Abstract
Background: Although accurate assessment of right ventricular (RV) morphology and function is clinically important, data regarding reference values for echocardiographic measurements of the right ventricle in the Japanese population are limited.
Methods and Results: The World Alliance Society of Echocardiography (WASE) Normal Values Study was conducted to examine normal echocardiographic values in 15 countries. Using the WASE study database, we analyzed 2-dimensional echocardiographic parameters of RV size and systolic function in 192 healthy Japanese individuals and compared them with those obtained from 153 healthy American individuals. In the Japanese population, the absolute values of RV dimensions were smaller for women than men, although the difference disappeared after the data were adjusted for body surface area. RV dimensions, RV length and RV area were smaller in the elderly, but age did not affect RV systolic function. The absolute value, but not the adjusted value, of RV size tended to be smaller in Japanese than American individuals for both sexes. For men, RV systolic function parameters were lower in the Japanese population. This trend was not seen in women.
Conclusions: The present study identified normal reference values for RV size and systolic function in a healthy Japanese population. Sex, age, and race had a significant impact on RV size; however, this trend was weak for RV systolic function.
Quantification of cardiac chamber size and function is essential in clinical practice, and transthoracic echocardiography is a simple, non-invasive tool used for this purpose. Although sex and racial differences in the context of cardiovascular diseases have been reported, limited data are available on normal echocardiographic values of cardiac morphology and function in Japanese individuals.1,2 Because the Japanese population is characterized by a smaller body size compared with Westerners, cut-off values in Western guidelines do not apply.3 Indeed, multinational studies have shown that cardiac chamber sizes differ among ethnicities.4 Previously, the Japanese Normal Values for Echocardiographic Measurements Project (JAMP), a multicenter prospective study, examined the normal values of echocardiographic measurements in a large healthy Japanese population.5,6 However, echocardiographic measurements were performed at individual local facilities, so it is possible that measurement bias among facilities may have impacted the results. This limitation was overcome by the World Alliance Societies of Echocardiography (WASE) study, because all analyses of echocardiographic images were performed in a core laboratory.4 In the WASE study, 2,262 individuals free of known cardiac and lung disease were prospectively enrolled at centers in 15 countries, including 230 Japanese individuals and 172 American individuals.
Recently, echocardiographic assessment of right ventricular (RV) remodeling has gained increasing attention in clinical practice because it can provide additive prognostic value over left ventricular morphology and function in various heart diseases.7,8 The WASE study investigated normal values of RV geometries and function stratified by sex, age, and ethnicity in 1,913 subjects and found that normal values of RV size and function differed by sex and age and that the Asian population had a smaller RV chamber size compared with White and Black population.9 Conversely, it is important to note that the Asian category in the WASE study encompassed a diverse range of ethnic groups, including individuals from India, China, Japan, Korea, the Philippines, and Iran. For the purpose of Japanese clinical practice, it is essential to first understand the differences between Japanese and Western cohorts, especially because existing guidelines are primarily based on Western data. However, the WASE study did not identify reference values for RV measurements obtained by 2-dimensional (2D) echocardiography in the Japanese population.4
The aims of the present study were to: (1) determine the normal 2D echocardiographic values of RV size and systolic function by sex and age in a Japanese population; and (2) to compare these values to those from American individuals included in the WASE study database.
Methods
Study Population
The WASE study is a multicenter international observational prospective cross-sectional study to establish normal echocardiography values for chamber size and function across different countries, races, and ethnicities worldwide. Details of the WASE study design and inclusion and exclusion criteria have been published elsewhere.10 Healthy adults (aged ≥18 years) without histories of cardiac, lung, and kidney diseases were stratified according to age (young, 18–40 years; middle aged, 41–65 years; elderly, >65 years) and sex. In all, 230 healthy Japanese adults and 172 healthy Americans were enrolled between 2016 and 2019. In the Japanese population, 1 subject was excluded because they lacked basic demographic information, and 37 subjects were excluded because of inadequate image quality or incomplete assessment of echocardiographic examinations. Similarly, 19 American subjects were excluded. Thus, our final analysis population consisted of 192 Japanese subjects and 153 American subjects.
This study was approved by the Institutional Ethics Committee of the University of Tokyo (IRB no. 11345). Written informed consent was obtained from all study participants.
Echocardiographic Examination
Comprehensive transthoracic echocardiography was performed with a commercially available system (Phillips, Siemens, or GE) by a physician or specialized technician following the WASE study-specific imaging protocol.10 All digital images were transferred to the echocardiography core laboratory (MedStar Health Research Institute, Washington, DC, USA) for analysis. All measurements were analyzed with a vender-neutral workstation (Image Arena; Tomtec, Unterschleissheim, Germany) following the American Society of Echocardiography (ASE)/European Association of Cardiovascular Imaging (EACVI) guideline.11 In this analysis, we focus on RV size and systolic function. Assessment of RV size was performed by measuring the RV end-diastolic area, RV end-systolic area, RV basal, mid, and length dimensions, as obtained from the apical RV-focused 4-chamber view. To evaluate RV systolic function, the RV fractional area change (RVFAC) was calculated using the following formula:
RVFAC = (RV end-diastolic area − RV end-systolic area) / RV end-diastolic area × 100
The tricuspid annular plane systolic excursion (TAPSE) was recorded with M-mode echocardiography through the lateral tricuspid annulus by calculating the amount of longitudinal motion of the annulus at peak systole, and peak systolic tissue Doppler velocity at the tricuspid annulus (RV S′) was also obtained. The echocardiographic measurements of the RV used in this study have been published previously.9
Statistical Analysis
Continuous variables are presented as the mean±SD, and categorical variables are presented as number and frequency (%). Group differences were evaluated with an unpaired two-tailed t-test to compare RV parameters between men and women and between Japanese and American subjects. Two-way analysis of variance (ANOVA) was used to assess differences in RV parameters among age groups. We used JMP 16 software (SAS Institute, Cary, NC, USA) for the analysis, and P<0.05 was considered statistically significant.
Results
Baseline Characteristics of the Study Population
The clinical characteristics of the study population are summarized in Table 1. Among Japanese individuals, the mean age was 48 years, 99 (52%) participants were male, and 100% were Asian. Among American subjects, the mean age was 47 years, 78 (51%) participants were male, 55% were White, and 45% were Black. The mean body surface area (BSA) was 1.6±0.2 m2
in Japanese individuals and 1.9±0.2 m2
in American individuals.
Table 1.
Characteristics of the Study Population
| |
Japanese |
American |
All subjects
(n=192) |
Men
(n=99) |
Women
(n=93) |
P value |
All subjects
(n=153) |
Men
(n=78) |
Women
(n=75) |
P value |
| Age (years) |
48±18 |
48±18 |
47±18 |
|
47±17 |
47±18 |
47±16 |
|
| Height (cm) |
164±8 |
170±5 |
157±6* |
<0.001 |
172±10 |
179±7 |
164±6* |
<0.001 |
| Weight (kg) |
59±10 |
65±8 |
53±8* |
<0.001 |
77±16 |
84±16 |
70±13* |
<0.001 |
| Body surface area (m2) |
1.6±0.2 |
1.7±0.1 |
1.5±0.1* |
<0.001 |
1.9±0.2 |
2.0±0.2 |
1.8±0.2* |
<0.001 |
| Heart rate (beats/min) |
64±10 |
62±10 |
65±10* |
0.014 |
66±11 |
63±11 |
69±11* |
0.004 |
| Systolic blood pressure (mmHg) |
126±11 |
128±10 |
124±12* |
0.016 |
122±13 |
124±13 |
120±12 |
|
| Diastolic blood pressure (mmHg) |
74±9 |
75±8 |
73±9 |
|
72±8 |
71±8 |
73±9 |
|
Unless indicated otherwise, data are given as the mean±SD. *P<0.05 compared with men.
Sex- and Age-Related Differences in Normal Values of RV Size and Function
Table 2 shows sex differences in RV size and function in the Japanese population. Women had smaller absolute values of RV dimensions, although the difference disappeared after the data were adjusted for BSA. In contrast, the absolute value of RV length was greater in men, whereas the BSA-adjusted RV length was larger in women. RV areas were greater in men, and that tendency persisted even after the data were adjusted for BSA. In terms of RV systolic functional parameters, including RVFAC, TAPSE and RV S′, there were no significant gender differences.
Table 2.
RV Size and Function Measurements in Japanese Men and Women Separately
| |
All subjects
(n=192) |
Men
(n=99) |
Women
(n=93) |
P value |
| RV base (mm) |
32.4±4.8 |
34.2±4.6 |
30.4±4.3* |
<0.001 |
| RV base/BSA (mm/m2) |
19.9±2.7 |
19.6±2.6 |
20.1±2.7 |
|
| RV mid (mm) |
25.5±5.1 |
27.2±5.1 |
23.7±4.6* |
<0.001 |
| RV mid/BSA (mm/m2) |
15.6±3.0 |
15.6±3.0 |
15.7±3.0 |
|
| RV length (mm) |
72.5±7.5 |
75.5±7.0 |
69.3±6.6* |
<0.001 |
| RV length/BSA (mm/m2) |
44.5±4.5 |
43.3±4.1 |
45.8±4.6* |
<0.001 |
| RVAd (cm2) |
16.2±3.5 |
17.8±3.1 |
14.5±3.1* |
<0.001 |
| RVAdi (cm2/m2) |
9.9±1.8 |
10.2±1.7 |
9.5±1.8* |
0.010 |
| RVAs (cm2) |
9.2±2.2 |
10.2±2.0 |
8.2±1.8* |
<0.001 |
| RVAsi (cm2/m2) |
5.6±1.1 |
5.9±1.1 |
5.4±1.0* |
0.002 |
| RVFAC (%) |
42.9±4.2 |
42.5±4.0 |
43.4±4.4 |
|
| TAPSE (mm) |
22.5±3.7 |
22.1±3.4 |
23.0±3.9 |
|
| RV S′ (cm/s) |
13.4±2.7 |
13.5±2.7 |
13.3±2.6 |
|
Unless indicated otherwise, data are given as the mean±SD. *P<0.05 compared with men. BSA, body surface area; RV, right ventricle; RVFAC, RV fractional area change; RVAd, RV area in end-diastole; RVAdi, RV area in end-diastole indexed to BSA; RVAs, RV area in end-systole; RVAsi, RV area in end-systole indexed to BSA; TAPSE, tricuspid annular plane systolic excursion.
Echocardiographic parameters stratified by age group are presented in Table 3. Absolute as well as BSA-adjusted RV size tended to be smaller with increasing age, whereas RVFAC and TAPSE did not differ across the 3 age groups. Only RV S′ differed between younger and middle age.
Table 3.
Age Dependency of RV Size and Function Measurements in All Japanese Individuals (n=192)
| |
Age group (years) |
| 18–40 (n=80) |
41–65 (n=65) |
>65 (n=47) |
P valueA |
| RV base (mm) |
32.3±4.7 |
33.3±5.4 |
31.2±4.1† |
|
| RV base/BSA (mm/m2) |
19.9±2.4 |
19.9±3.0 |
19.7±2.6 |
|
| RV mid (mm) |
27.0±5.4 |
24.9±4.7* |
23.8±4.6* |
0.0017 |
| RV mid/BSA (mm/m2) |
16.6±3.1 |
14.9±2.8* |
15.0±2.5* |
0.0003 |
| RV length (mm) |
73.7±7.7 |
72.9±7.5 |
69.8±6.5*,† |
0.014 |
| RV length/BSA (mm/m2) |
45.6±4.5 |
43.5±4.5* |
44.1±4.3 |
0.018 |
| RVAd (cm2) |
16.9±3.7 |
16.5±3.6 |
14.5±2.6*,† |
0.0005 |
| RVAdi (cm2/m2) |
10.4±1.8 |
9.8±1.8* |
9.1±1.2*,† |
0.0003 |
| RVAs (cm2) |
9.6±2.3 |
9.5±2.3 |
8.3±1.7*,† |
0.0030 |
| RVAsi (cm2/m2) |
5.9±1.1 |
5.6±1.2 |
5.2±0.8* |
0.0031 |
| RVFAC (%) |
43.3±4.5 |
42.6±4.1 |
42.8±3.8 |
|
| TAPSE (mm) |
22.6±3.7 |
22.6±3.5 |
22.3±3.9 |
|
| RV S′ (cm/s) |
13.9±2.9 |
12.9±2.0* |
13.1±3.0 |
|
Unless indicated otherwise, data are given as the mean±SD. AP values for 3-way analysis of variance. *P<0.05 compared with the 18–40-year age group; †P<0.05 compared with the 41–65-year age group. Abbreviations as in Table 2.
Comparison of RV Size and Function Between Japanese and American Subjects
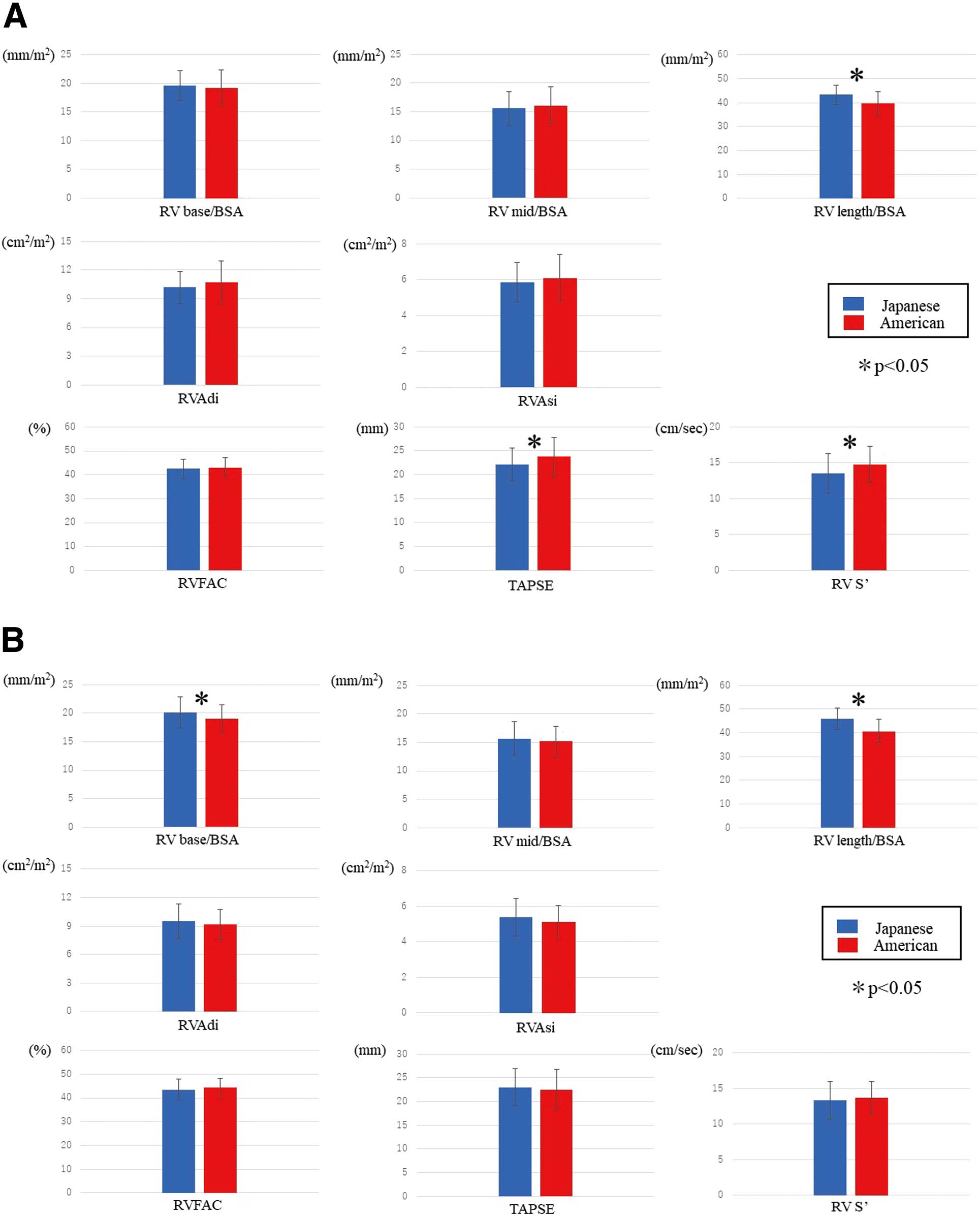
Table 4 presents RV size and function by race. For both men and women, the absolute values of RV size were smaller in Japanese than American subjects. Because of the smaller BSA in Japanese subjects, the adjusted values of RV basal and mid dimensions and RV area did not differ between Japanese and American men. In women, the adjusted values of RV mid dimension and RV area were not significantly different between Japanese and American subjects. The adjusted value of RV length was smaller in American than Japanese individuals of both sexes (Figure). In men, RV systolic parameters such as TAPSE and RV S′ were lower in Japanese than American individuals; however, there was no significant difference in RVFAC between the 2 groups. In women, there were no significant differences in any RV systolic functional parameters between Japanese and American individuals.
Table 4.
RV Size and Functional Measurements for Men and Women According to Race
| |
Men |
Women |
Japanese
(n=99) |
American
(n=78) |
P value |
Japanese
(n=93) |
American
(n=75) |
P value |
| RV base (mm) |
34.2±4.6 |
38.6±4.8 |
<0.001 |
30.4±4.3 |
33.6±3.9 |
<0.001 |
| RV base/BSA (mm/m2) |
19.6±2.6 |
19.2±3.1 |
|
20.1±2.7 |
18.9±2.5 |
0.0055 |
| RV mid (mm) |
27.2±5.1 |
32.4±5.8 |
<0.001 |
23.7±4.6 |
27.0±4.7 |
<0.001 |
| RV mid/BSA (mm/m2) |
15.6±3.0 |
16.1±3.2 |
|
15.7±3.0 |
15.2±2.7 |
|
| RV length (mm) |
75.5±7.0 |
80.2±8.2 |
<0.001 |
69.3±6.6 |
72.0±6.9 |
0.010 |
| RV length/BSA (mm/m2) |
43.3±4.1 |
39.8±4.8 |
<0.001 |
45.8±4.6 |
40.6±5.0 |
<0.001 |
| RVAd (cm2) |
17.8±3.1 |
21.6±4.5 |
<0.001 |
14.5±3.1 |
16.3±2.9 |
0.0001 |
| RVAdi (cm2/m2) |
10.2±1.7 |
10.7±2.3 |
|
9.5±1.8 |
9.2±1.6 |
|
| RVAs (cm2) |
10.2±2.0 |
12.4±2.8 |
<0.001 |
8.2±1.8 |
9.1±1.7 |
0.0013 |
| RVAsi (cm2/m2) |
5.9±1.1 |
6.1±1.3 |
|
5.4±1.0 |
5.1±0.9 |
|
| RV FAC (%) |
42.5±4.0 |
43.0±4.0 |
|
43.4±4.4 |
44.3±4.0 |
|
| TAPSE (mm) |
22.1±3.4 |
23.7±4.1 |
0.0042 |
23.0±3.9 |
22.5±4.3 |
|
| RV S′ (cm/s) |
13.5±2.7 |
14.7±2.6 |
0.0028 |
13.3±2.6 |
13.6±2.3 |
|
Unless indicated otherwise, data are expressed as the mean±SD. Abbreviations as in Table 2.
Discussion
We studied RV size and systolic functional parameters in a healthy Japanese population and compared them with those of American individuals in a subgroup analysis of the WASE study. In healthy Japanese individuals, RV dimensions, length, and area are larger in men than in women. In addition, RV size gradually decreases with age, and RV size is smaller in Japanese than American individuals. Furthermore, adjusted values for RV dimensions and area tended to be similar between Japanese and American individuals, except for RV length. Conversely, there were only tendencies for small or no differences in RV systolic functional parameters according to sex, age, and race. Normative data on echocardiographic measurements of cardiac structure and function are limited in Japanese individuals, as far as specific reference values, and their differences according to sex, age, and race. Previously, in the JAMP study, which enrolled 700 healthy Japanese volunteers, we reported that RV area decreased slightly with age, whereas RVFAC did not change with age.5 The present study is the first to determine RV diameters at the mid- and basal levels and RV length in a healthy Japanese population, whereas the JAMP study provided only RV diameter at the basal level. With regard to RV systolic function, this study is the first to determine TAPSE and RV S′, whereas the JAMP study analyzed only RVFAC. In addition, although our findings in a Japanese population are similar to those of the JAMP study, there are several differences between the 2 studies. For example, RV diastolic area (16±4 cm2
in men, 13±3 cm2
in women) and systolic area (9±3 cm2
in men, 7±2 cm2
in women) tended to be slightly smaller, and RVFAC tended to be larger (44±13% in men, 46±11% in women) in the JAMP study.5 This may be because in the JAMP study, quality control of the echocardiographic images was left to the local institutions, which may not have obtained appropriate RV-focused 4-chamber views, in addition to measurement bias between institutions. In the present study, sex- and age-related differences were not detectable in RV systolic parameters, whereas race affected TAPSE and RV S′ in men. Our findings are similar to those reported in the WASE study.9
Maffessanti et al investigated the effects of sex, age, and body size on RV volumes and RV ejection fraction (RVEF) using 3-dimensional (3D) echocardiography in a multicenter echocardiographic study involving 507 healthy volunteers in Italy.12 In that study, sex, age, and body size significantly influenced RV volumes and RVEF.12 This differs from the findings in our study; RVEF showed only a weak correlation with sex and age, and no correlation with body size. Similarly, the Multi-Ethnic Study of Atherosclerosis (MESA), a large population-based study, reported that sex, age, and race are associated with significant differences in RV mass, RV volumes, and RVEF measured by cardiac magnetic resonance (CMR) imaging.13 In that study, older age was associated with lower RV mass and higher RVEF. Men had greater RV mass and volumes than woman, but lower RVEF.13 Chinese Americans have lower RV mass than White individuals, but have higher RVEF.13 This differs from the findings in the present study, possibly because of differences in the method used to measure RV systolic function. Accurate determination of RVEF by echocardiography is still challenging because of the complex geometry of the RV, and CMR is considered the gold standard method to evaluate RVEF. Lee et al reported that RVFAC has a significantly higher correlation with CMR-derived RVEF compared with TAPSE (mean correlation coefficient [r] of 0.56 vs. 0.40), but its correlation was weak.14 Most recently, 3D speckle-tracking echocardiography has been increasingly used to quantify RV function and is known to have a strong correlation with CMR.15 Further studies are required for accurate assessment of RV function with these techniques.
In the present study, the absolute value and adjusted value of RV size showed different trends by sex, age, and race. Current ASE/EACVI guidelines suggest that adjustment for BSA should be performed in left chamber measurements to allow for differences in body size.11 Conversely, most RV chamber values are not adjusted in the current guideline; therefore, misclassification may occur. D’Oronzio et al demonstrated that adjusting RV size for BSA is an important determinant of RV dimensions and systolic function.16 Whether the best method for chamber quantification of the RV is to use the absolute or adjusted value is a matter of debate.
This study has some limitations. First, it should be noted that only 2 centers from Japan were included in the WASE study. This limited representation may not be sufficient for generalizing the findings of this study to the Japanese population. To establish reference values that are applicable to Japan, studies involving a greater number of institutions from across the country are needed. Second, because the present study was a subanalysis of the WASE study, the number of subjects in was small. Further studies on a larger number of subjects are needed. Third, because the RV has a complex 3D geometry, it is challenging to accurately assess RV chamber function with conventional 2D echocardiography. Three-dimensional echocardiography allows for the measurement of RV volumes directly, regardless of its complex shape. In addition, longitudinal strain with speckle-tracking echocardiography is more sensitive than conventional echocardiographic parameters. Future studies are warranted to assess RV performance accurately with 3D or speckle-tracking echocardiography. Finally, comparison of Japanese data with that of other Asian groups would be interesting. Differences in the size and function of the RV may exist across various racial groups, even within the same Asian population. However, the study was jointly designed by our Japanese team and our US collaborators in the WASE study, and we had limited access to data from other Asian cohorts. Future research will be needed to facilitate such comparative analyses.
Conclusions
For the first time, we determined reference values for RV size and systolic function obtained using 2D echocardiography based on measurements from a core laboratory in healthy Japanese subjects, and investigated the influence of sex, age, and race on these values. RV dimensions and length, as well as areas, were larger in men than in women. In addition, RV size decreased gradually with age, and was smaller in Japanese compared with American individuals. In contrast, RV systolic function parameters showed minimal or no differences by sex, age, and race.
These results may be helpful in clinical practice, and these changes should be considered carefully when evaluating RV performance.
Sources of Funding
This work was partly supported by a Grant-in-Aid for Scientific Research C (21K12701) from the Japan Society for the Promotion of Science (M.D.).
Disclosures
The authors declare that there are no conflicts of interest.
IRB Information
This study was approved by the Institutional Ethics Committee of the University of Tokyo (Reference no. 11345).
Data Availability
The deidentified participant data will not be shared.
References
- 1.
Pandey A, Omar W, Ayers C, LaMonte M, Klein L, Allen NB, et al. Sex and race differences in lifetime risk of heart failure with preserved ejection fraction and heart failure with reduced ejection fraction. Circulation 2018; 137: 1814–1823, doi:10.1161/CIRCULATIONAHA.117.031622.
- 2.
Colantonio LD, Gamboa CM, Richman JS, Levitan EB, Soliman EZ, Howard G, et al. Black-White differences in incident fatal, nonfatal, and total coronary heart disease. Circulation 2017; 136: 152–166, doi:10.1161/CIRCULATIONAHA.116.025848.
- 3.
Ministry of Health, Labour and Welfare. https://www.mhlw.go.jp/content/000711007.pdf (accessed September 10, 2023) (in Japanese).
- 4.
Asch FM, Miyoshi T, Addetia K, Citro R, Daimon M, Desale S, et al. Similarities and differences in left ventricular size and function among races and nationalities: Results of the World Alliance Societies of Echocardiography Normal Values Study. J Am Soc Echocardiogr 2019; 32: 1396–1406.e2, doi:10.1016/j.echo.2019.08.012.
- 5.
Daimon M, Watanabe H, Abe Y, Hirata K, Hozumi T, Ishii K, et al. Normal values of echocardiographic parameters in relation to age in a healthy Japanese population: The JAMP study. Circ J 2008; 72: 1859–1866, doi:10.1253/circj.CJ-08-0171.
- 6.
Daimon M, Watanabe H, Abe Y, Hirata K, Hozumi T, Ishii K, et al. Gender differences in age-related changes in left and right ventricular geometries and functions: Echocardiography of a healthy subject group. Circ J 2011; 75: 2840–2846, doi:10.1253/circj.CJ-11-0364.
- 7.
Mohammed SF, Hussain I, Abou Ezzeddine OF, Takahama H, Kwon SH, Forfia P, et al. Right ventricular function in heart failure with preserved ejection fraction: A community-based study. Circulation 2014; 130: 2310–2320, doi:10.1161/CIRCULATIONAHA.113.008461.
- 8.
Modin D, Møgelvang R, Andersen DM, Biering-Sørensen T. Right ventricular function evaluated by tricuspid annular plane systolic excursion predicts cardiovascular death in the general population. J Am Heart Assoc 2019; 8: e012197, doi:10.1161/JAHA.119.012197.
- 9.
Addetia K, Miyoshi T, Citro R, Daimon M, Gutierrez Fajardo P, Kasliwal RR, et al. Two-dimensional echocardiographic right ventricular size and systolic function measurements stratified by sex, age, and ethnicity: Results of the World Alliance of Societies of Echocardiography Study. J Am Soc Echocardiogr 2021; 34: 1148–1157.e1, doi:10.1016/j.echo.2021.06.013.
- 10.
Asch FM, Banchs J, Price R, Rigolin V, Thomas JD, Weissman NJ, et al. Need for a global definition of normative echo values-rationale and design of the World Alliance of Societies of Echocardiography Normal Values Study (WASE). J Am Soc Echocardiogr 2019; 32: 157–162.e2, doi:10.1016/j.echo.2018.10.006.
- 11.
Lang RM, Badano LP, Victor MA, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2015; 28: 1–39.e14, doi:10.1016/j.echo.2014.10.003.
- 12.
Maffessanti F, Muraru D, Esposito R, Gripari P, Ermacora D, Santoro C, et al. Age-, body size-, and sex-specific reference values for right ventricular volumes and ejection fraction by three-dimensional echocardiography: A multicenter echocardiographic study in 507 healthy volunteers. Circ Cardiovasc Imaging 2013; 6: 700–710, doi:10.1161/CIRCIMAGING.113.000706.
- 13.
Kawut SM, Lima JAC, Barr RG, Chahal H, Jain A, Tandri H, et al. Sex and race differences in right ventricular structure and function: The multi-ethnic study of atherosclerosis-right ventricle study. Circulation 2011; 123: 2542–2551, doi:10.1161/CIRCULATIONAHA.110.985515.
- 14.
Lee JZ, Low SW, Pasha AK, Howe CL, Lee KS, Suryanarayana PG. Comparison of tricuspid annular plane systolic excursion with fractional area change for the evaluation of right ventricular systolic function: A meta-analysis. Open Heart 2018; 5: e000667, doi:10.1136/openhrt-2017-000667.
- 15.
Li Y, Zhang L, Gao Y, Wan X, Xiao Q, Zhang Y, et al. Comprehensive assessment of right ventricular function by three-dimensional speckle-tracking echocardiography: Comparisons with cardiac magnetic resonance imaging. J Am Soc Echocardiogr 2021; 34: 472–482, doi:10.1016/j.echo.2020.12.013.
- 16.
D’Oronzio U, Senn O, Biaggi P, Gruner C, Jenni R, Tanner FC, et al. Right heart assessment by echocardiography: Gender and body size matters. J Am Soc Echocardiogr 2012; 25: 1251–1258, doi:10.1016/j.echo.2012.08.013.
