0.00 |
Table 8
Comparison of frequency of dental caries among the YCSB-SI and comparative samples
1 Fisher’s exact test between YCSB-SI and comparative samples. ns: not significant;
Table 9
Comparison of frequency of enamel hypoplasia among the YCSB-SI and comparative samples
| Population |
Locality |
Period |
Sex |
UI1 |
Difference1,2 |
LC |
Difference 1,2 |
| Number of teeth |
Number of teeth affected |
Hypoplasia frequency |
Number of teeth |
Number of teeth affected |
Hypoplasia frequency |
| YCSB-SI |
Kamakura |
Medieval |
Male |
11 |
6 |
0.55 |
|
7 |
5 |
0.71 |
|
|
|
|
Female |
6 |
5 |
0.83 |
ns1 |
4 |
2 |
0.50 |
ns1 |
|
|
|
Unknown |
7 |
5 |
0.71 |
|
4 |
4 |
1.00 |
|
|
|
|
Total |
24 |
16 |
0.67 |
|
15 |
11 |
0.73 |
|
| Jomon (Sawada, 2010) |
All Japan |
Jomon |
Total |
147 |
114 |
0.78 |
ns2 |
169 |
156 |
0.92 |
*2 |
| Yayoi (Sawada, 2010) |
North Kyushu-Yamaguchi |
Yayoi |
Total |
157 |
106 |
0.68 |
ns2 |
187 |
144 |
0.77 |
ns2 |
| Edo (Sawada, 2010) |
Tokyo |
Edo |
Total |
45 |
26 |
0.58 |
ns2 |
55 |
46 |
0.84 |
ns2 |
1 Fisher’s exact test between sexes. ns: not significant.
2 Fisher’s exact test between YCSB-SI and comparative samples. ns: not significant;
One adult male and one adult female between them exhibited 12 weapon-related traumas in the YCSB-SI series.
The first case is individual No. 1852, an adult female. The entire skeleton is preserved. The individual exhibited one sharp-force trauma on the right parietal bone (Figure 4, Appendix 2). The cut was oriented from the medial anterior to the lateral posterior and entered into the diploe with flat and smooth cut surfaces. The cut produced a unilateral flaking of cut surfaces, which is consistent with the diagnostic criteria of sharp-force traumas made by Japanese swords. This specimen did not exhibit any color difference between modified and original bone surfaces, suggesting that it was not recent damage to the cranium. The lack of signs of healing indicates that the individual’s cranium was cut either immediately prior to death or in the postmortem period.
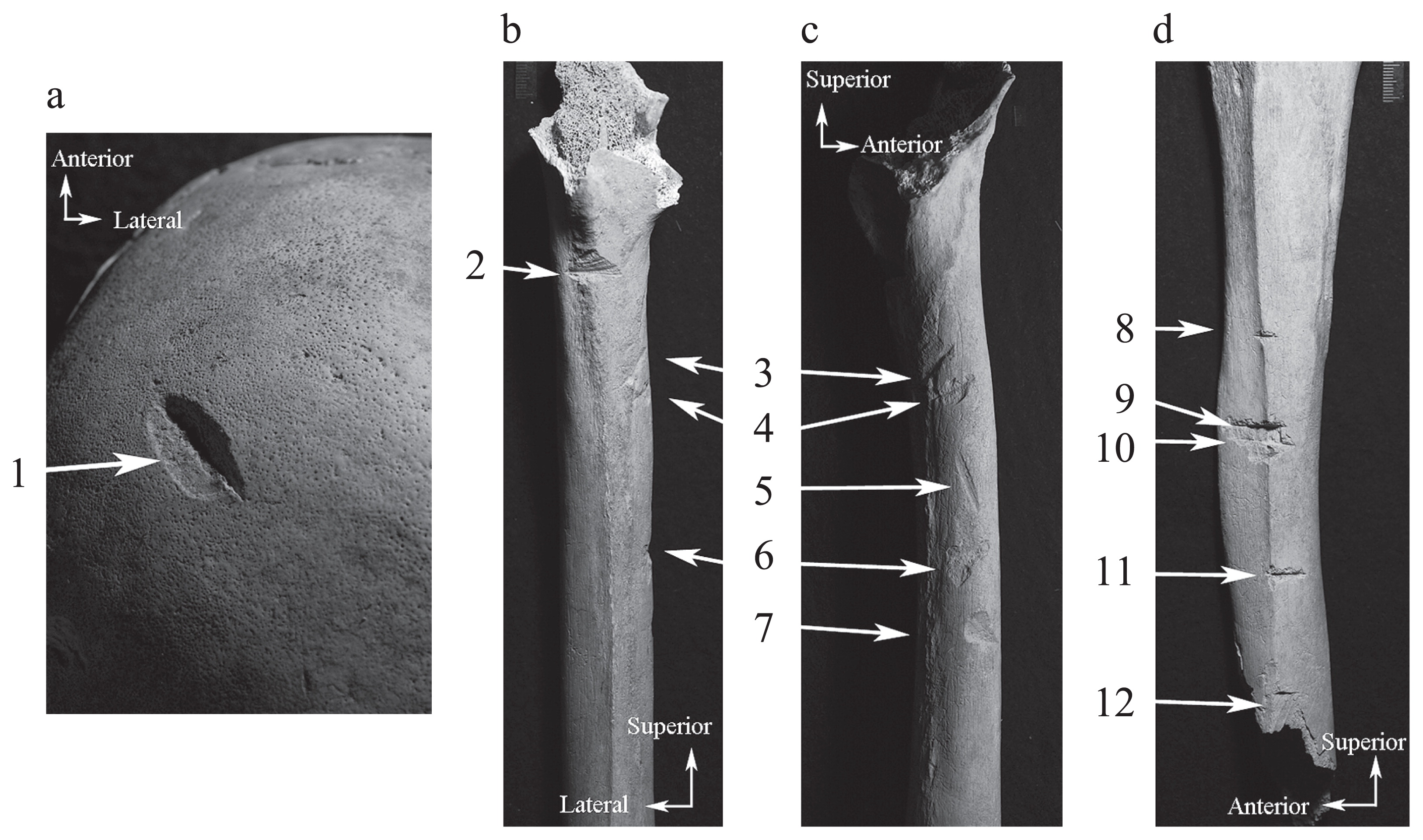
The second case is individual No. 1766, an adult male. The entire skeleton is preserved. The individual exhibited six sharp-force traumas on the left femur and five sharp-force ones on the left tibia (Figure 4, Appendix 2). The former were concentrated on the medial surface of the femoral body in the depth of the cortical bone and the latter were concentrated on the interosseous border of the left tibia in the depth of the cortical bone. They all left flat and smooth cut surfaces. The lack of signs of healing indicates that the individual was cut either immediately prior to death or in the postmortem period.
The frequency of individuals with a cranial trauma was 2% out of 51 individuals, which is significantly lower than that of Zaimokuza (P < 0.01), but there is no significant difference among the YCSB-SI and other skeletal series (P > 0.05) (Table 12). The frequency of individuals with postcranial traumas was 2% out of 51 and there is no significant difference between YCSB-SI and YM (P > 0.05) (Table 10). YCSB-SI and other medieval crania exhibited traumas predominantly on the parietal bones, while in Edo traumas were less frequently observed on the parietal bones (Table 11). The traumas were observed equally on both sexes, which is consistent with the circumferences of the medieval series, while in Edo the traumas were observed solely on adult males (Table 12).
Table 10
Fisher’s exact test of cut-mark frequency among the YCSB-SI and comparative samples
1 Fisher’s exact test between YCSB-SI and comparative samples. ns: not significant;
Table 11
Comparison of location of cranial cut marks among the YCSB-SI and comparative samples
| Population |
Locality |
Period |
Number and frequency of cut marks |
| ZYG |
NAS |
MAX |
FRO |
PAR |
TEM |
OCC |
| YCSB-SI |
Kamakura |
Medieval |
0 (0.00) |
0 (0.00) |
0 (0.00) |
0 (0.00) |
1 (1.00) |
0 (0.00) |
0 (0.00) |
| YCSB-372 (Nagaoka et al., 2009) |
Kamakura |
Medieval |
0 (0.00) |
0 (0.00) |
0 (0.00) |
3 (0.19) |
11 (0.69) |
0 (0.00) |
2 (0.13) |
| YM (Hirata et al., 2004) |
Kamakura |
Medieval |
0 (0.00) |
0 (0.00) |
0 (0.00) |
7 (0.44) |
8 (0.50) |
0 (0.00) |
1 (0.06) |
| Seiyokan (Nagaoka et al., 2010) |
Kamakura |
Medieval |
1 (0.04) |
2 (0.08) |
1 (0.04) |
2 (0.08) |
12 (0.48) |
3 (0.12) |
4 (0.16) |
| Edo (Nagaoka, 2012) |
Tokyo |
Edo |
1 (0.10) |
0 (0.00) |
0 (0.00) |
0 (0.00) |
3 (0.30) |
2 (0.20) |
4 (0.40) |
ZYG, zygomatic bone; NAS, nasal bone; MAX, maxilla; FRO, frontal bone; PAR, parietal bone; TEM, temporal bone; OCC, occipital bone. When the number of cut marks on each bone was recorded, a continuous cut mark on two bones or more was separately counted.
Table 12
Comparison of age and sex composition of individuals with cut marks among the YCSB-SI and comparative samples
| Population |
Locality |
Period |
Number and frequency of individuals with cut marks |
| Subadult |
Adult |
Unkown age |
| Male |
Female |
Unknown sex |
| YCSB-SI |
Kamakura |
Medieval |
0 (0.00) |
1 (0.50) |
1 (0.50) |
0 (0.00) |
0 (0.00) |
| YCSB-372 (Nagaoka et al., 2009) |
Kamakura |
Medieval |
1 (0.13) |
3 (0.38) |
1 (0.13) |
0 (0.00) |
3 (0.38) |
| YM (Hirata et al., 2004) |
Kamakura |
Medieval |
0 (0.00) |
2 (0.50) |
2 (0.50) |
0 (0.00) |
0 (0.00) |
| Seiyokan (Nagaoka et al., 2010) |
Kamakura |
Medieval |
0 (0.00) |
3 (0.50) |
1 (0.17) |
1 (0.17) |
1 (0.17) |
| Edo (Nagaoka, 2012) |
Tokyo |
Edo |
0 (0.00) |
2 (1.00) |
0 (0.00) |
0 (0.00) |
0 (0.00) |
Discussion
This study indicated several findings regarding the paleodemography and paleopathology of YCSB-SI. (1) YCSB-SI yielded a younger age-at-death distribution than other skeletal series, in particular Edo. (2) The frequency of caries lesions in YCSB-SI was 5% and females exhibited more caries lesions than males. YCSB-SI exhibited the lowest caries prevalence rate among Japanese populations. (3) The frequency of AMTL in YCSB-SI was 7% and females exhibited more AMTL than males. (4) The frequencies of enamel hypoplasia of YCSB-SI were 67% in UI1 and 73% in LC, which were almost equal to those of the Yayoi and Edo series. (5) The presence of weapon-related traumas on the cranium and limb bones from YCSB-SI was demonstrated. The most important question is whether these findings are consistent with the assumption that the medieval people were in a poor health and experienced difficult lives.
Paleodemography
The reconstruction of age-at-death distribution of human skeletal remains has a persistent problem in terms of the validity of adult age estimation techniques (Bocquet-Appel and Masset, 1982, 1985, 1996; Buikstra and Konigsberg, 1985; Horowitz et al., 1988; Mensforth, 1990; Konigsberg and Frankenberg, 1992). The analyses of an archaeological sample from different places and times have similarly resulted in the concentration of deaths between 25 and 45 years and the lack of elderly individuals over the age of 60 years, which differs from the distribution recorded in historical documents or model life tables due to the methodological problem (Weiss, 1973; Howell, 1982; Chamberlain, 2006; Storey, 2007). Paleodemographers have sought solutions to overcome the difficult problem of age-at-death estimation and a consensus on procedures for estimating age at death from a skeletal sample, the ‘Rostock Manifesto,’ advocated using the Bayesian theorem to provide a methodological basis for adult aging techniques (Hoppa, 2002). Nagaoka et al. (2012b) estimated the age-at-death distribution of the human skeletal remains associated with the Okhotsk culture using the Buckberry–Chamberlain system of auricular surface aging and the Bayesian approach, and obtained an appropriate mortality profile of the prehistoric hunter-gatherers with a high proportion of elderly individuals. Based on the methods and reference sample employed by Nagaoka et al. (2012b), this study estimated the age-at-death distributions of YCSB-SI and comparative samples. The distributions obtained here exhibit a high proportion of elderly individuals (17–29%), which is likely to be plausible, since these distributions do not depart from the realistic demographic structures of preindustrialized societies in historical or ethnological records (Kobayashi, 1956; Weiss, 1973; Howell, 1979; Kito, 2000). Comparison of these demographic profiles further demonstrated younger age-at-death distributions in the medieval series than in the Edo-period series. This result is consistent with the result of Nagaoka et al. (2006) that life expectancy changed little over the thousands of years between the Jomon and medieval periods but improved during the few hundred years between the medieval and Edo periods. Even though this study and Nagaoka et al. (2006) used different aging methods, they commonly obtained the short-lived tendency of medieval people.
Nagaoka et al. (2006) compared the urban sanitation situation between the medieval and Edo populations and considered that population concentration in medieval Kamakura had impacted negatively on the lives of the inhabitants. Urban sanitation of the water supply and waste disposal was not provided there and the observation of injured skeletons by Nagaoka et al. (2009, 2010) implied the possibility that some of the medieval Japanese individuals were drawn into direct or indirect involvement in violence and warfare. In Edo-period Japan also, the mortality rate was higher in urban areas than in rural areas (Kito, 2000). There were repeated epidemics of measles, influenza, dysentery, smallpox, beriberi, typhoid, cholera, syphilis, enteritis, and diarrhea among the inhabitants of Edo at that time (Fujikawa, 1969). Previous studies of cribra orbitalia and enamel hypoplasia in Edo (Yamamoto, 1988; Hirata, 1990) demonstrated stressful living conditions in the city of Edo due to nutritional deficiency and population concentration. Despite these conditions, the level of urban sanitation in Edo-period Japan surpassed that of the West, both in terms of water supply and waste disposal (Hanley, 1997). Clean drinking water was constantly supplied from the Tamagawa and Kanda aqueducts in Edo City and excrement was recycled into manure for agricultural use (Hanley, 1997). Customs concerning hygiene, food and drink, combined with a lack of domestic animals, suggest that living conditions in Edo were more sanitary than in the West (Hanley, 1997). Historical demographers consider that conditions of diet, clothes, houses, bathing, and urban sanitation improved drastically within the Edo period and that these changes led to the increase in life expectancy (Hanley, 1997; Kito, 2000). Although the population concentration in the city of Edo had impacted negatively on the lives of the inhabitants, a comparison between Kamakura and Edo suggests that the time between the medieval and Edo periods corresponded not only to a span of extension of life expectancy but also to a period of improvement in urban living conditions. It is reasonable to consider that population concentration in Kamakura led to more stressful circumferences than in Edo, possibly by unsanitary living conditions, malnutrition, and occasionally death by violence and warfare.
Caries lesions and AMTL
YCSB-SI exhibited the lowest frequencies of caries lesions among Japanese populations from the Jomon to Edo periods. Although comparative data were collected from a range of literatures, the lowest frequencies of caries lesions were consistently obtained both in YCSB-SI and Zaimokuza (Table 8). Dental caries prevalence has often been related to subsistence in archaeological contexts. The adoption of agriculture reduced oral health and increased caries prevalence (e.g. Lukacs, 1992; Larsen, 1997), and moreover in Japan the caries prevalence rate is higher among Yayoi agriculturists than Jomon hunter-gatherers (e.g. Oyamada et al., 1996; Todaka et al., 2003). The lowest prevalence rate in caries lesions in YCSB-SI can be explained by two things: the dietary habits of the medieval period were different from those of other periods, including Jomon and Yayoi; or, because caries lesions usually increase with age, the young age distribution of YCSB-SI led to the low caries rate. The archaeological remains from medieval Kamakura indicated that the medieval people had consumed, among other things, rice, nuts, millet, soybeans, fruit, meat, and fish, and had cooked them using kitchen knives, kettles, pans, and mortars (Kawano, 1995), and Japanese food history also implies that the food ingredients employed by commoners in the medieval period were almost the same as those of historic Japan (see Sakura, 1964). They did not lead to subsistence change in the medieval period. Together with the paleodemographic results, the latter explanation is more plausible than the former.
Another finding is sexual differences in caries lesions and AMTL: females exhibited higher prevalence rates of both than males. Irei et al. (2008) found a higher caries prevalence in females than in males in the Edo-period human skeletons from Kumejima Island (Okinawa, Japan) and explained it by the different dietary habits between sexes which had been implied by Yoneda et al. (2004). That is, C3 plants or carbohydrates were consumed mainly by females, while fish or proteins were consumed mainly by males. High caries prevalence in females has been reported in modern and ancient human populations and has been usually explained by cultural factors (e.g. easy access to foods during food preparation) and biological ones (e.g. early eruption of permanent teeth in females and pregnancy) (Lukacs and Largaespada, 2006). If this explanation is the case here, the high caries prevalence in females in YCSB-SI is a culturally and biologically significant finding.
Enamel hypoplasia
Enamel hypoplasia is defined as developmental dental enamel defects induced by metabolic stresses from nutritional disorders or diseases during the enamel formation period (e.g. Goodman and Rose, 1990; Hillson, 1996). These defects are a good indicator of the childhood health status of the ancient human skeletons (Goodman et al., 1980; Duray, 1996; Starling and Stock, 2007; Oyamada et al., 2012). The previous study by Yamamoto (1988) suggested that Edo exhibited the highest frequencies of enamel hypoplasia among Japanese populations and concluded that the Edo people lived under stressful environments such as population concentration and infectious diseases. However, Yamamoto’s (1988) sample size of the medieval people is only five upper central incisors and three lower canines and the comparison between the medieval and Edo-period series had not been sufficiently conducted. Contrary to Yamamoto (1988), the frequencies of enamel hypoplasia in YCSB-SI were almost equal to those of the Yayoi and Edo series. It is safe to consider, with the current data, that there was not so much of a difference in the severity of living conditions between YCSB-SI and Edo and that the living conditions in Edo are not necessarily worse than those in YCSB-SI.
Weapon-related traumas
Several preceding studies have shown that human skeletons from medieval Japan exhibited traumatic injuries related to violence, such as gashes, decapitations, blows, stabbing, and scratches (Suzuki et al., 1956; Morimoto, 1987; Morimoto and Hirata, 1992; Hirata et al., 2004; Nagaoka et al., 2009, 2010). The results of this study demonstrated the presence of weapon-related traumas on the cranium and limb bones. The traumatic injuries found in YCSB-SI, which exhibited similarity to those of other medieval series with regard to morphology and distribution, strongly suggest the prevalence of violence in the medieval period. This is consistent with the historical background that the rise to political power of the warrior class and the establishment of a military government resulted in continuous disturbances, armed conflicts, and violent death, and also the severe living conditions implied by the paleodemographic and paleopathological findings.
The frequency of weapon-related trauma in crania was significantly lower in YCSB-SI than in Zaimokuza, although there was no significant difference among the YCSB-SI and other skeletal series. Most of the cranial traumas in the Zaimokuza were scratch marks, which have been rarely observed in other medieval sites in Kamakura (Hirata et al., 2004; Nagaoka et al., 2009, 2010). An exceptionally high rate of weapon-related traumas in the Zaimokuza has been pointed out by Hirata et al. (2004) and Nagaoka et al. (2009) and has been explained as follows:
“Suzuki’s examination of scratches did not distinguish between cut marks and other confounding factors. As well as the [YCSB-372] sample, the Zaimokuza sample was possibly subjected to postmortem abrasion before burial which yielded features similar to cut marks or eliminated the original features of cut marks. It is reasonable to assume that taphonomic processes led to overestimation of the percentage of scratches of the Zaimokuza sample” (Nagaoka et al., 2009: 178).
With the current data available, it is difficult to give cultural or biological meaning to the significant difference in cut-mark frequencies between YCSB-SI and Zaimokuza.
Conclusions
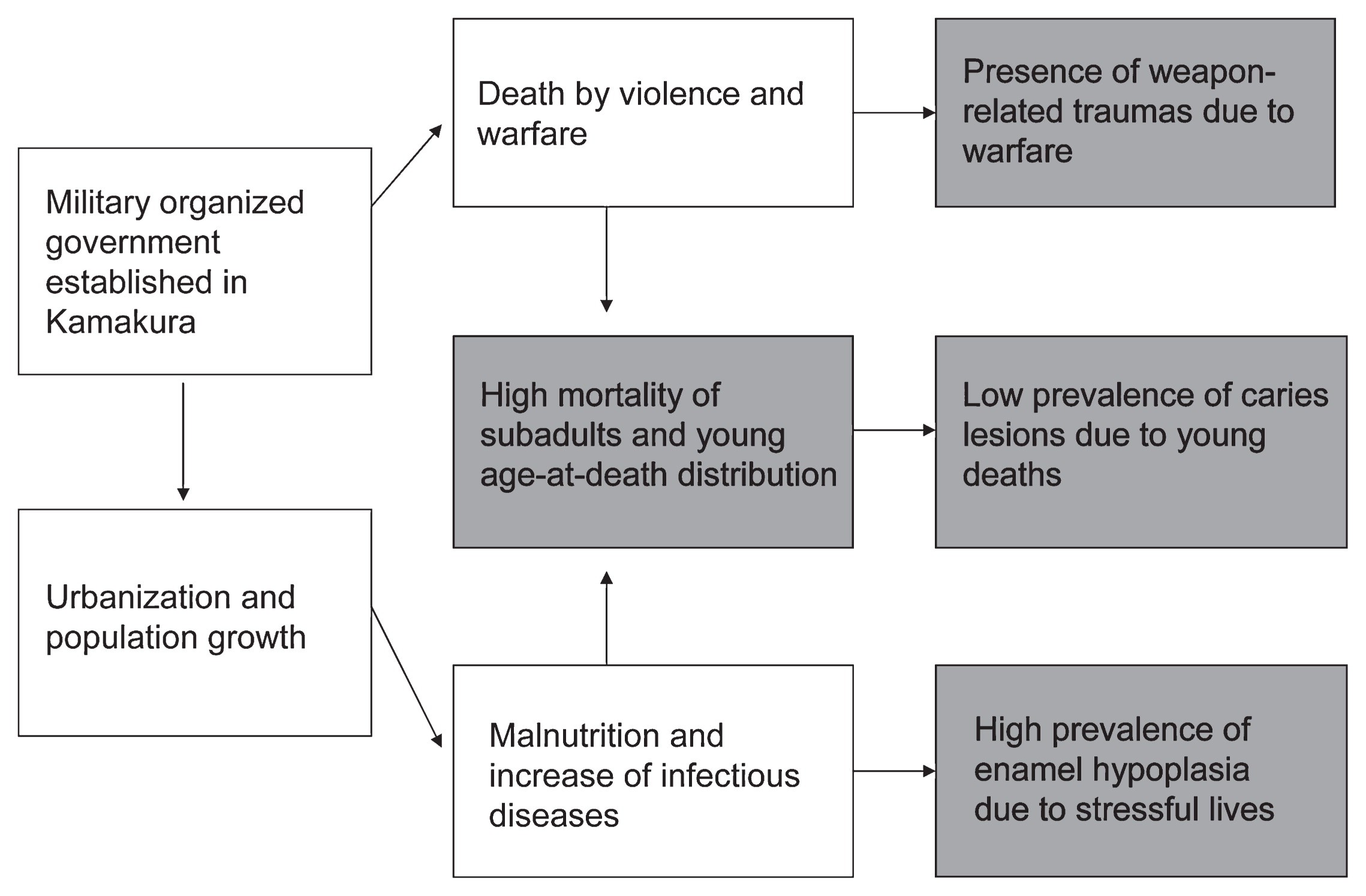
This study applied bioarchaelogical analyses to a new series of human skeletal remains from medieval Kamakura. All the results obtained here can be consistently explained by assuming severe living conditions prevailed in medieval Kamakura. The severity of living conditions in YCSB-SI can be considered to be the same as or worse than that in Edo. It is inferred from the present and previous data that population concentration in Kamakura impacted negatively on the lives of the inhabitants, possibly by malnutrition, increase of infectious diseases, and occasionally death by violence, and led to the high proportion of stress markers, the high proportion of deaths in young individuals, and the low prevalence rate of caries lesions (Figure 5). It is concluded that urbanization is a key to understanding the paleodemographic and paleopathological characteristics of the population. Although the sample size of the materials used in this study is small, this is the first to reveal life and death situations from the synthetic perspective of age-at-death distributions, AMTL, caries lesions, enamel hypoplasia, and weapon-related traumas.
Acknowledgments
This study is supported by JSPS Kakenhi (No. 22570222, 23770284).
References
- Bocquet-Appel, J.P. Masset, C. (1982) Farewell to palaeodemography. Journal of Human Evolution, 11: 321–333.
- Bocquet-Appel, J.P. Masset, C. (1985) Paleodemography: resurrection or ghost? Journal of Human Evolution, 14: 107–111.
- Bocquet-Appel, J.P. Masset, C. (1996) Paleodemography: expectancy and false hope. American Journal of Physical Anthropology, 99: 571–583.
- Brooks, S. Suchey, J.M. (1990) Skeletal age determination based on the os pubis: a comparison of the Acsadi–Nemeskeri and Suchey–Brooks methods. Human Evolution, 5: 227–238.
- Brothwell, D.R. (1981) Digging Up Bones. Cornel University Press, Ithaca, NY, pp. 59–75.
- Bruzek, J. (2002) A method for visual determination of sex using the human hip bone. American Journal of Physical Anthropology, 117: 157–168.
- Buckberry, J.L. Chamberlain, A.T. (2002) Age estimation from the auricular surface of the ilium: a revised method. American Journal of Physical Anthropology, 119: 231–239.
- Buikstra, J.E. Konigsberg, L.W. (1985) Paleodemography: critiques and controversies. American Antiquity, 87: 316–333.
- Chamberlain, A. (2006) Demography in Archaeology. Cambridge University Press, Cambridge.
- Duray, S.M. (1996) Dental indicators of stress and reduced age at death in prehistoric Native Americans. American Journal of Physical Anthropology, 99: 275–286.
- Fujikawa, Y. (1969) Nihon-shippei-shi. Heibonsha, Tokyo (in Japanese).
- Fujita, H. (1995) Geographical and chronological differences in dental caries in the Neolithic Jomon period of Japan. Anthropological Science, 103: 23–37.
- Goodman, A.H. Rose, J.C. (1990) Assessment of systemic physiological perturbations from dental enamel hypoplasias and associated histological structures. Yearbook of Physical Anthropology, 33: 59–110.
- Goodman, A.H. Armelagos, G.J. Rose, J.C. (1980) Enamel hypoplasias as indicators of stress in three prehistoric populations from Illinois. Human Biology, 52: 515–528.
- Hanley, B.S. (1997) Everyday Things in Premodern Japan: The Hidden Legacy of Material Culture. University of California Press, Berkeley.
- Hillson, S. (1996) Dental Anthropology. Cambridge University Press, Cambridge.
- Hirata, K. (1990) Secular trend and age distribution of cribra orbitalia in Japanese. Human Evolution, 5: 375–385.
- Hirata, K Nagaoka, T. (2005) Shutsudo jinkotsu no chosa. In: Tamagawa bunkazai kenkyusho (ed.), Yuigahama Chusei Shudan Bochi Iseki. Tamagawa bunkazai kenkyusho, Kanagawa, pp. 205–213 (in Japanese).
- Hirata, K. Oku, C. Hoshino, K. Tomo, S. Takahashi, S. (2002) Yuigahama-minami iseki no tantai maiso iko jinkotsu ni tsuite. In: Yuigahama-minami iseki hakkutsu chosa dan (ed.), Yuigahama-minami Iseki 2. Yuigahama-minami iseki hakkutsu chosa dan, Kamakura, pp. 1–240 (in Japanese).
- Hirata, K. Nagaoka, T. Hoshino, K. (2004) Analysis of injuries by swords in medieval Japanese skeletons from Yuigahama, Kamakura. Anthropological Science (Japanese Series), 112: 19–26 (in Japanese with English summary).
- Hirata, K. Nagaoka, T. Hoshino, K. Sawada, J. (2011) Kamakurashi yuigahama chiiki no chusei iseki shutsudo jinkotsu. In: Nakajo, T. Sakai, H. Ishida, H. (eds.), Kokogaku wo Kagaku suru). Rinsen shoten, Tokyo, pp. 207–232 (in Japanese).
- Hoppa, R.D. (2002) Paleodemography: looking back and thinking ahead. In: Hoppa, R.D. Vaupel, J.W. (eds.), Paleodemography: Age Distributions from Skeletal Samples. Cambridge University Press, Cambridge, pp. 9–28.
- Horowitz, S. Armelagos, G. Wachter, K. (1988) On generating birth rates from skeletal populations. American Journal of Physical Anthropology, 76: 189–196.
- Howell, N. (1976) Toward a uniformitarian theory of human paleodemography. Journal of Human Evolution, 5: 25–40.
- Howell, N. (1979) Demography of the Dobe !Kung. Academic Press, New York.
- Howell, N. (1982) Village composition implied by a paleodemographic life table. American Journal of Physical Anthropology, 59: 263–269.
- Hudson, M. (2009) Japanese beginning. In: Tsutsui, W.M. (ed.), The Companion to Japanese History. Wiley-Blackwell, Oxford, pp. 15–29.
- Irei, K. Doi, N. Fukumine, T. Nishime, A. Hanihara, T. Yoneda, M. Ishida, H. (2008) Dental diseases of human skeletal remains from the early-modern period of Kumejima Island, Okinawa, Japan. Anthropological Science, 116: 149–159.
- Kawano, S. (1995) Chusei Toshi Kamakura. Kodansha, Tokyo (in Japanese).
- Kito, H. (2000) Jinko kara yomu Nihon no Rekishi. Kodansha, Tokyo (in Japanese).
- Kobayashi, K. (1956) On the expectation of life in the late Tokugawa period. Journal of Anthropological Society Nippon, 65: 32–43 (in Japanese with English summary).
- Konigsberg, L.W. Frankenberg, S.R. (1992) Estimation of age structure in anthropological demography. American Journal of Physical Anthropology, 89: 235–256.
- Krogman, W.M. Iscan, M.Y. (1986) The Human Skeleton in Forensic Medicine. Charles C. Thomas, Springfield, IL, pp. 103–132.
- Larsen, C.S. (1997) Bioarchaeology. Interpreting Behaviour from the Human Skeleton. Cambridge University Press, Cambridge.
- Lewis, J.E. (2008) Identifying sword marks on bone: criteria for distinguishing between cut marks made by different classes of bladed weapon. Journal of Archaeological Science, 35: 2001–2008.
- Lovejoy, C.O. Meindl, R.S. Pryzbeck, T.R. Mensforth, R.P. (1985) Chronological metamorphosis of the auricular surface of the illium: a new method of determining adult age at death. American Journal of Physical Anthropology, 68: 15–28.
- Lukacs, J.R. (1992) Dental paleopathology and agricultural intensification in South Asia: new evidence. American Journal of Physical Anthropology, 87: 133–150.
- Lukacs, J.R. Largaespada, L.L. (2006) Explaining sex differences in dental caries prevalence: saliva, hormones, and ‘life-history’ etiologies. American Journal of Human Biology, 18: 540–555.
- Matsushita, T. (2002) Kamakurashi yuigahama-minami iseki shukotsubo shutsudo chusei jinkotsu no maiso to kotaisu oyobi jusho jinkotsu. In: Yuigahama-minami iseki hakkutsu chosa dan (ed.), Yuigahama-minami iseki 3. Yuigahama-minami iseki hakkutsu chosa dan, Kamakura, pp. 101–134 (in Japanese).
- Mensforth, R.P. (1990) Paleodemography of the Carlston Annis (Bt-5) late archaic skeletal population. American Journal of Physical Anthropology, 82: 81–99.
- Moorrees, C.F. Fanning, E.A. Hunt, E.E.Jr (1963a) Age variation of formation stages for ten permanent teeth. Journal of Dental Research, 42: 1490–1502.
- Moorrees, C.F. Fanning, E.A. Hunt, E.E.Jr (1963b) Formation and resorption of three deciduous teeth in children. American Journal of Physical Anthropology, 21: 205–213.
- Morimoto, I. (1987) Note on the technique of decapitation in medieval Japan. Journal of Anthropological Society Nippon, 95: 477–486.
- Morimoto, I. Hirata, K. (1992) A decapitated human skull from medieval Kamakura. Anthropological Science, 100: 349–358.
- Morimoto, I. Takahashi, Y. Hirata, K. (1984) Jinkotsu no shoken. In: Kamakura city board of education (ed.), Kamakurashi Chusei Shudan Bochi (Tokushu Yogo Rojin Homu Kamakura Seiyokan Kensetsu Yoteichi) Hakkutsu Chosa Hokokusho. Kamakura City Board of education, Kamakura, pp. 8–11 (in Japanese).
- Nagaoka, T. (2012) Cranial traumatic injuries caused by weapons in Tokugawa Japan. International Journal of Osteoarchaeology, 22: 138–144.
- Nagaoka, T. Hirata, K. (2007) Reconstruction of paleodemographic characteristics from skeletal age at death distributions: perspectives from Hitotsubashi, Japan. American Journal of Physical Anthropology, 134: 301–311.
- Nagaoka, T. Hirata, K. (2008) Demographic structure of skeletal populations in historic Japan: a new estimation of adult age-at-death distributions based on the auricular surface of the ilium. Journal of Archaeological Science, 135: 1370–1377.
- Nagaoka, T. Hirata, K. Yokota, E. Matsu’ura, S. (2006) Paleodemography of a medieval population in Japan: analysis of human skeletal remains from the Yuigahama-minami site. American Journal of Physical Anthropology, 131: 1–14.
- Nagaoka, T. Sawada, J. Hirata, K. (2008) Did the Jomon people have a short lifespan? Evidence from the adult age-at-death estimation based on the auricular surface of the ilium. Anthropological Science, 116: 161–169.
- Nagaoka, T. Uzawa, K. Hirata, K. (2009) Weapon-related traumas of human skeletons from Yuigahama chusei shudan bochi, Japan. Anatomical Science International, 84: 170–181.
- Nagaoka, T. Uzawa, K. Hirata, K. (2010) Evidence for weapon-related traumas in medieval Japan: observations of the human crania from Seiyokan. Anthropological Science, 118: 129–140.
- Nagaoka, T. Abe, M. Shimatani, K. (2012a) Estimation of mortality profiles from non-adult human skeletons in Edo-period Japan. Anthropological Science, 120: 115–128.
- Nagaoka, T. Ishida, H. Shimoda, Y. Sunagawa, M. Amano, T. Ono, H. Hirata, K. (2012b) Estimation of skeletal adult age distribution of Okhotsk people in northern Japan. Anthropological Science, 120: 103–113.
- Ohkouchi, T. (1986) Kanagawaken Yuigahama chusei shudan bochi iseki. Nippon Kokogaku Nenpo, 39: 444–449 (in Japanese).
- Ohshima, N. (1996) Chronological changes of dental caries frequencies of human skeletal remains in Hokkaido. Anthropological Science (Japanese Series), 104: 385–397 (in Japanese).
- Oyamada, J. Manabe, Y. Kitagawa, Y. Rokutanda, A. (1996) Dental morbid condition of hunter-gatherers on Okinawa island during the middle period of the prehistoric shell midden culture and of agriculturalists in northern Kyushu during the Yayoi period. Anthropological Science, 104: 261–280.
- Oyamada, J. Kitagawa, Y. Kato, K. Matsushita, T. Tsurumoto, T. Manabe, Y. (2012) Sex differences in linear enamel hypoplasia (LEH) in early modern Japan. Anthropological Science, 120: 97–101.
- Phenice, T.W. (1969) A newly developed visual method of sexing the os pubis. American Journal of Physical Anthropology, 30: 297–301.
- Sakaue, K. (2006) Application of the Suchey–Brooks system of pubic age estimation to recent Japanese skeletal material. Anthropological Science, 114: 59–64.
- Sakura, H. (1964) Historical changes in the frequency of dental caries among the Japanese people. Journal of Anthropological Society Nippon, 71: 153–157 (in Japanese with English summary).
- Sawada, J. (2010) Childhood health of the Jomon and Yayoi people as revealed by analysis of enamel hypoplasia. The Achaeological Journal, 606: 33–37 (in Japanese with English title).
- Scheuer, J.L. Musgrave, J.H. Evans, S.P. (1980) The estimation of late fetal and perinatal age from limb bone length by linear and logarithmic regression. Annals of Human Biology, 7: 257–265.
- Shimoda, Y. Nagaoka, T. Moromizato, K. Sunagawa, M. Hanihara, T. Yoneda, M. Hirata, K. Ono, H. Amano, T. Fukumine, T. Ishida, H. (2012) Degenerative changes of the spine in people from prehistoric Okhotsk culture and two ancient human groups from Kanto and Okinawa, Japan. Anthropological Science, 120: 1–21.
- Starling, A.P. Stock, J.T. (2007) Dental indicators of health and stress in early Egyptian and Nubian agriculturalists: a difficult transition and gradual recovery. American Journal of Physical Anthropology, 134: 520–528.
- Storey, R. (2007) An elusive paleodemography? A comparison of two methods for estimating the adult age distribution of deaths at late Classic Copan, Honduras. American Journal of Physical Anthropology, 132: 40–47.
- Suzuki, H. Watanabe, H. Iwamoto, M. Masuda, S. Inamoto, N. Hayashi, T. Tanabe, Y. Sakura, H. Kohara, Y. (1956) Medieval Japanese skeletons from the burial site at Zaimokuza, Kamakura City. In: Anthropological Society of Nippon (ed.), Zaimokuza Site and Human Skeletons at Kamakura City. Iwanami shoten, Tokyo, pp. 1–194 (in Japanese with English summary).
- Todaka, Y. Oyamada, J. Manabe, Y. Kitagawa, Y. Kato, K. Rokutanda, A. (2003) The relationship between immigration and the prevalence of dental caries in the Yayoi people. Anthropological Science, 111: 265–292.
- Todd, T.W. (1920) Age changes in the pubic bone, 1. The male White pubis. American Journal of Physical Anthropology, 3: 285–339.
- Todd, T.W. (1921) Age changes in the pubic bone, 2. The pubis of the male Negro–White hybrid. American Journal of Physical Anthropology, 4: 1–26.
- Ubelaker, D.H. (1989) Human Skeletal Remains. Excavation, Analysis, Interpretation, 2nd edn. Aldine, Chicago.
- Yamamoto, M. (1988) Enamel hypoplasia of the permanent teeth in Japanese from the Jomon to the modern periods. Journal of Anthropological Society Nippon, 96: 417–433 (in Japanese with English summary).
- Yoneda, M. Shibata, Y. Doi, N. (2004) Palaeodiet on the Ryukyu Islands: isotope analyses of prehistoric Gusuku and recent periods. Anthropological Science, 112: 290.
- Wakebe, T. (1990) A morphological study of crania of infants and children in the Japanese. Nagasaki Medical Journal, 65: 805–824.
- Walker, P.L. (2008) Sexing skulls using discriminant function analysis of visually assessed traits. American Journal of Physical Anthropology, 136: 39–50.
- Walker, P.L. Long, J.C. (1977) An experimental study of the morphological characteristics of tool marks. American Antiquity, 42: 605–616.
- Weiss, K.M. (1973) Demographic models for anthropology. Memoirs of the Society for American Archaeology 27, American Antiquity, 38, 1–186.
