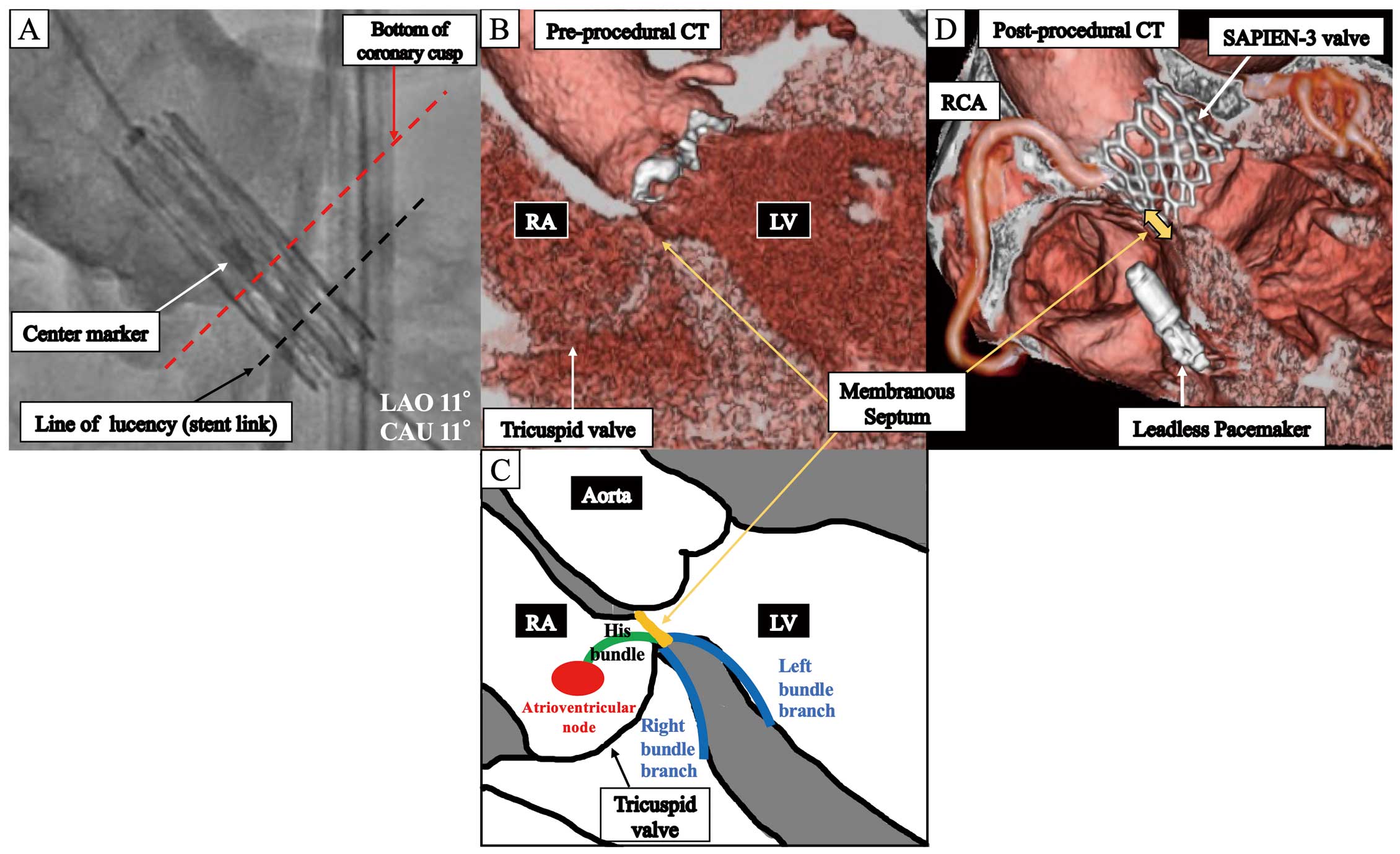
A 92-year-old woman with severe aortic stenosis was admitted for transcatheter aortic valve implantation (TAVI). She had no electrocardiogram abnormalities, such as right bundle branch block or atrioventricular block (AVB). A 26-mm SAPIEN-3 valve (Edwards Lifesciences, Irvine, CA, USA) was deployed by the traditional method using a center marker (Figure A) with 2 mL less than nominal volume because the annulus area (473.8 mm2) was smaller than a 26-mm valve (519 mm2). After TAVI, new left bundle branch block and first-degree AVB emerged, which developed into advanced AVB on postoperative day 5. Finally, a leadless pacemaker was implanted before discharge. We retrospectively evaluated pre- and post-operative computed tomography (CT) images, which revealed that the valve edge overlapped with the membranous septum (MS;
Figure B,D). The bundle of His runs along the lower end of the MS (Figure C). Therefore, we assumed that mechanical injury caused by the valve was responsible for the conduction disturbance. It has been reported that an MS length <5 mm (in this case, 3.1 mm) is a risk factor for pacemaker implantation.1
In the high implantation technique, the line of lucency (Figure A, black line) is aligned to the bottom of the non-coronary cusp, not the center marker, which may minimize the risk of pacemaker implantation.1
Reference
- 1.
Ramanathan PK, Nazir S, Elzanaty AM, Nesheiwat Z, Mahmood M, Rachwal W, et al. Novel method for implantation of balloon expandable transcatheter aortic valve replacement to reduce pacemaker rate: Line of lucency method. Structural Heart 2020; 4: 427–432.
