Images in Cardiovascular Medicine
Histopathological Findings of Pulmonary Hypertension With Elevated Pulmonary Arterial Wedge Pressure in Hereditary Hemorrhagic Telangiectasia
2022 年 4 巻 6 号 p. 287-288

詳細
2022 年 4 巻 6 号 p. 287-288
Pulmonary hypertension (PH) with elevated pulmonary arterial wedge pressure (PAWP) is defined as PH associated with left heart disease (PH-LHD), in which chronic pulmonary venous hypertension may cause remodeling of pulmonary veins and arterioles.1
A 64-year-old woman with hereditary hemorrhagic telangiectasia (HHT) was admitted for the treatment of progressive PH with elevated PAWP and a high cardiac output state induced by hepatic arteriovenous malformations over 5 years. Echocardiography detected atrial dilatation, as well as right ventricular dilation and dysfunction (Figure A,B). Right heart catheterization revealed a cardiac index of 4.05 L/min/m2, mean pulmonary arterial pressure (PAP) of 56 mmHg, PAWP of 25 mmHg, right atrial pressure of 28 mmHg, and pulmonary vascular resistance of 5.0 Wood units (Figure I). On the ninth hospital day, the patient suddenly developed hemoptysis and died.
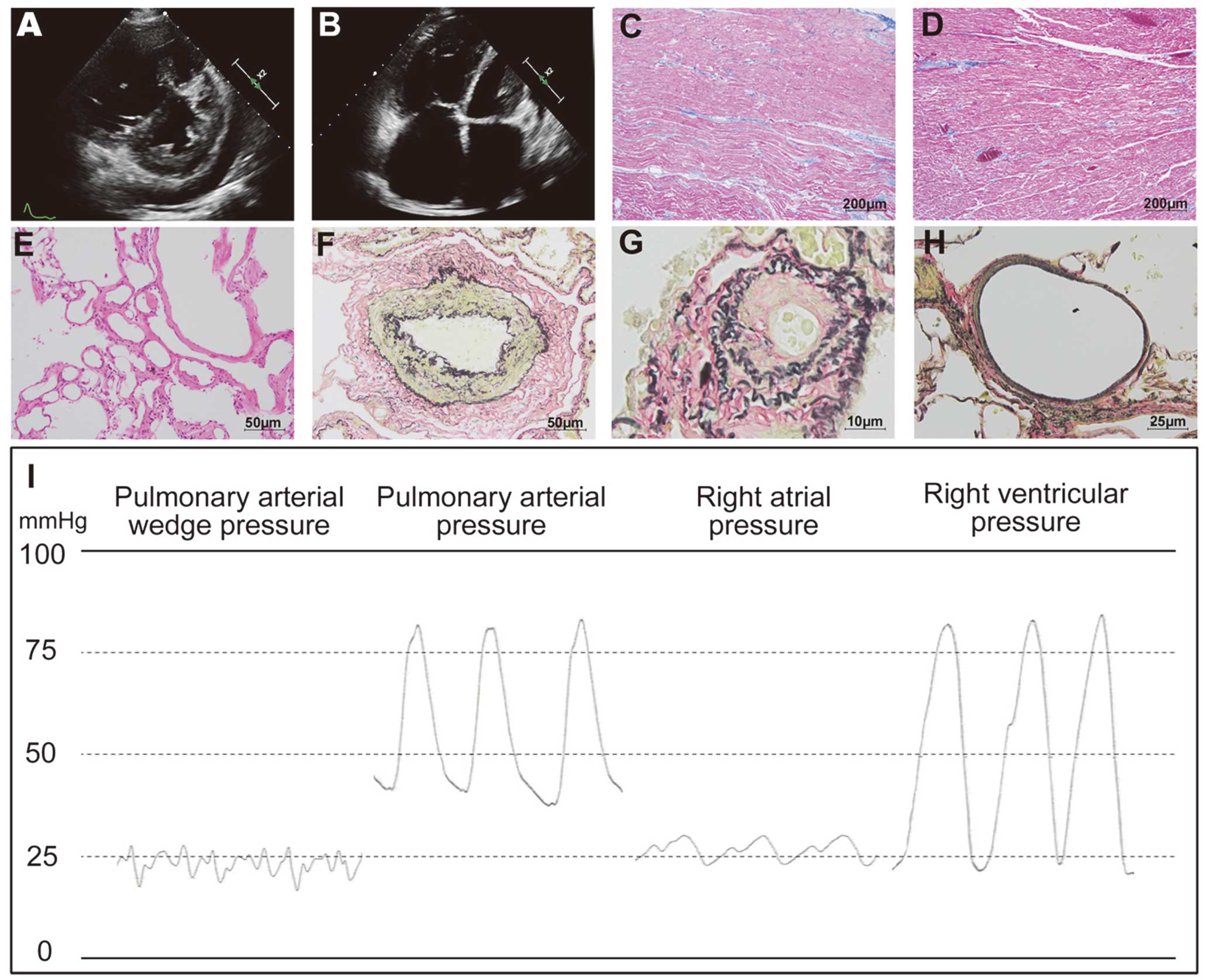
(A,B) Echocardiography, (C–H) histopathological staining, and (I) intracardiac pressures on right heart catheterization. (C,D) Masson’s trichrome staining of the right (C) and left (D) ventricles. (E) Hematoxylin-eosin staining of the lung. (F–H) Elastica van Gieson staining of the pulmonary artery (F), pulmonary arteriole (G), and pulmonary venule (H).
On autopsy, myocardial fibrosis of both ventricles was mild (Figure C,D). Abnormal dilated vessels were found in the lung that were compatible with the pathology of HHT (Figure E). Medial and intimal thickening was found in the pulmonary arteries and arterioles (Figure F,G). Notably, almost no remodeling of the pulmonary veins or venules was observed (Figure H), which is not consistent with the pathological characteristics of PH-LHD. Thus, the increased PAP and volume overload due to the high cardiac output state may have caused severe right ventricular dilatation and dysfunction, as well as mild pulmonary arterial remodeling. In addition, the finding of high PAWP, similar to the patient’s right atrial pressure, was attributed mainly to the pericardial constraint and interventricular interaction. Therefore, PH with equalized high diastolic chamber pressures may occur with no remodeling of the pulmonary veins or venules.
None.