Neoatherosclerosis in Sirolimus-Eluting Stents After Paclitaxel-Coated Ballooning Cannot Be Stabilized Despite PCSK9 Inhibitor Therapy
論文ID: CR-19-0014
この記事には本公開記事があります。

詳細
論文ID: CR-19-0014
A 60-year-old man had undergone percutaneous coronary intervention 11 years previously. A sirolimus-eluting stent (SES) was implanted for a mid-left anterior descending artery (LAD). At that time, coronary angioscopy (CAS) showed white intima on the stent (Figure B-a). Two years later, the intima on the SES had changed to yellow on CAS, suggesting that neoatherosclerosis had occurred. Seven years after that, non-ST elevation myocardial infarction was noted at the stented site, with neoatherosclerosis. The patient underwent emergency coronary intervention for the LAD via paclitaxel-coated ballooning. Thrombolysis in myocardial infarction flow grade 3 was noted. CAS showed a brighter yellow plaque at the stent site (Figure B-b). One year later, the intima with neoatherosclerosis still had a higher yellow grade plaque (Figure B-c). Therefore, evolocumab was commenced because of the high risk for coronary artery disease.1 After 7 months of evolocumab, low-density lipoprotein cholesterol had decreased from 102 mg/dL to 7 mg/dL, and lipoprotein(a) had decreased from 32 mg/dL to 3.3 mg/dL. A residual dense yellow plaque with thinning neointima and attached red thrombus, however, was noted at the SES on CAS (Figure B-d).
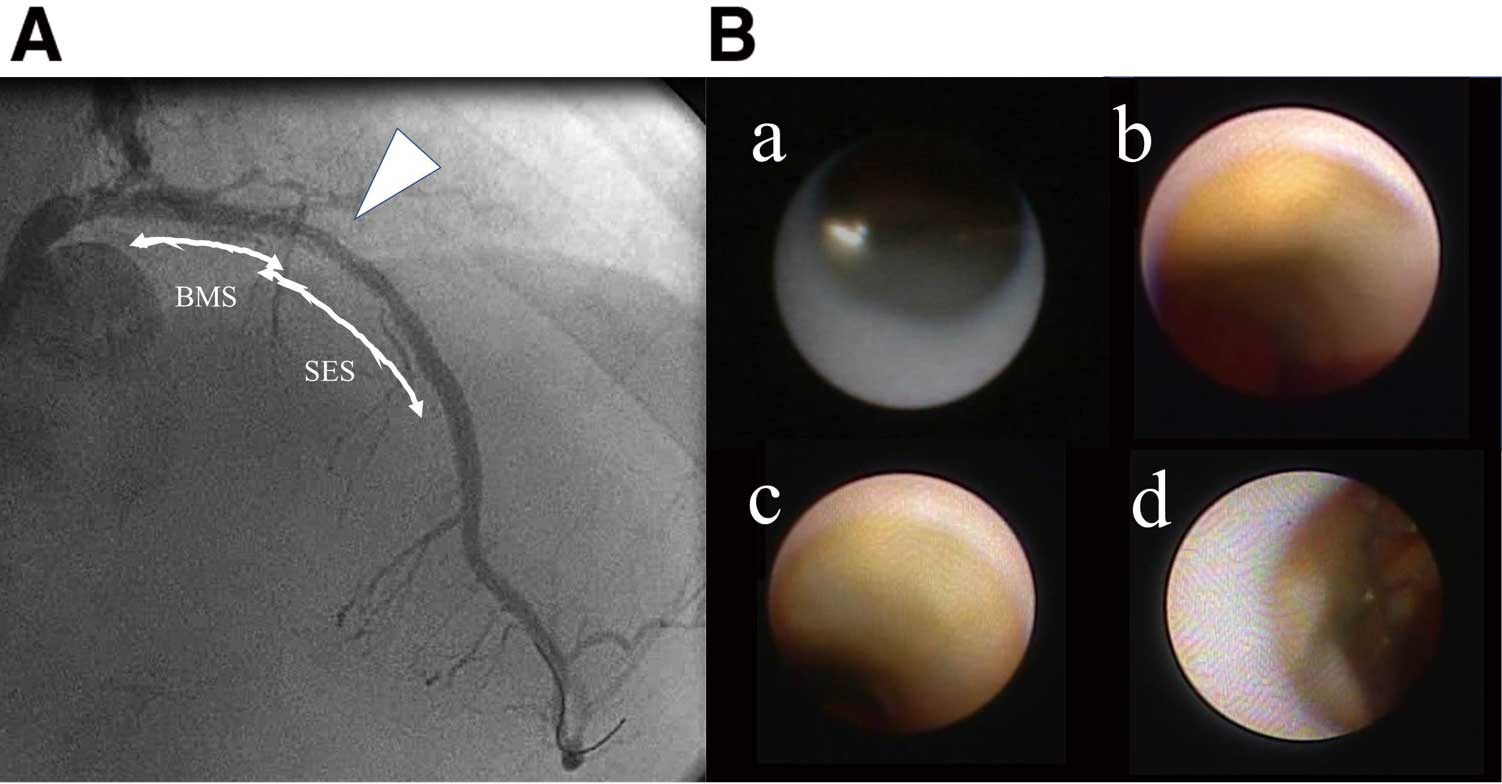
(A) Coronary angiography after 7 months of evolocumab (white arrow, sirolimus-eluting stent [SES] implantation site). (B) Coronary angioscopy at the SES implantation site (a) 11 years previously; (b) 9 years previously; (c) 2 years previously; and (d) after the 7-month evolocumab treatment.
CAS could clearly visualize the residual yellow plaque with a red thrombus and the thinning neointima. This indicates that aggressive lipid-lowering therapy cannot stabilize advanced neoatherosclerosis after SES implantation and that paclitaxel-coated ballooning might impair endothelial function because of the direct drug effect.
The authors declare no conflicts of interest.