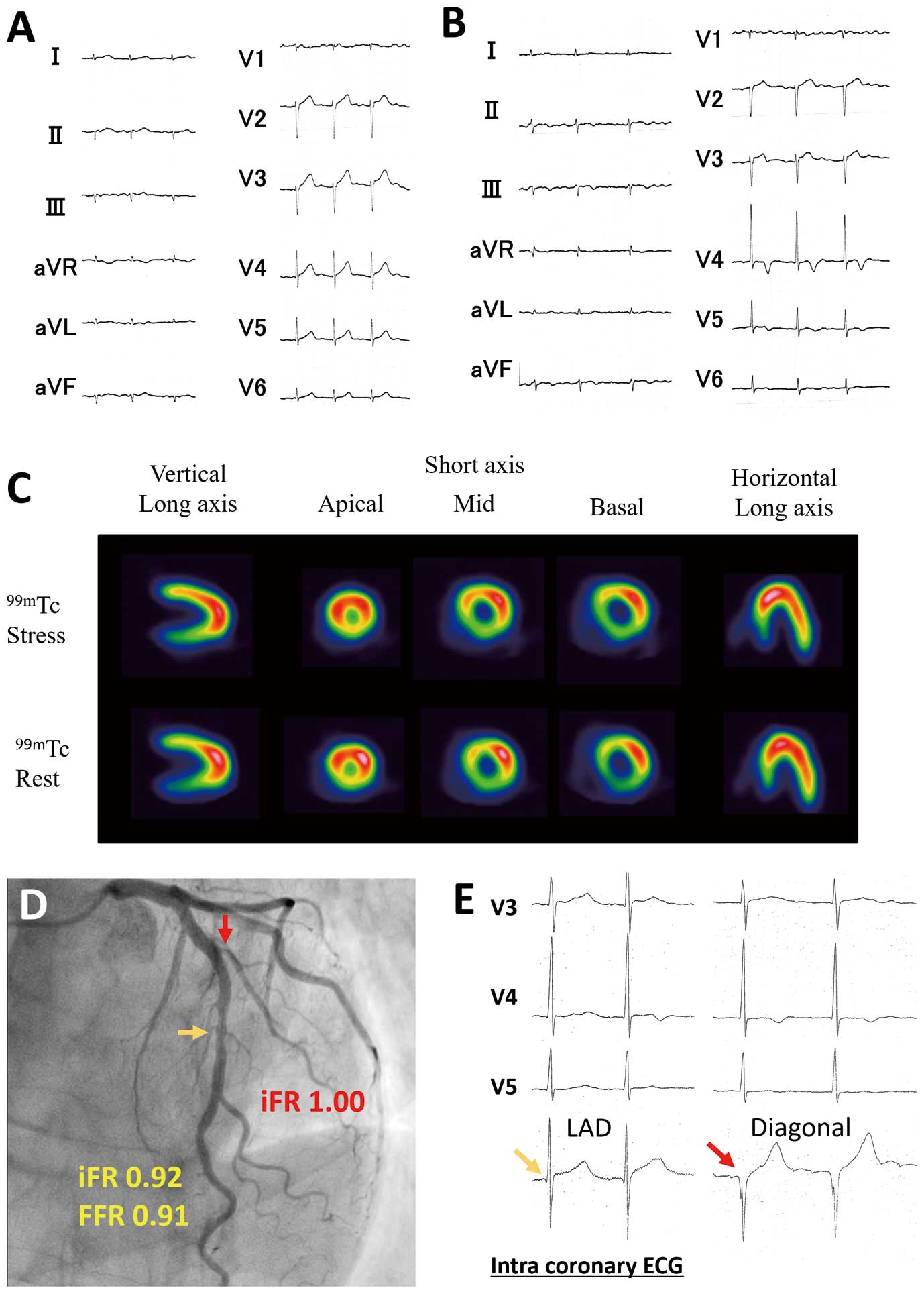
A 70-year-old man, being treated for dyslipidemia and paroxysmal atrial fibrillation, presented with a negative T wave on V4-5 induction on electrocardiogram (ECG) at his annual general checkup, despite never feeling any chest pain (Figure A,B). Echocardiogram highlighted severe hypokinesis with partially reduced anterior wall thickness, high echo density, and absence of left ventricular hypertrophy. On stress myocardial scintigraphy the perfusion defect was more evident on the rest image in the middle of the anterior wall, indicating the occurrence of reperfusion after myocardial infarction (MI;
Figure C). The following coronary angiography showed intermediate stenosis in the midportion of the left anterior descending (LAD) artery, and severe stenosis in the ostium of the first diagonal artery (D1). The infarct-related coronary artery could not be identified because the lateral wall was perfused by the high lateral branch. Physiological measurements of both the LAD and D1 were negative in the diagnosis of myocardial ischemia (LAD: instantaneous wave free ratio [iFR], 0.92; fractional flow reserve [FFR], 0.91; D1: iFR, 1.00;
Figure D). To assess local ECG abnormalities, an intracoronary ECG (icECG) was recorded by connecting an electrode to the pressure wire. This study was approved by the institute. On icECG an abnormal Q wave was noted solely in the D1, indicating that a lesion in the D1 was responsible for the asymptomatic MI (Figure E). Increase in FFR and iFR after MI complicated the evaluation of myocardial viability. icECG contributed to identification of the cause of the MI in the D1 region and proper selection of pharmacological therapy without intervention for this patient. The combined use of FFR and icECG might be helpful to identify the reperfused culprit lesion without additional use of myocardial scintigraphy.
Disclosures
The authors declare no conflicts of interest.
