Abstract
The Rakhigarhi site is the location of the ruins of an ancient megacity of the Harappan civilization and had not previously been investigated thoroughly. We tried to examine the physical and pathological traits of human skeletons (n = 37) from the cemetery at the site. In our study, a cranial index was calculated from one male skull (dolichocranic; index value = 65.78). The mean statures estimated by long bone length were 175.8 cm (male) and 166.1 cm (female). The indices of femoral diaphyseal shape were 79.8 (males) and 90.31 (females) for the platymeric index; and 113.78 (males) and 112.74 (female) for the pilasteric index. The dental health of the subjects appeared to be good as the overall prevalence of oral pathologies (caries and antemortem tooth loss) was generally low. Periosteal reactions were found in tibias and possible evidence of osteomyelitis was also observed in a femur. Some joint parts showed signs of osteoarthritis. Although various pathologies have been identified, we could not find any specific lesions suggestive of leprosy and tuberculosis in these skeletons. Although our study has added invaluable data to the existing information pool on the health and disease status of Harappan society, more accurate conjecture on the structure of Harrappan society based on bioarchaeological evidence will need additional research based on future excavations at Rakhigarhi cemetery.
Introduction
Since its discovery in the 1920s, the Harappan civilization has been revealed to be one of the earliest and most prosperous urban civilizations of ancient times. During the mature Harappan period (c. 2600–1900 BCE), settlements included a wide network of urban and rural sites that varied in size and function. At the height of the civilization, cities and towns covered a vast area of South Asia; its sphere of influence was much larger than the Mesopotamian and Egyptian civilizations combined (Possehl, 1993; Kenoyer, 1998; Shinde, 2016). The largest city ruins discovered so far include Kalibangan, Mohenjo Daro, Harappa, Rakhigarhi, and Dholavira (Shinde, 2016). This civilization boasted highly sophisticated technology, and the Harappans developed megacity areas as political and administrative regional centers, managing civic amenities such as defensive walls, dams, reservoirs, canals, drainage, public facilities, elaborate water management and sanitation systems, etc. (Shinde, 2016).
As for human remains, approximately 600 Harappan individuals have been surveyed in about 50 burial sites so far (Dibyopama et al., 2015; Valentine et al., 2015). Some important pioneering studies have provided valuable information on the physical and pathological traits of the Harappan people. In brief, Robbins et al. (2009) reported the identification of a leprosy patient among the ancient skeletons of the Balathal site, dating to before the first millennium BC, reconfirming the authenticity of the first textual reference to leprosy in early Vedic scriptures. Robbins Schug et al. (2013) reported that the prevalence of infection among skeletons from the burial areas at Harappa increased over time; the risk of the infection differentiated between burial communities. Robbins Schug et al. (2012) and Lovell (2014) examined the signs of trauma in human bones from the city of Harappa (3300–1300 BCE), showing that patterns of violence characterized the society, contradicting the conception of the Harappan civilization as a peaceful prehistoric realm. Nath et al. (2015) reported archaeoanthropological information obtained during the excavation of Harappan interments at Rakhigarhi, Haryana. They estimated stature based on long bone measurements, and also acquired other fundamental anthropological data. Additionally, Lukacs (2017) indicated that Harappans exhibited greater occlusal wear, smaller teeth, and a distinct dental pathology profile. In particular, Harappan farmers exhibited higher caries rates and calculus than Holocene foragers.
Despite these pioneering achievements, there is still much work to be done to achieve complete understanding of the Harappan people’s biomedical traits. Considering the significance of the Harappan civilization in world history, more investigations should be done on cemetery remains from the same period. The purpose of the current research is thus to explore the physical and pathological traits of the Harappan people by examining human bones from graves that have not previously been investigated. The cemetery of Rakhigarhi, the largest Harappan city categorized as a political and administrative regional center at that time (Shinde et al., 2015), was investigated by Nath et al. (2015), though most burials there remained uninvestigated. In 2015–2016, several graves at the same Rakhighari cemetery were newly investigated by us, i.e. teams from Deccan College, Post-Graduate and Research Institute, Deemed University (India), the Department of Archaeology & Museums, Haryana (India), and Seoul National University College of Medicine (South Korea) (Shinde et al., 2018). Bioanthropological studies were carried out on the human bones we collected from the Rakhigarhi cemetery, adding invaluable information to the existing pool and helping to unravel the physical and pathological traits of the Harappan people.
Materials and Methods
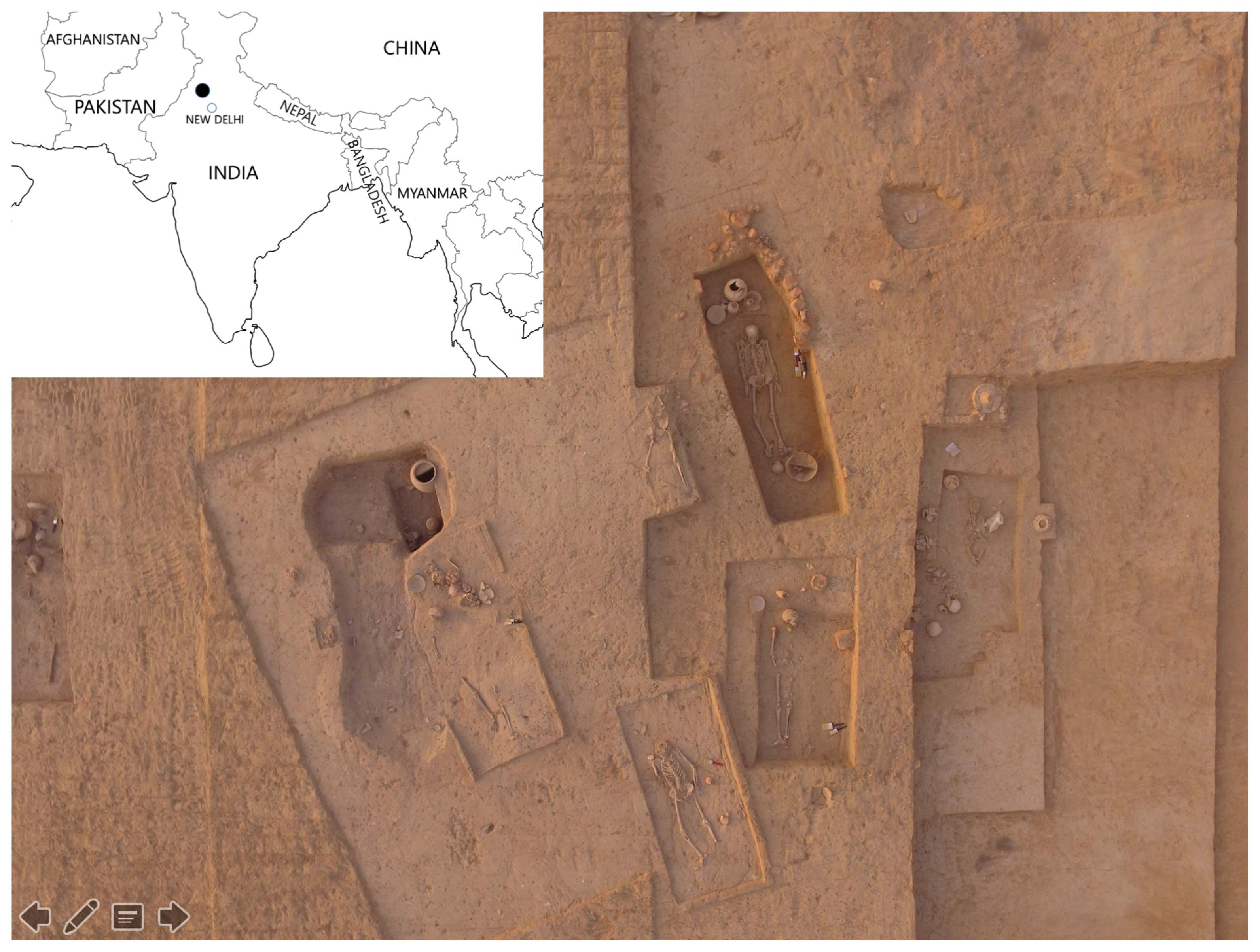
Rakhigarhi is a village in Hisar District of the state of Haryana, India (Figure 1) (Shinde et al., 2015). The skeletons examined in this study were recovered (2015–2016) from locations RGR 7.2 (trenches A1 and A2) and RGR 7.3 (trenches B1 and B2) of a cemetery in Rakhigarhi (Shinde et al., 2018). Radiocarbon dating by accelerator mass spectrometry (performed at the Inter University Accelerator Center) was done on charcoal samples obtained at site depths of 9.1 and 20.6 m. Calibrated dates were 2273 ± 38 and 2616 ± 73 years BCE for the former and latter specimens, respectively (Vahia et al., 2016). Detailed information of our excavation at the cemetery is available in a previous archaeological report (Shinde et al., 2018).
Our excavations uncovered the remains of at least 37 complete or partial individuals, excluding isolated skeletal elements (Table 1). Overall, the preservation status of skeletons was not good; many of them were fragmentary or incomplete. The skeletal remains were analyzed to reveal the biological traits of the Harappan population. The sex and age were estimated for each skeletal individual, based on the Standards for Data Collection (Buikstra and Ubelaker, 1994; Ubelaker, 1999). The results are summarized in our previous report (Shinde et al., 2018), and are listed in Table 1. We measured the morphological features of the individuals based on Martin’s methods of standard anthropometric measurements (Martin and Knussmann, 1988). All measurements were taken twice and then averaged.
Table 1
Skeletal samples used in this study
| Locality |
Trench |
Burial no. |
Sex |
Age |
Burial type |
| RGR 7.2 (n = 28) |
A1 (n = 4) |
BR 01 |
|
Male |
36–50 years |
Primary |
| BR 02 |
|
Male |
16–18 years |
Primary |
| BR 03 |
|
Indeterminate |
3–5 years |
Primary |
| BR 04 |
|
Female |
36–50 years |
Primary |
| A2 (n = 24) |
BR 07 |
|
Indeterminate |
36–50 years |
Primary |
| BR 08 |
|
Indeterminate |
Indeterminate |
Primary |
| BR 09 |
|
Indeterminate |
36–50 years |
Primary |
| BR10 |
A |
Indeterminate |
2–4 years |
Primary |
| B |
Indeterminate |
Indeterminate |
Primary |
| BR 12 |
|
Indeterminate |
Indeterminate |
Primary |
| BR 13 |
|
Indeterminate |
Indeterminate |
Primary |
| BR 15 |
|
Female |
Indeterminate |
Primary |
| BR 17A |
|
Indeterminate |
2–4 years |
Primary |
| BR18 |
A |
Indeterminate |
Indeterminate |
Primary |
| B |
Indeterminate |
Indeterminate |
Primary |
| BR 19 |
|
Female |
21–35 years |
Primary |
| BR20 |
A |
Indeterminate |
36–50 years |
Primary |
| B |
Indeterminate |
2–4 years |
Primary |
| BR 22 |
|
Female |
21–35 years |
Primary |
| BR 23 |
|
Indeterminate |
Juvenile |
Primary |
| BR 24 |
|
Female |
Indeterminate |
Primary |
| BR 25 |
|
Male |
36–50 years |
Primary |
| BR 26 |
|
Indeterminate |
36–50 years |
Primary |
| BR 28 |
|
Indeterminate |
Indeterminate |
Primary |
| BR 31 |
|
Female |
>50 years |
Primary |
| BR 33 |
|
Female |
21–35 years |
Primary |
| BR 35 |
|
Indeterminate |
12–16 years |
Primary |
| BR 36 |
|
Female |
36–50 years |
Primary |
| RGR 7.3 (n = 9) |
B1 (n = 1) |
BR 01A |
|
Male |
21–35 years |
Primary |
| B2 (n = 8) |
BR02 |
A1 |
Male |
21–35 years |
Primary |
| A2 |
Indeterminate |
36–50 years |
Secondary |
| B |
Female |
36–50 years |
Secondary |
| C1 |
Male |
16–18 years |
Primary |
| C2 |
Indeterminate |
Indeterminate |
Secondary |
| BR 03 |
A |
Male |
Indeterminate |
Primary |
| B |
Indeterminate |
Indeterminate |
Primary |
| BR 04 |
|
Female |
36–50 years |
Primary |
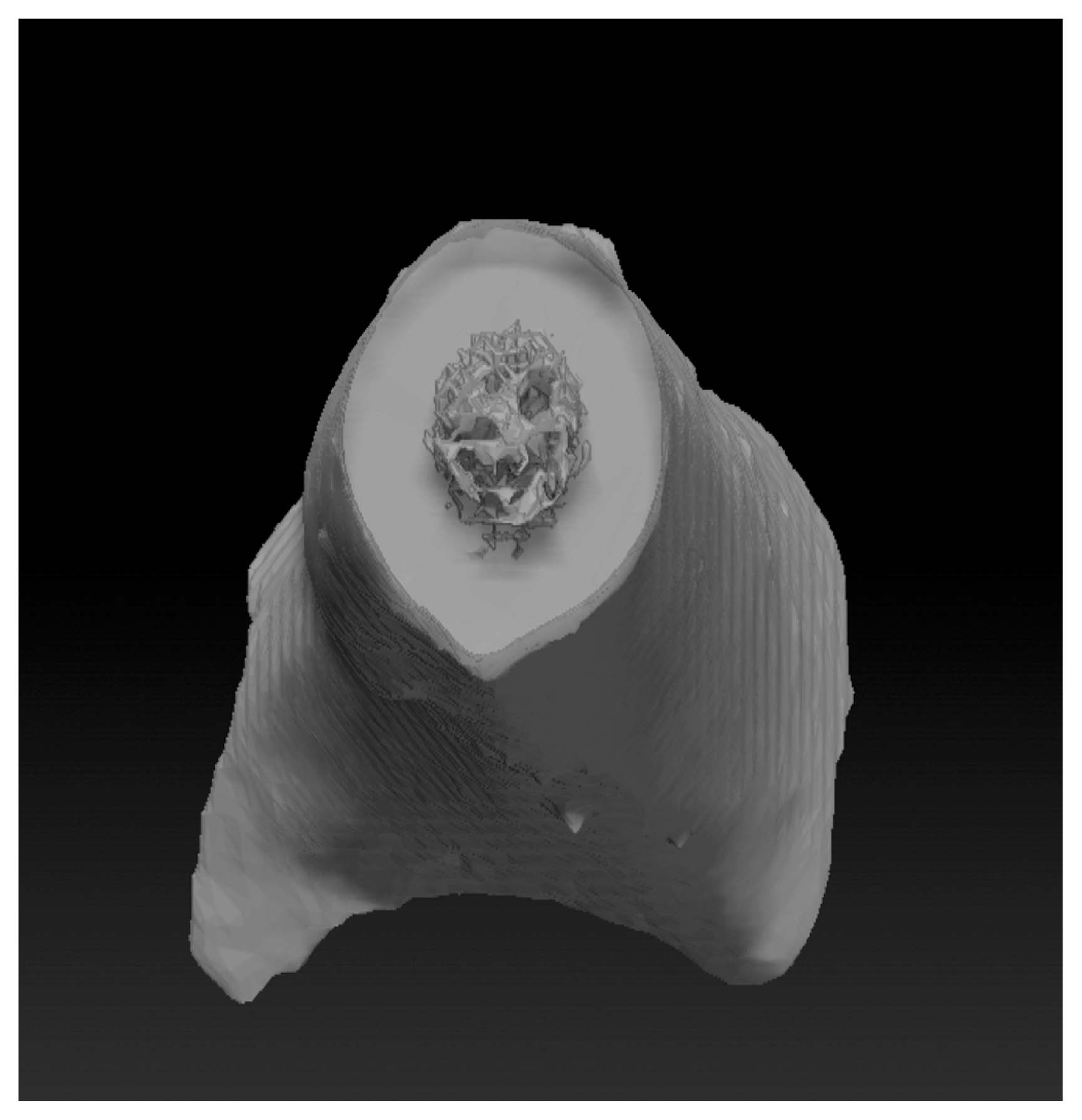
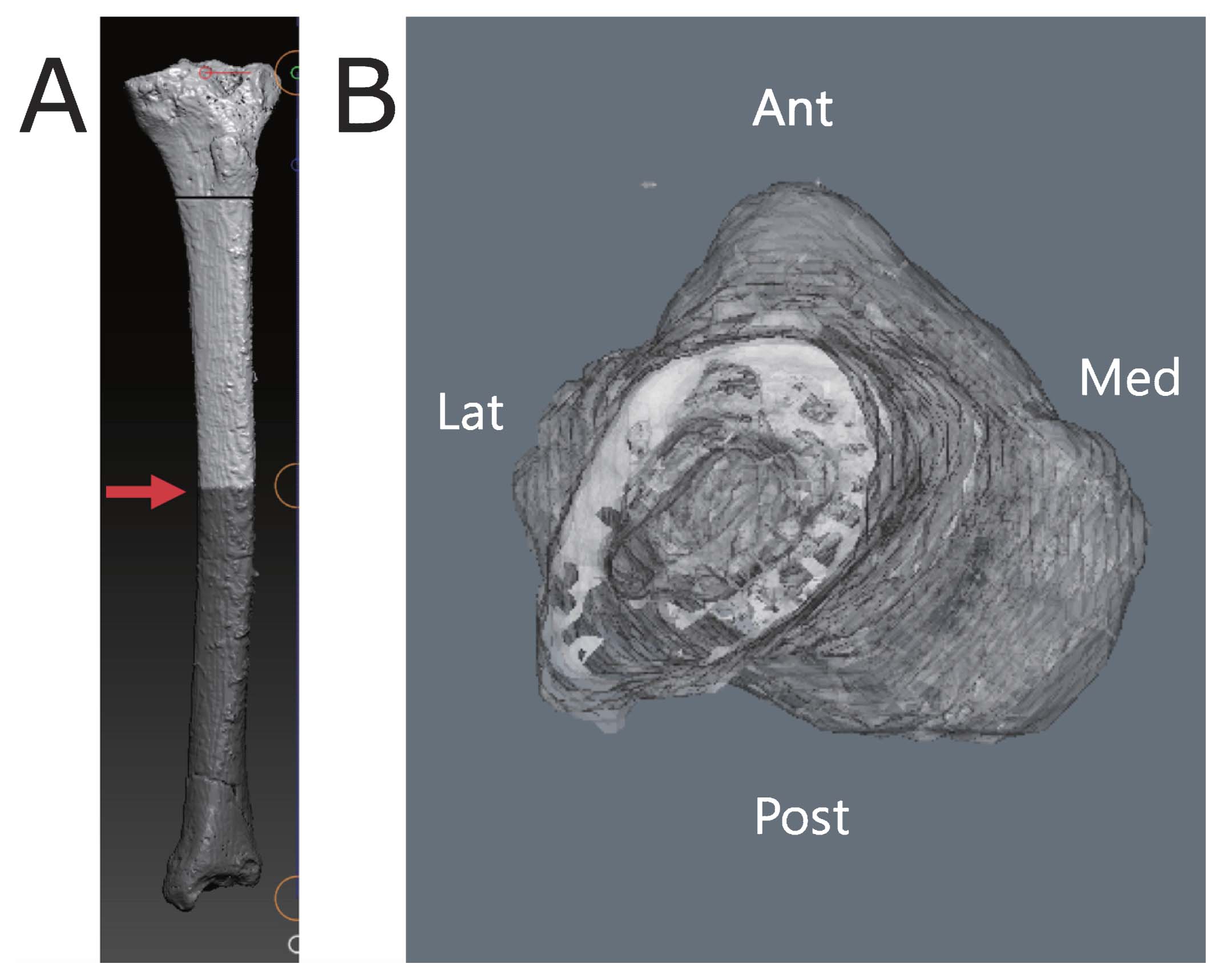
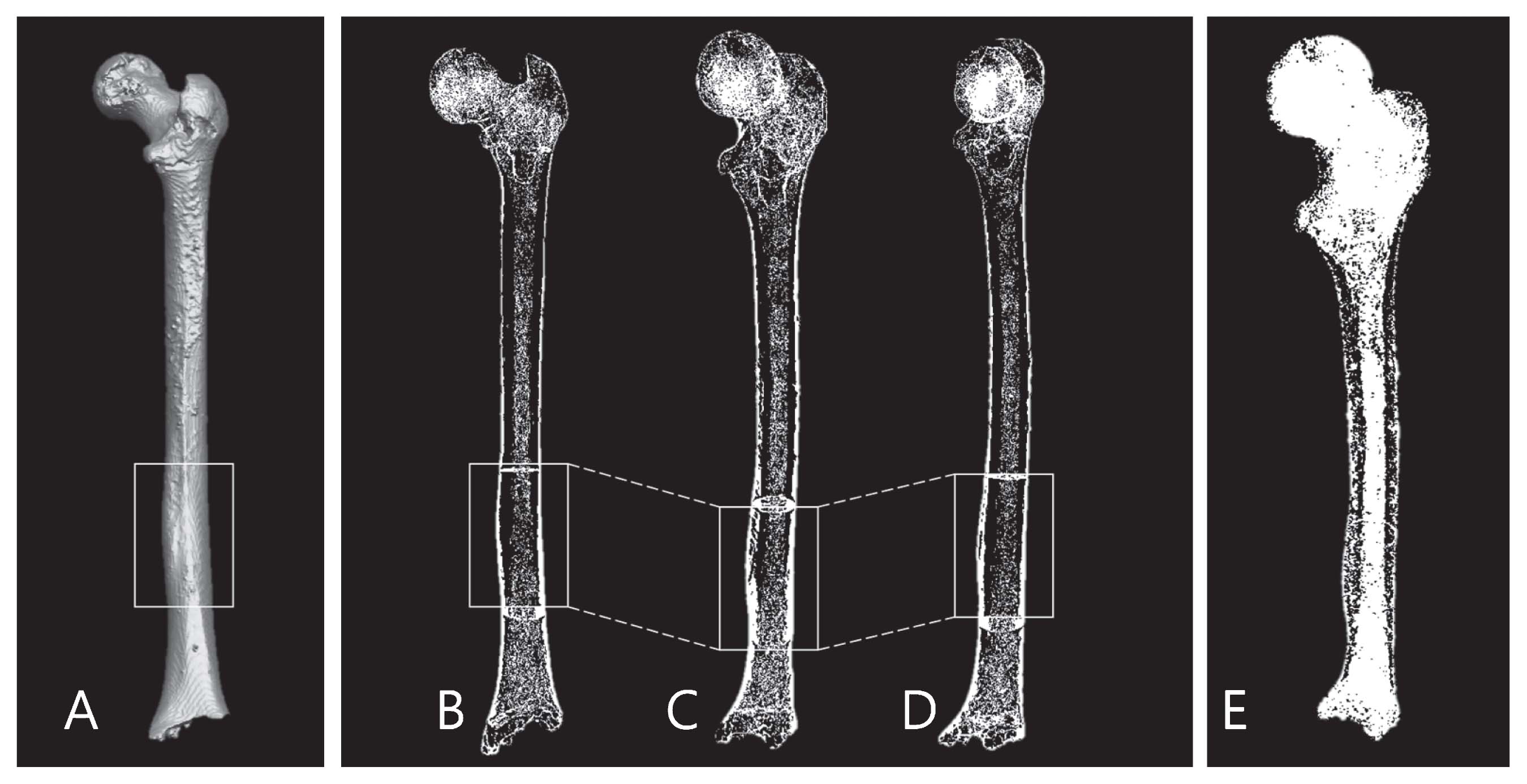
Due to the skeletal remains being plastered with hard material, we had difficulties in undertaking conventional macroscopic examinations of the specimens (Figure 2). X-ray fluorescence (XRF) tests were performed to determine the chemical composition of the hard material (Korea Institute of Geoscience and Mineral Resources, Daejeon). Chemical analysis allows identification of different areas of provenance of the raw materials in the context of specific historical periods. When conventional measurements were difficult, we scanned the bones by computed tomography (CT) (Siemens, Erlangen, Germany). Then, we virtually removed the hard materials from the bony surface on the three-dimensional reconstructed images. We managed to take measurements based on the images (Figure 3).

Cranial index (CI) was calculated by (maximum cranial breadth/maximum cranial length) × 100. CI was further categorized into dolichocranic (≤74.9), mesocranic (75–79.9), and brachycranic (80–84.9) (Liebenberg et al., 2015). We estimated the stature of the Rakhigarhi people from the maximum length of the long bones, following the Trotter–Gleser formula (Trotter and Gleser, 1958). Indices of diaphyseal shape in the femur were also calculated as shown in Appendix 1. The robusticity of the femur is evaluated in indexes that consider the anteroposterior and mediolateral dimensions of the subtrochanter and midshaft region. We note that long bone diaphyseal shape reflects the personal history of mechanical loading, and thus can be used to evaluate the physical activity level of human populations (Larsen, 1987; Ruff, 1987). The femur platymeric index, indicating the general shape of proximal femur diaphysis, was classified into broad or platymeria (≤84.9), more rounded or eurymeria (85.0–99.9), and less frequently, anteroposteriorly broad or stenomeria (100.0≤) (Tallman and Winburn, 2015). When the presence of hard materials on the bones interfered with manual measurements, CT reconstructed images were used to calculate the indices of femoral diaphyseal shape (Stock and Shaw, 2007; see Appendix 2).
Skeletal remains were examined for the presence of stress indicators. We note that periosteal reaction represents episodes of physiological stress caused by an acute illness and/or an inflammatory response to nutritional inadequacy and trauma (Lovell, 2014). Specific lesions consistent with leprosy and tuberculosis were investigated following the method of Robbins Schug et al. (2013) and Robbins Schug (2017). Evidence for osteoarthritis was also examined in the Rakhigarhi skeletons. Dental remains were investigated for caries, enamel hypoplasia, antemortem tooth loss (AMTL), and dental attrition following the method of Lukacs (2017). A sample of 445 teeth were inspected with oblique incandescent light. Deciduous teeth were from 3 individuals (total teeth = 35), and the permanent teeth from 17 individuals (total teeth = 410). Data on AMTL were collected from alveolar bone. A tooth was considered to be present when the tooth socket could be identified.
Results and Discussion
In this study, the CI was obtained from only one male cranium (7.3 B2 Burial 2C-1): dolichocranic (index value = 65.78). In a previous report of the Rakhigarhi excavation in 1997–1998, the CI was also obtained from a male cranium. The individual’s maximum cranial length and breadth were 178 mm and 133 mm, respectively (Nath et al., 2015), thus being categorized as dolichocranic (index value = 74.72). Walimbe and Tavares (2002) also demonstrated that the inhabitants of the mature Harappan era, to which the Rakhigarhi site belonged, were in general dolichocranic. The current CI result is not very different from previous reports on Harappans from this period. In the past several decades, researchers have figured out the anthropological identities of past populations of the Harappan civilization, particularly using human skeletal remains from excavation sites (Hemphill et al., 1991; Kennedy, 1995, 2000; Walimbe, 2007, 2014, 2016; Mushrif-Tripathy, 2014). Although the CI result of this report might have similar academic significance, we could not evaluate it clearly because the amount of Rakhgarhi specimen is insufficient to clarify the conclusion.
Some individuals’ long bone measurements could not be easily measured due to hard materials adhering to the bony surfaces. The chemical composition of these hard materials, as revealed by XRF, is summarized in Table 2. The most abundant elements in the hard materials were silicon dioxide (SiO2) and calcium oxide (CaO). Considering the former is the main component of quartz in the soil and the latter is also known as quicklime or burnt lime, the material appears to be a liming soil. We inferred that the liming soil might have been used for grave construction at least in the eastern part of the Harappan civilization sphere. In those cases, we actively used CT reconstruction images to overcome the difficulties with conventional manual examination of the bones (Table 3, Table 4).
Table 2
X-ray fluorescence data of the hard materials present on the surface of the Rakhigarhi skeletons
| Constituent |
SiO2 |
Al2O3 |
Fe2O3 |
CaO |
MgO |
| Wt.% |
28.32 |
6.74 |
2.83 |
31.89 |
1.62 |
| K2O |
Na2O |
TiO2 |
MnO |
P2O5 |
Igloss |
| 1.80 |
0.66 |
0.31 |
0.10 |
0.42 |
25.81 |
Table 3
Stature estimation based on long bone length
| Individual (sex) |
Side/bone |
Measurement (manual*/CT**) |
Trotter and Gleser (1958) |
| 7.2 BR-01 (♂) |
Right femur |
484 (CT) |
176.63 ± 3.8 |
| 7.2 BR-02 (♂) |
Right fibula |
403 (manual) |
177.28 ± 3.24 |
| 7.2 A2 BR-9 (?) |
Right humerus |
325 (manual) |
170.29 ± 4.25 |
| 7.2 A2 BR-22 (♀) |
Left tibia |
328 (CT) |
159.79 ± 3.27 |
| 7.2 A2 BR-36 (♀) |
Left humerus |
313 (CT) |
167.07 ± 4.25 |
| 7.3 B1 BR-1 (♂) |
Left femur |
486 (manual) |
177.06 ± 3.8 |
| 7.3 B2 BR-2A-1 (♂) |
Left femur |
496 (manual) |
179.21 ± 3.8 |
| 7.3 B2 BR-2B (♀) |
Right ulna |
253 (manual) |
165.49 ± 4.66 |
| 7.3 B2 BR-2C-1 (♂) |
Right tibia |
410 (CT) |
179.39 ± 3.27 |
| 7.3 B2 BR-3A (♂) |
Left humerus |
307 (manual) |
165.47 ± 4.25 |
| 7.3 B2 BR-4 (♀) |
Left tibia |
379 (manual) |
171.98 ± 3.27 |
** Computed tomography-based three-dimensional reconstruction.
Table 4
Indices of femoral diaphyseal shape in this study
| Individual (sex) |
Platymeric |
Pilasteric |
Measurements (manual*/CT**) |
| 7.2 BR-01 (♂) |
R: 56.63 |
R: 135.16 |
CT |
| 7.2 BR-02 (♂) |
L: 82.65, R: 84.45 |
R: 103.65 |
Manual |
| 7.2 BR-04 (♀) |
R: 82.39 |
|
CT |
| 7.2 A2 BR-09 (?) |
R: 99.90 |
|
CT |
| 7.2 A2 BR-24 (♀) |
L: 83.47, R: 85.70 |
R: 108.18 |
CT |
| 7.2 A2 BR-25 (♂) |
R: 85.59 |
R: 108.62 |
CT |
| 7.2 A2 BR-33 (♀) |
L: 98.99, R: 97.65 |
L: 134.3, R: 131.4 |
Manual |
| 7.3 B1 BR-1 (♂) |
L: 89.83, R: 86.59 |
L: 107.99, R: 113.72 |
Manual |
| 7.3 B2 BR-2A-1 (♂) |
L: 87.65, R: 85.76 |
L: 122.38, R: 121.17 |
Manual |
| 7.3 B2 BR-2C-1 (♂) |
L: 77.26 |
L: 101.05, R: 100.35 |
Manual |
| 7.3 B2 BR-4 (♀) |
R: 95.51 |
R: 98.64 |
CT |
** Computed tomography-based three-dimensional reconstruction.
The stature of the Rakhigarhi people was estimated from the maximum length of the long bones, as summarized in Table 3. The estimated mean stature was 175.8 cm (range 165.5–179.4 cm) for males (n = 6) and 166.1 cm (range 159.8–172.0 cm) for females (n = 4). Male stature on average was about 9 cm higher than female stature (Table 3). Previous estimated statures of skeletal individuals collected from the same Rakhigarhi cemetery (1997–1998) were approximately 171–178 cm for males and 155–165 cm for females (Nath et al., 2015). Comparing the previous report with ours, the heights of males in this study are almost within the same range as 1997–1998 data, though our females are taller than those of Nath et al. (2015). The difference in female height might reflect the social differentiation between the localities at the Rakhigarhi cemetery. Alternatively, this difference may be caused by a greater female response to poor nutrition in the population with the increasing development of social hierarchy.
The calculated indices of diaphyseal shape of femur are also summarized in Table 4. Overall, diaphyseal measurements of long bones have provided insights into biomechanical patterns in prehistory. In our Rakhigarhi cases, the platymeric index value for the femoral subchanteric region ranged between 56.63 and 89.83 (mean = 79.8) for males (right-sided, n = 5), and between 82.39 and 98.99 (mean = 90.31) for females (right-sided, n = 4). Our results showed that the mean platymeric index is obviously greater in females; that is, the subtrochanteric areas in males are flatter than in females. This difference might have been due to different locomotor behavior between sexes, which should be further investigated for its possible social implications. The pilasteric index, the external breadth index of femoral shafts, was also calculated in this study. It ranged from 100.35 to 135.16 (mean = 113.78) for males (right, n = 6) and from 98.64 to 134.3 (mean = 112.74) for females (right, n = 3). Unlike the platymeric index, the pilasteric indices did not differ much between sexes. In general, a high pilasteric index is known to be caused by intense exercise such as the contraction of the hamstrings and quadriceps muscles while running or climbing (Morrison, 1970; Ruff, 1987; Stock and Pfeiffer, 2004; Wescott, 2005). As our pilasteric index is relatively higher than the other groups already reported (Wescott, 2005; Pomeroy and Zakrzewski, 2009), the Rakhigarhi people examined by us might have experienced high levels of mobility.
The dental health of the Rakhigarhi people was relatively good and the overall prevalence of oral pathologies was very low (Table 5). For instance, caries was seen in only three individuals (7-2 A1 BR 02, 7.2 A2 BR 07, 7.3 B2 BR 04) and AMTL was observed only in two individuals (7-2 A1 BR 01, 7.2 A2 BR 31). The ratios of caries to caries-free are 2.8% (male), 1.0% (female) and 1.3% (sex-indeterminate), respectively (Table 4). In this study, enamel defects were also observed in a female, a male and two children (sex-indeterminate). In a previous study, linear enamel hypoplasia (LEH) was a commonly observed dental disease among a Harappan population (Lukacs, 1991). Meanwhile, LEH was also observed in a female adult (7.2 A2 BR 33) and an immature male individual (7.3 B2 BR02 C1) in the current report.
Table 5
Frequency and prevalence of teeth affected by caries, enamel defects, and antemortem tooth loss (AMTL)
|
Caries |
Enamel defects |
AMTL |
|
caries/caries-free |
% |
defects/defects-free |
% |
AMTL/AMTL-free |
% |
| Males |
4/139 |
2.8 |
7/136 |
4.9 |
1/143 |
0.7 |
| Females |
2/189 |
1.0 |
2/189 |
1.0 |
14/191 |
7.3 |
| Indeterminate |
1/75 |
1.3 |
3/76 |
3.9 |
0/76 |
0 |
In general, localized hypoplastic defects are detected in deciduous teeth, as seen in many studies on prehistoric South Asian skeletons (Lukacs and Hemphill, 1990, 1991; Lukacs and Pal, 1993; Hemphil et al., 1991; Meadow, 1991). In this study, localized hypoplastic defects were also observed only in the deciduous canine teeth of two children (7.2 A1 BR03 and 7.2 A2 BR10A). As for why the localized enamel defects occurred in deciduous teeth, we note that it is commonly observed among nutritionally disadvantaged groups (Skinner, 1996), especially in case of diets with low retinol content (Lukacs and Walimbe, 1998). Malnutrition, an environmental stressor that is regarded as a primary cause of enamel defects (Lovell and Whyte, 1999), might have been related to localized enamel defects in some deciduous teeth from Rakhigarhi cemetery.
Previous analysis of Rakhigarhi skeletons in 1997–1998 also indicated that attrition was serious in the examined teeth (Nath et al., 2015). In our sample from the Rakhigarhi site, severe dental attritions were commonly observed as well (Figure 4). They were frequently seen in the anterior teeth of the maxilla of the middle- and old-aged adults, particularly in the lingual surface of them. In general, dental attrition reflects dietary habits, food preparation methods, and occupational activities of the population. Lingual surface attrition of maxillary anterior teeth may be due to forceful holding or pulling of animal skin between the teeth for the purpose of softening it (Lukacs and Pastor, 1988).

In their examination of skeletons from Cemetery R-37, H and Area G at Harappa, Robbins Schug et al. (2013) identified the paleopathological signs of non-specific periosteal reactions, maxillary infections, and specific infections such as leprosy and/or tuberculosis. Lovell (2014) reported that the frequency of non-specific infectious disease, indicated by periosteal lesions, was low. Meanwhile, by the late Harappan phase, the osteological signs of leprosy and tuberculosis reached as high as 15.4% of the individuals buried at Cemetery H, and 21.7% (only leprosy) of Area G cases. The previous researchers argued that the infection rate of the Harappan people might have varied through time, closely tracking the changes in social, economic, and environmental stresses. In our Rakhigarhi samples, two individuals (7.2 A2 BR-9 and 7.2 A1 BR-02) demonstrated periosteal reactions of slight pitting with surface striation on tibias, a possible sign of chronic infectious disease. Of these two, 7.2 A2 BR09 exhibited a periosteal reaction on the medial surface of the midshaft portion of the right tibia, while 7.2 A1 BR02 showed the same reactions on the posteromedial surfaces on both tibia. The femur diaphysis of 7.2 A1 BR02 also displayed evidence of osteomyelitis in the right femur (Figure 5). Serial CT images showed a radio-opaque area in the medial portion of the left femoral diaphysis. Obviously, new bone formation tends to enclose the infected area caused by osteomyelitis (Mast and Horwitz, 2002). As a serious health problem, osteomyelitis is defined as an infection of the bone and bone marrow resulting in inflammation, necrosis, and new bone formation, and is commonly observed from the pre-antibiotic era (Santos and Suby, 2015). However, the poor preservation condition of this case did not allow us to definitively diagnose whether the femoral osteomyelitis was a non-hematogenous or hematogenous type of osteomyelitis. Moreover, it is hard to diagnose which pathogens infect the archeological skeleton.
Osteoarthritis is one of the most commonly observed pathological conditions in the postcranial remains from the Indus civilization (Lovell, 2016). The knee was identified as the joint most affected by arthritic changes among the skeletons from Harappa (Lovell, 2014). In a previous study, the unusual involvement of arthritis was also found in the cervical spine of Harappan people, which might be related to carrying loads on the head, a common practice in South Asia even today (Lovell, 1994). In the present study, some parts of the postcranial skeleton, such as the knee, ankle, and vertebral joints of three individuals, exhibited evidence of osteoarthritis. A femoral condyle with moderate lipping was seen on an individual (7.2 A2 BR-18-2). Vertebral osteoarthritis was also identified on a single individual (7.2 A2 BR31). Severe osteophytes in the ankle joint were found in an adult young male (7.3 B1 BR01A) (Figure 6). Lastly, the current research found no evidence of trauma, including injury.

Conclusion
We examined the human skeletal series from Rakhigarhi cemetery to assess the physical and pathological traits of people from the mature Harappan period. Overall, the Harappan inhabitants of Rakhigarhi in this study seem to have been in general healthy. Some of our results accord well with previous reports (Nath et al., 2015; Lovell, 2016). Our investigation of Rakhigarhi cemetery provides invaluable information to unravel the health and disease conditions of the Harappan people. Ultimately, however, as only a small number of Harappan skeletons were recovered from these burial sites and have been examined so far, we must also consider that a wider area of this cemetery remains to be investigated further. To attain a level of knowledge that offers us a holistic understanding of the various aspects of Harappan society, additional bioarchaeological studies should be undertaken at other Rakhigarhi cemetery and grave sites in the future.
Appendix
Appendix 1
Calculation of diaphyseal shape indices in the femur
| Index |
Region |
Description |
| Femur platymeric |
Subtrochanter |
(Subtrochanteric anteroposterior diameter/Subtrochangeric mediolateral diameter) × 100 |
| Femur pilasteric |
Midshaft |
(Anteroposterior midshaft diameter/Mediolateral midshaft diameter) × 100 |
Acknowledgments
This study was supported in part by a grant from the National Geographic Society (Asia 21-15), and Seoul National University Research Grant in 2015.
References
- Buikstra J.E. and Ubelaker D.H. (1994) Standards for data collection from human skeletal remains: Proceedings of a Seminar at the Field Museum of Natural History, organized by Jonathan Haas. Arkansas Archaeological Survey Research Series, No. 44. Arkansas Archaeological Survey, Fayetteville. pp. 16–21.
- Dibyopama A., Kim Y.J., Oh C.S., Shin D.H., and Shinde V. (2015) Human skeletal remains from ancient burial sites in India: with special reference to Harappan civilization. Korean Journal of Physical Anthropology, 28: 1–9.
- Hemphill B.E., Lukacs J.R., and Kennedy K.A.R. (1991) Biological adaptations and affinities of Bronze Age Harappans. In: Meadow R.H. (ed.), Harappa Excavations 1986–1990: A Multidisciplinary Approach to Third Millennium Urbanism. Prehistory Press, Madison, pp. 137–182.
- Kennedy K.A.R. (1995) Have Aryans been identified in the prehistoric skeletal record from South Asia? Biological anthropology and concepts of ancient races. In: Erdosy G. (ed.), The Indo-Aryans of Ancient South Asia: Language, Material Culture and Ethnicity. Walter de Gruyter, Berlin, pp. 32–66.
- Kennedy K.A.R. (2000) God-Apes and Fossil Men: Paleoanthropology of South Asia. University of Michigan Press, Ann Arbor.
- Kenoyer J.M. (1998) Ancient Cities of the Indus Valley Civilization. Oxford University Press, Karachi.
- Larsen C.S. (1987) Bioarchaeological interpretations of subsistence economy and behavior from human skeletal remains. Advances in Archaeological Method and Theory, 10: 339–445.
- Liebenberg L., Stull K.E., L’Abbé E.N., and Botha D. (2015) Evaluating the accuracy of cranial indices in ancestry estimation among South African groups. Journal of Forensic Sciences, 60: 1277–1282.
- Lovell N.C. (1994) Spinal arthritis and physical stress at Bronze Age Harappa. American Journal of Physical Anthropology, 93: 149–164.
- Lovell N.C. (2014) Skeletal paleopathology of human remains from cemetery R37 at Harappa, excavated in 1987 and 1988. University of Alberta Education and Research Archive. doi:10.7939/R3125QG92.
- Lovell N.C. (2016) Bioarchaeology of the Indus Valley civilization: biological affinities, paleopathology, and chemical analyses. In: Robbins Schug G. and Walimbe S.R. (eds.), A Companion to South Asia in the Past. Wiley-Blackwell, Hoboken, pp. 169–186.
- Lovell N.C. and Whyte I. (1999) Patterns of dental defects at ancient Mendes, Egypt. American Journal of Physical Anthropology, 110: 69–80.
- Lukacs J.R. (1991) Localized enamel hypoplasia of human deciduous canine teeth: prevalence and pattern of expression in rural Pakistan. Human Biology, 63: 513–522.
- Lukacs J.R. (1998) Physiological stress in prehistoric India: new data on localized hypoplasia of primary canines linked to climate and subsistence change. Journal of Archaeological Science, 25: 571–585.
- Lukacs J.R. (2017) Dental adaptations of Bronze age Harappans: occlusal wear, crown size, and dental pathology. International Journal of Paleopathology, 18: 69–81.
- Lukacs J.R. and Hemphill B.E. (1990) Traumatic injuries of prehistoric teeth: new evidence from Baluchistan and Punjab provinces, Pakistan. Anthropologischer Anzeiger, 48: 351–363.
- Lukacs J.R. and Hemphill B.E. (1991) Dental anthropology of prehistoric Baluchistan: a morphometric approach to the peopling of south Asia. In: Kelley M.A. and Larsen C.S. (eds.), Advances in Dental Anthropology. Wiley-Liss, New York, pp. 77–119.
- Lukacs J.R. and Pal J.N. (1993) Mesolithic subsistence in north India: inferences from dental attributes. Current Anthropology, 34: 745–765.
- Lukacs J.R. and Pastor R.F. (1988) Activity-induced patterns of dental abrasion in prehistoric Pakistan: evidence from Mehrgarh and Harappa. American Journal of Physical Anthropology, 76: 377–398.
- Martin R. and Knussmann R. (1988) Anthropologie. Handbuch Der Vergleichenden Biologie des Menschen, Band, I. Gustav Fischer Verlag, Stuttgart.
- Mast N.H. and Horwitz D. (2002) Osteomyelitis: a review of current literature and concepts. Operative Techniques in Orthopaedics, 12: 232–241.
- Meadow R.H. (1991) Harappa Excavations 1986–1990: A Multidisciplinary Approach to Third Millennium Urbanism. Prehistory Press, Madison.
- Morrison J.B. (1970) The mechanics of the knee joint in relation to normal walking. Journal of Biomechanics, 3: 51–61.
- Mushrif-Tripathy V. (2014) Human skeletal studies in India: a review. In: O’Donnabhain B. and Lozada M.C. (eds.), Archaeological Human Remains: Global Perspectives. Springer, Cham, pp. 139–153.
- Nath A., Walimbe S.R., Garge T.M., Mushrif-Tripathy V., Dehuri R., and Malik A. (2015) Harappan interments at Rakhigarhi, Haryana. Man and Environment, XL: 9–32.
- Pomeroy E. and Zakrzewski S.R. (2009) Sexual dimorphism in diaphyseal cross-sectional shape in the medieval Muslim population of Écija, Spain, and Anglo-Saxon Great Chesterford, UK. International Journal of Osteoarchaeology, 19: 50–65.
- Possehl G.L. (1993) The Harappan civilization: a contemporary perspective. In: Possehl G.L. (ed.), Harappan Civilization: A Contemporary Perspective, Aris and Philips, Warminster, pp. 15–28.
- Robbins G., Mushrif Tripathy V., Misra V.N., Mohanty R.K., Shinde V.S., Gray K.M., and Schug M.D. (2009) Ancient skeletal evidence for leprosy in India (2000 B.C.). PLoS ONE, 4: e5669.
- Robbins Schug G. (2017) A Hierarchy of Values: The bioarchaeology of complexity, order, health, and hierarchy at Harappa. In: Klaus H., Harvey A.R., and Cohen M.N. (eds.), Bones of Complexity: Osteological Indicators of Emergent Heterarchy and Hierarchy. University Press of Florida, Gainesville, pp. 263–289.
- Robbins Schug G., Gray K., Mushrif-Tripathy V., and Sankhyan A.R. (2012) A peaceful realm? Trauma and social differentiation at Harappa. International Journal of Paleopathology, 2: 136–147.
- Robbins Schug G., Blevins K.E., Cox B., Gray K., and Mushrif-Tripathy V. (2013) Infection, disease, and biosocial processes at the end of the Indus civilization. PLoS ONE, 8: e84814.
- Ruff C.B. (1987) Sexual dimorphism in human lower limb bone structure: relationship to subsistence strategy and sexual division of labor. Journal of Human Evolution, 16: 391–416.
- Santos A.L. and Suby J.A. (2015) Skeletal and surgical evidence for acute osteomyelitis in non-adult individuals. International Journal of Osteoarchaeology, 25: 110–118.
- Shinde V. (2016) Current perspectives on the Harappan civilization. In: Robbins Schug G. and Walimbe S.R. (eds.), A Companion to South Asia in the Past. Wiley-Blackwell, Hoboken, pp. 127–144.
- Shinde V., Jadhav N., and Shastri R. (2015) Field Based Research at Rakhigarhi, the Harappan Metropolis in Haryana 2012 to 2015: A Preliminary Report. Deccan College Post-Graduate and Research Institute Deemed University Pune and Department of Archaeology and Museums, Haryana Government, Chandigarh.
- Shinde V.S., Kim Y.J., Woo E.J., Jadhav N., Waghmare P., Yadav Y., Munshi A., Chatterjee M., Panyam A., Hong J.H., Oh C.S., and Shin D.H. (2018) Archaeological and anthropological studies on the Harappan cemetery of Rakhigarhi, India. PLoS ONE, 13: e0192299.
- Skinner M. (1996) Developmental stress in immature hominines from Late Pleistocene Eurasia: evidence from enamel hypoplasia. Journal of Archaeological Science, 23: 833–852.
- Stock J.T. and Pfeiffer S. (2004) Long bone robusticity and subsistence behavior among Late Stone Age foragers of the forest and fynbos biomes of South Africa. Journal of Archaeological Science, 31: 999–1013.
- Stock J.T. and Shaw C.N. (2007) Which measures of diaphyseal robusticity are robust? A comparison of external methods of quantifying the strength of long bone diaphysis to cross-sectional geometric properties. American Journal of Physical Anthropology, 134: 412–423.
- Tallman S.D. and Winburn A.P. (2015) Forensic applicability of femur subtrochanteric shape to ancestry assessment in Thai and White American males. Journal of Forensic Sciences, 60: 1283–1289.
- Trotter M. and Gleser G.C. (1958) A re-evaluation of estimation of stature based on measurements of stature taken during life and of long bones after death. American Journal of Physical Anthropology, 16: 79–123.
- Ubelaker D.H. (1999) Human Skeletal Remains: Excavation, Analysis, Interpretation. Taraxacum, Washington, D.C.
- Vahia M.N., Kumar P., Bhogale A., Kothari D.C., Chopra S., Shinde V., Jadhav N., and Shastri R. (2016) Radiocarbon dating of charcoal samples from Rakhigarhi, Haryana, India using accelerator mass spectrometer. Current Science, 111: 27–28.
- Valentine B., Kamenov G.D., Kenoyer J.M., Shinde V., Mushrif-Tripathy V., Otarola-Castillo E., and Krigbaum J. (2015) Evidence for patterns of selective urban migration in the Greater Indus Valley (2600–1900 BC): a lead and strontium isotope mortuary analysis. PLoS ONE, 10: e0123103.
- Walimbe S.R. (2007) Population movements in the Indian subcontinent during the protohistoric period: physical anthropological assessment. In: Petraglia M.D. and Allchin B. (eds.), The Evolution and History of Human Populations in South Asia: Inter-Disciplinary Studies in Archaeology, Biological Anthropology, Linguistics and Genetics. Springer, Dordrecht, pp. 297–319.
- Walimbe S.R. (2014) The Harappan civilization and human skeletal biology. In: Chakrabarti D.K. and Lal M. (eds.), A Fresh Look at the History of Ancient India, Vol. 2: Protohistoric Foundations. Vivekananda International Foundation, New Delhi, pp. 243–332.
- Walimbe S.R. (2016) Human skeletal studies: Changing trends in theoretical and methodological perspectives. In: Robbins Schug G. and Walimbe S.R. (eds.), A Companion to South Asia in the Past. Wiley-Blackwell, Hoboken, pp. 482–295.
- Walimbe S.R. and Tavares A. (2002) Human Skeletal Biology: Scope, Development and Present Status of Research in India. In: Paddayya K. (ed.), Recent Studies in Indian Archaeology, Indian Council of Historical Research, Monograph Series 6. Munshiram Manoharlal, New Delhi, pp. 367–402.
- Wescott D. (2005) Population variation in femur subtrochanteric shape. Journal of Forensic Sciences, 50: 286–293.