Abstract
Objectives: The ability to transfer between surfaces is essential for wheelchair users’ independence. We hypothesized that transfer of hemiparetic stroke patients would be improved by using surfaces at the same height with no gap or obstacle between them.
Methods: A cross-sectional study was conducted to compare the difficulty of two transfer methods as a pilot study. Thirteen hemiparetic stroke patients were transferred from a platform table to a chair (wheelchair or flat chair) and from the chair to the table using the regular and lateral transfer methods. Functional Independence Measure (FIM) transfer score in both transfer methods and Stroke Impairment Assessment Set (SIAS) score were measured.
Results: The FIM transfer score significantly increased in the lateral transfer condition compared with the regular transfer condition, indicating that the former method reduced the transfer difficulty, regardless of the SIAS scores.
Conclusions: The transfer difficulty of patients with hemiparetic stroke decreases when using the lateral transfer method. The lateral transfer method is easy, potentially helping prevent care-related injuries among caregivers.
Introduction
Mobility is a fundamental function for the enrichment of well-being and quality of life, and the ability to transfer from one surface to another is essential for independence among wheelchair users. Despite transfers being a frequent daily activity, they are ranked as difficult among wheelchair-related activities.1,2
A previous study demonstrated that the difficulty of performing transfers is affected by the difference in height, width of the gap, and presence of an obstacle (armrest) between transfer surfaces.3 Specifically, in cases where the person is able to independently perform a transfer to and from a wheelchair, gaps wider than 8.9 cm between transfer surfaces at the same height make transfers increasingly difficult, particularly in the presence of an obstacle.3 The presence of such difficulties between transfer surfaces requires greater recruitment of the biceps and anterior deltoid muscles compared with when a wheelchair is located close to a transfer surface.4–6
Moreover, transfer activity can cause upper limb pain and overuse-related injuries in wheelchair users,7–9 and is the most common activity leading to falls in patients with stroke.10 In a multivariate analysis performed by Lamb et al., transfer ability was related to the incidence of falls.11
Difficulties in performing transfers in wheelchair users can cause additional problems for the healthcare provider and/or family members who provide care for them. For persons who are not able to transfer by themselves, a caregiver is required to support transfers during daily activities. A previous study reported that work-related injuries to healthcare workers and caregivers during transfers are common.12–18 Providing assistance with transfers has caused work-related injuries in more than 78% of physical therapists and their assistants at rehabilitation facilities.19 Because of the work-related incidence of low back pain, 10% of female nurses reported having lost more than 1 month out of their total working days.20
The most common transfer method, which is known as a regular transfer or “getting-up transfer,” is defined as lifting the buttocks during transfer from one surface to another surface. Generally, the patient requires assistance at the point of lifting and rotating the buttocks during transfer. If interfering factors, such as a difference in the height of the surfaces, the width of the gap, or the presence of an obstacle, can be removed, the patient is more likely to be able to perform a transfer by scooting their buttocks laterally without lifting. This practice is referred to as the “lateral transfer.” We hypothesized that patients with hemiparetic stroke can improve their transfer independence by performing a lateral transfer under an environmental setup in which the transfer surfaces are at the same height with no gap, and with no obstacle between the surfaces. However, it is unclear whether there is a difference in the difficulty between the getting-up method and the lateral transfer method. If our hypothesis is correct, the lateral transfer approach would facilitate the independence of transfers and decrease the need for assistance during transfers. The aim of the present pilot study was to test our hypothesis among patients with hemiparetic stroke.
Methods
Participants
The current study used a cross-sectional design. Because this was a pilot study, the sample size was determined as the minimum number of participants based on previous reports that suggested recommendations for a sample size for pilot studies.21,22 Thirteen patients with hemiparetic stroke participated in the study (Mage=64.8 years, SD=10.5, range: 47–79 years; Table 1). All patients suffered from hemiparesis following a cerebrovascular incident, and patients’ mean height and weight were 162.6 (SD=8.8 cm) and 57.4 (SD=11.6 kg), respectively. The exclusion criteria were as follows: presence of bilateral, cerebellar, and/or brain-stem lesions; severe upper-extremity pain or injury; severe injury of the lower extremity on the non-paretic side; other neuromuscular disease; and pressure sores.
Table1
Participants’ characteristics (N=13)
| ID |
Gender |
Age
(years) |
Height
(cm) |
Weight
(kg) |
TO
(days) |
Diagnosis |
Paretic side |
SIAS |
Cognitive impairments |
MMSE |
| HF |
KE |
FT |
KM |
FF |
| 1 |
Male |
68 |
164 |
58.2 |
51 |
CH |
Right |
4 |
4 |
3 |
3 |
4 |
MD |
27 |
| 2 |
Female |
69 |
156 |
47.6 |
21 |
CH |
Left |
0 |
0 |
0 |
0 |
0 |
USN, AD, MD, ED |
20 |
| 3 |
Female |
47 |
167 |
58.3 |
23 |
CH |
Left |
1 |
2 |
0 |
0 |
0 |
None |
29 |
| 4 |
Male |
74 |
160 |
49.6 |
40 |
CI |
Left |
1 |
1 |
1 |
1 |
0 |
AD, USN |
18 |
| 5 |
Male |
66 |
165 |
50.5 |
13 |
CH |
Left |
1 |
0 |
0 |
0 |
0 |
AD, USN |
26 |
| 6 |
Male |
56 |
165 |
53.3 |
30 |
SAH |
Left |
1 |
1 |
0 |
3 |
3 |
MD, AD, ED |
25 |
| 7 |
Male |
68 |
170 |
55.4 |
27 |
CH |
Right |
2 |
2 |
0 |
1 |
0 |
AD, Asomatognosia |
23 |
| 8 |
Female |
67 |
161 |
45.2 |
117 |
CI |
Right |
3 |
2 |
2 |
2 |
2 |
Motor aphasia, AD, MD, USN |
18 |
| 9 |
Male |
76 |
156 |
47 |
45 |
CH |
Right |
1 |
1 |
0 |
1 |
0 |
Motor aphasia, USN, AD |
unmeasurable |
| 10 |
Female |
54 |
150 |
64.4 |
152 |
CH |
Left |
1 |
1 |
0 |
1 |
0 |
AD |
30 |
| 11 |
Female |
79 |
153 |
55.3 |
37 |
CH |
Right |
4 |
4 |
4 |
4 |
4 |
None |
26 |
| 12 |
Male |
71 |
162 |
78.5 |
36 |
CI |
Left |
2 |
3 |
3 |
2 |
1c |
AD |
27 |
| 13 |
Male |
47 |
185 |
82.6 |
104 |
CH |
Left |
3 |
3 |
3 |
2 |
2 |
Motor aphasia |
20 |
| Mean |
64.8 |
162.6 |
57.4 |
53.5 |
|
|
|
|
|
|
|
|
24.1 |
| (SD) |
(10.5) |
(8.8) |
(11.6) |
(42.8) |
|
|
|
|
|
|
|
|
(4.2) |
Note. TO, Time since stroke onset; CI, Cerebral infarction; CH, Cerebral hemorrhage; SAH, Subarachnoid hemorrhage; SIAS, Stroke Impairment Assessment Set; HF, Hip flexion test; KE, Knee extension test; FT, Foot tap test; KM, Knee mouth test; FF, Finger function test; MD, Memory disorder; USN, Unilateral spatial neglect; AD, Attentional disorder; ED, Executive dysfunction; MMSE, Mini-Mental State.
In the start position, the patient sat on the platform table with their feet on the floor. The patients were asked to transfer to/from the wheelchair in their usual way. The procedure for transferring from the platform table to the wheelchair was as follows (Figure 1c): (1) scoot forward to the edge of the platform table from the start position, (2) slide their buttocks laterally on the platform table closer to the wheelchair, (3) lean their trunk forward and lift their buttocks from the platform table, (4) rotate their buttocks to the direction of the wheelchair so that their head moves in the opposite direction to their buttocks, and (5) slowly sit on the wheelchair. In contrast, transfer from the wheelchair to the platform table was performed as follows: (1) grasp the armrest of the wheelchair with the non-paralyzed upper limb, (2) scoot forward to the edge of the wheelchair seat, (3) slide their buttocks within the wheelchair seat to be closer to the platform table, (4) lean their trunk forward and put their non-paralyzed hand on the platform table, (5) lift their buttocks from the wheelchair, (6) rotate their buttocks to the direction of the platform table, and (7) sit down slowly on the platform table.
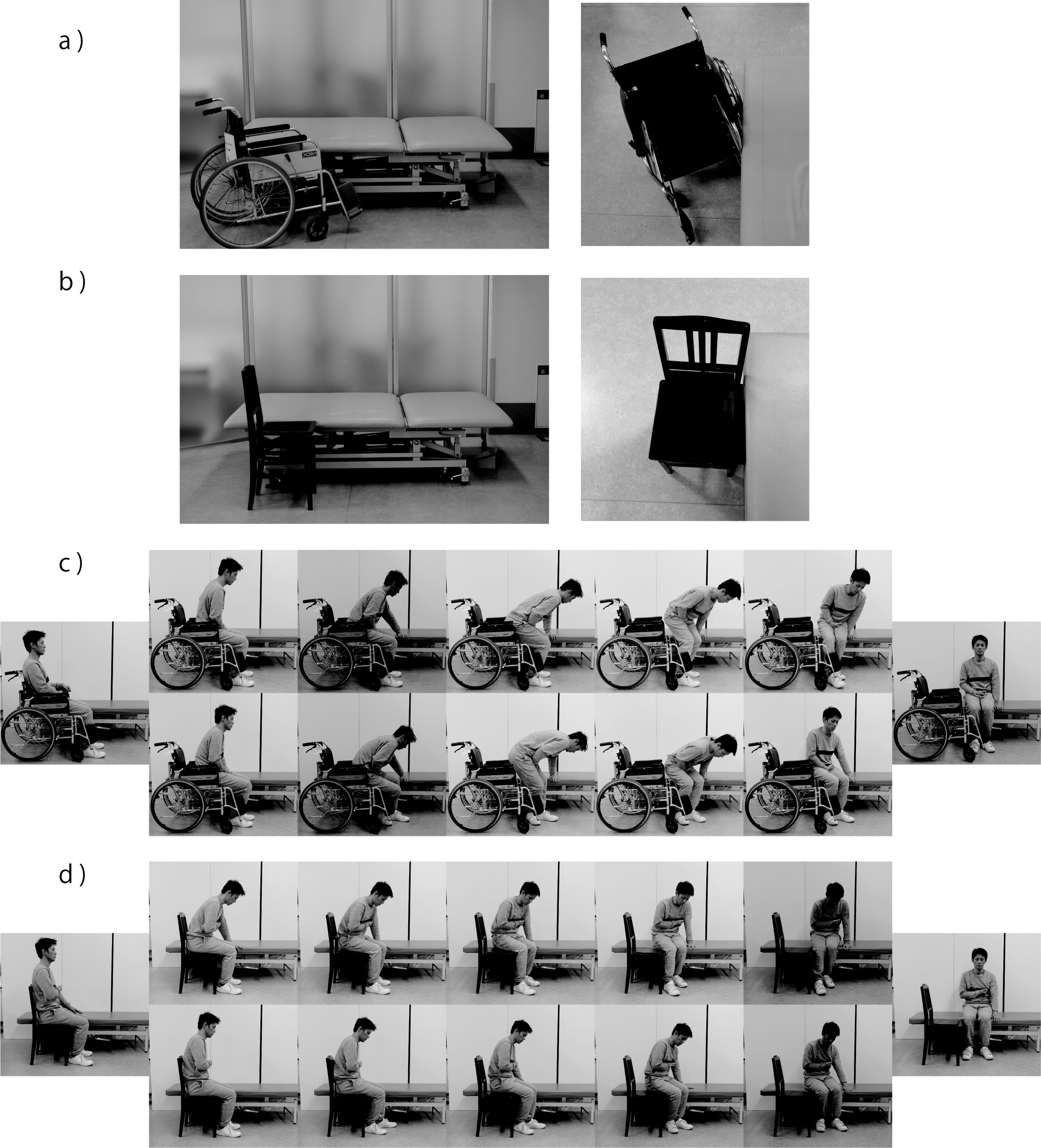
The starting position involved the patient sitting on the platform table with their feet on the floor. The patients were asked to transfer to/from the flat chair. The procedure was as follows (Figure 1d): (1) scoot forward to the edge of the platform table from the starting position, and (2) push on the platform table using their non-paretic upper limb to scoot their buttocks laterally to the surface of the flat chair. During the scooting movement, patients leaned their trunk slightly forward to move the weight of their buttocks to their feet. (3) Repeat the scooting motion several times until they are sitting on the flat chair. Conversely, the transfer from the flat chair to the platform table was performed as follows: (1) put their non-paretic upper limb on the platform table, and (2) scoot laterally from the starting position to the platform table repeatedly until they are sitting on the platform table.
Experimental setup and procedure
A platform table, a standard wheelchair without a seat cushion, and a square flat chair (PI5; Yamaha Co., Ltd., Hamamatsu, Japan) with no armrests were used to perform the experiment. The height of the platform table and flat chair were adjusted to the same level as the height of the wheelchair seat. In the experiment using the wheelchair, it was positioned close to the platform table at 20–45° with the non-paretic side of the participant facing the platform table (Figure 1a). Before performing a transfer, both wheels of the wheelchair were locked in place. In the experiment using the flat chair, the chair was positioned parallel and very close to the platform table without a gap between the table and chair seat (Figure 1b). The chair was also positioned so that the paretic side of the patient faced the chair when sitting on the side of the platform table.
The participants performed the following four transfers: (1) transfer from the platform table to the standard wheelchair, (2) transfer from the standard wheelchair to the platform table, (3) transfer from the platform table to the flat chair, and (4) transfer from the flat chair to the platform table. Each transfer was performed according to the procedures described in the following section. One transfer was performed under each transfer condition. The patients were allowed to rest for a few minutes between trials according to their fatigue. One therapist closely supervised the patients to prevent a fall during transfers. According to the patient’s transfer ability, the therapist supported the lifting and/or rotating of the participant’s buttocks with minimum assistance. The transfers were video-recorded with a video camera for the assessment.
Assessment
The Functional Independence Measure (FIM) transfer score was used as a measure of the primary outcome. The FIM transfer score provides a measure of the amount of physical assistance needed and level of independence observed during transfers based on a 1–7 ordinal scale and it has been shown to have high inter-rater reliability and validity.23–26 A score of 7 indicates “complete independence,” 6 indicates “modified independence,” 5 indicates “supervision,” 4 indicates “minimal assistance (subject 75%+),” 3 indicates “moderate assistance (subject 50%+),” 2 indicates “maximal assistance (subject 25%+),” and 1 equals “total assistance (subject 0%+).” Transfer ability was evaluated by three occupational therapists (including the therapist who supervised the transfer) using video footage of the transfer motions. In cases of disagreement between the raters, they discussed the score until a consensus was obtained. To examine the relationship between the transfer performance and the degree of motor impairment, the Stroke Impairment Assessment Set (SIAS) for motor function was used to assess motor impairment.27,28 The SIAS is a standardized measure of stroke impairment that consists of 22 subcategories, such as motor function, muscle tone, sensation, and pain. For motor function, each item is rated from 0 (severely impaired) to 5 (normal).
Ethics
The study protocol was approved by the Ethics Review committee of Fujita Health University. All patients provided written informed consent before their participation in the study. This study was performed in accordance with the Declaration of Helsinki.
Data analysis and statistical analysis
To analyze the SIAS finger score, 1a, 1b, and 1c of the SIAS finger score were transformed to 1, 2, and 3, respectively, while 2, 3, 4, and 5 of the SIAS finger score were transformed to 4, 5, 6, and 7, respectively, according to a previous study.29 To compare the FIM scores for getting-up transfer and lateral transfer, we used a Wilcoxon signed rank test. The relationship between the total SIAS motor function score and FIM transfer score was shown as a scatter diagram with a probability ellipse to analyze the trends between the motor impairment level and difficulty level for the two transfer types. All statistical analyses were performed with R (3.4.3; Institute of Statistical Mathematics, Tokyo, Japan). The statistical significance level was set at a p-value of .05.
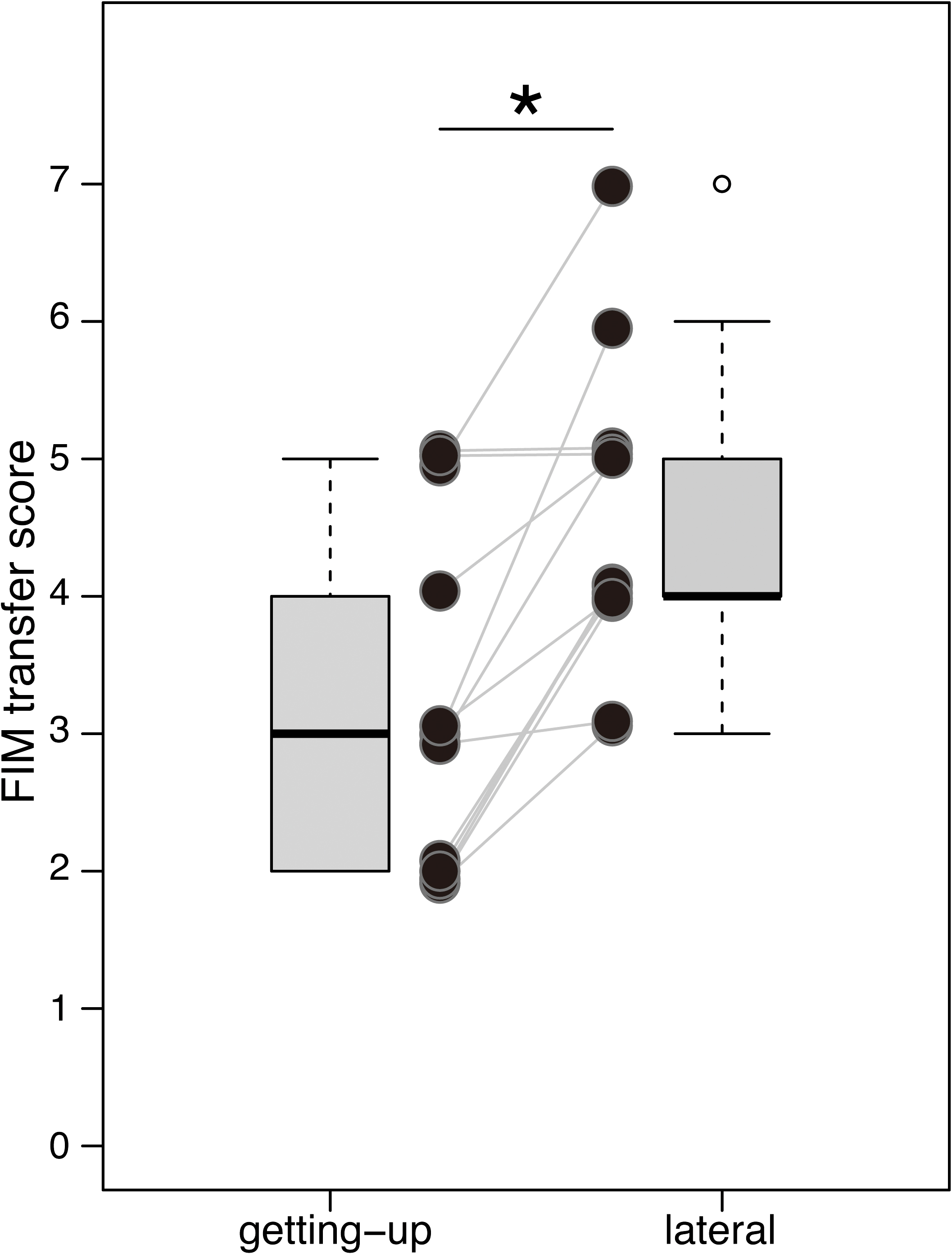
Results
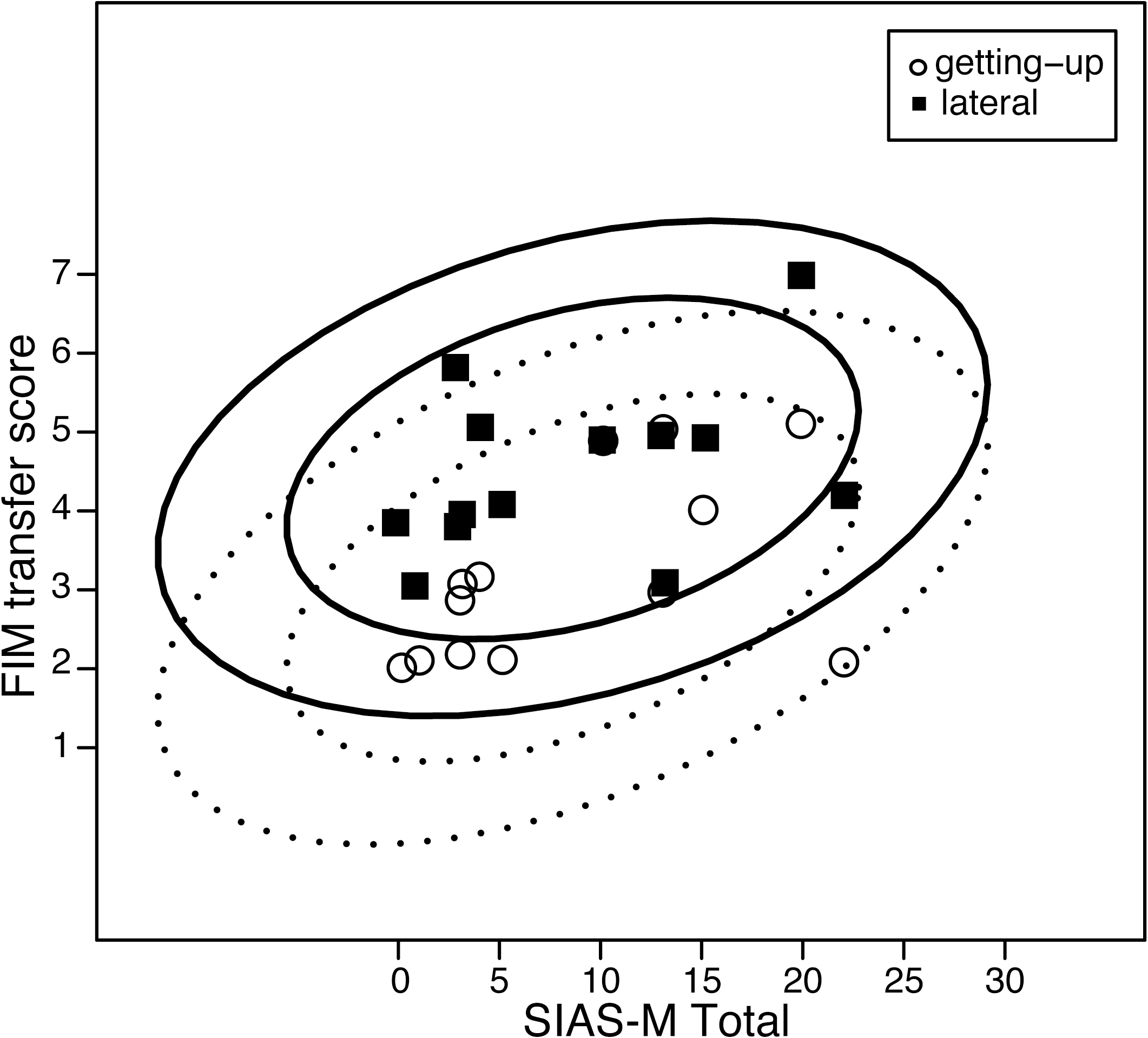
All patients performed all transfers without any adverse events. The FIM transfer scores for the getting-up and lateral transfer methods are shown in Figure 2. The FIM transfer score was higher for the lateral transfer compared with the getting-up transfer in almost all patients. The median FIM score for the getting-up transfer was 3 (range 2–5). For the lateral transfer, the median FIM score was 4 (range 3–7). Statistical analysis revealed that the FIM score was significantly higher in the lateral transfer method than in the getting-up transfer method (p=.002). The relationship between the FIM transfer score for each method and the total SIAS motor function score is shown in Figure 3. The probability ellipse shifted in the upward direction for the lateral transfer compared with the getting-up transfer, indicating that the lateral transfer improved the degree of independence and reduced the degree of assistance, even in participants with a similar degree of lower-limb motor paralysis.
Discussion
One of the most important aspects of rehabilitation practice is ensuring safety and independence in activities of daily living. The aim of the present study was to test whether the level of independence in performing a transfer differs between two methods for a bed-to/from-wheelchair transfer in patients with hemiparetic stroke. The FIM transfer scores were significantly higher for the lateral transfer than for the getting-up transfer. These results suggested that the lateral transfer was safe for use in transferring patients with stroke. Moreover, the results detailed how much lateral transfer contributed to the improvement of independence in transferring, which is clinically useful in deciding the type of vehicle to use, based on patients’ ability.
In the commonly used getting-up transfer method, to perform a transfer from a wheelchair to another surface, patients must lift their buttocks to avoid hitting the armrest and wheel of the wheelchair5,6,30–34. Conversely, the lateral transfer method requires patients to raise their center of gravity only a minimal amount and allows them to transfer to another surface by moving their center of gravity mainly in a lateral direction on the level surface. A particularly important difference may be that the lateral transfer method does not require high motor functioning of the lower limbs. Previous studies reported that the lower limbs play an essential role in supporting body mass and controlling sitting balance during major forward movements of the center of gravity in a sitting position that occur during getting-up transfers.35,36
The lateral transfer method may also reduce the risk of transfer-related pain and accidents such as falls in patients with hemiparetic stroke. When wheelchair users with poor trunk and lower-limb function transfer from a seat to another surface, they must rely on their upper extremities for stability and mobility. Their soft tissue structures are exposed to overuse during transfers because the shoulder becomes a weight-bearing joint.7 The overuse of an upper limb can contribute to the pathogenesis of joint pain.7 Regarding transfer-related falls among inpatients in a rehabilitation center, Saverino et al. reported that falls occur most frequently during standing up without assistance.37 As a lateral transfer is achieved by a narrow range of movements in the antero-posterior and vertical directions, this might reduce the burden and subsequent pain of the upper limbs and the risk of falling compared with the getting-up transfer method.
In addition, the present results suggest that the requirement for transfer assistance was decreased by using the lateral transfer method. As described above, work-related injuries to healthcare workers during transfers are prevalent in healthcare,14–17 with low back pain being the most common result.38 This injury typically occurs when the buttocks of the care receiver are lifted during a transfer.38 Thus, the present findings may be useful for the prevention of work-related injuries associated with transfer assistance.
A major clinical implication drawn from the present study is that the lateral transfer approach has the potential to improve the independence of transfers and decrease the need for assistance during transfers in various areas, such as the bed, toilet, and bathtub. A standard wheelchair has several barriers to this approach; in particular, the wheel, armrest, and height difference between the wheelchair and bed inhibit this approach. To overcome the difficulties involved in the getting-up transfer method when using a standard wheel chair, various assistive tools (e.g., transfer boards)39,40 and a wheelchair with a removable arm-rest type41 have been used. However, although these approaches can partially reduce the barriers, it cannot completely eliminate them. Considering the current findings, we argue for the development of novel transfer assist devices that eliminate such barriers completely and make the environment more conducive for lateral transfers. When a new mobility/transfer assistive device that can promote the lateral transfer method is proposed,42 rehabilitation workers could begin to recommend the use of the device based on the evidence presented in this study.
The results of the current study revealed that the lateral transfer was easier than the getting-up transfer in patients with hemiparetic stroke, even in participants with a similar degree of lower-limb motor paralysis. However, the present pilot study involved several limitations that should be considered. Because of the small sample size, it was not possible to delineate those characteristics of wheelchair users that are most beneficial for the lateral transfer method. Further research with a larger number of participants with various types and levels of impairment is needed to investigate which characteristics inhibit and facilitate the use of the lateral transfer method. Moreover, in future research, a multicenter randomized controlled trial should be carried out with an appropriately powerful sample size, given that this pilot study has shown that lateral transfer might be effective. Conducting further research with an appropriate sample size, in addition to a wider range of severities and disorders, would provide further clinical evidence of the advantages of the lateral transfer method.
Acknowledgments
We thank the staff of the Department of Rehabilitation at our university hospital for their contribution to this study.
Notes
Conflict of Interest
The authors declare that they have no competing interests.
References
- 1. Linacre JM, Heinemann AW, Wright BD, Granger CV, Hamilton BB. The structure and stability of the functional independence measure. Arch Phys Med Rehabil 1994; 75: 127–132.
- 2. Tsuji T, Sonoda S, Domen K, Saitoh E, Liu M, Chino N. ADL structure for stroke patients in Japan based on the functional independence measure. Am J Phys Med Rehabil 1995; 74: 432–438.
- 3. Toro ML, Koontz AM, Cooper RA. The impact of transfer setup on the performance of independent wheelchair transfers. Hum Factors 2013; 55: 567–580.
- 4. Koontz AM, Gagnon D, Brindle E, Cooper RA. Positioning the wheelchair close to the target surface reduces shoulder muscular demand for sitting pivot transfers. In Rehabilitation : mobility, exercise, and sports. Amsterdam: IOS Press; 2010: 13–15.
- 5. Koontz AM, Kankipati P, Lin YS, Cooper RA, Boninger ML. Upper limb kinetic analysis of three sitting pivot wheelchair transfer techniques. Clin Biomech 2011; 26: 923–929.
- 6. Koontz A, Toro M, Kankipati P, Naber M, Cooper R. An expert review of the scientific literature on independent wheelchair transfers. Disabil Rehabil Assist Technol 2012; 7: 20–29.
- 7. Alm M, Saraste H, Norrbrink C. Shoulder pain in persons with thoracic spinal cord injury: Prevalence and characteristics. J Rehabil Med 2008; 40: 277–283.
- 8. Brose SW, Boninger ML, Fullerton B, McCann T, Collinger JL, Impink BG, Dyson-Hudson TA. Shoulder ultrasound abnormalities, physical examination findings, and pain in manual wheelchair users with spinal cord injury. Arch Phys Med Rehabil 2008; 89: 2086–2093.
- 9. Dalyan M, Cardenas DD, Gerard B. Upper extremity pain after spinal cord injury. Spinal Cord 1999; 37: 191–195.
- 10. White HC. Post-stroke hip fractures. Arch Orthop Trauma Surg 1988; 107: 345–347.
- 11. Lamb SE, Ferrucci L, Volapto S, Fried LP, Gurainik JM. Risk factors for falling in home-dwelling older women with stroke. Stroke 2003; 34: 494–501.
- 12. Alperovitch-Najenson D, Sheffer D, Treger I, Finkels T, Kalichman L. Rehabilitation versus nursing home nurses’ low back and neck-shoulder complaints. Rehabil Nurs 2015; 40: 286–293.
- 13. Bhimani R. Understanding work-related musculoskeletal injuries in rehabilitation from a nursing perspective. Rehabil Nurs 2016; 41: 91–100.
- 14. Bork BE, Cook TM, Rosecrance JC, Engelhardt KA, Thomason ME, Wauford IJ, Worley RK. Work-related musculoskeletal disorders among physical therapists. Phys Ther 1996; 76: 827–835.
- 15. Campo M, Weiser S, Koenig KL, Nordin M. Work-related musculoskeletal disorders in physical therapists: A prospective cohort study with 1-year follow-up. Phys Ther 2008; 88: 608–619.
- 16. Darragh AR, Huddleston W, King P. Work-related musculoskeletal injuries and disorders among occupational and physical therapists. Am J Occup Ther 2009; 63: 351–362.
- 17. Smedley J, Egger P, Cooper C, Coggon D. Prospective cohort study of predictors of incident low back pain in nurses. BMJ 1997; 314: 1225–1228.
- 18. Theis JL, Finkelstein MJ. Long-term effects of safe patient handling program on staff injuries. Rehabil Nurs 2014; 39: 26–35.
- 19. McCrory B, Burnfield JM, Darragh AR, Meza JL, Irons SL, Chernyavskiy P, Link AM, Brusola G. Work injuries among therapists in physical rehabilitation. Proc Hum Factors Ergon Soc Annu Meet 2014; 54: 1072–1076.
- 20. Smedley J, Egger P, Cooper C, Coggon D. Manual handling activities and risk of low back pain in nurses. Occup Environ Med 1995; 52: 160–163.
- 21. Julious SA. Sample size of 12 per group rule of thumb for a pilot study. Pharm Stat 2005; 4: 287–291.
- 22. Moore CG, Carter RE, Nietert PJ, Stewart PW. Recommendations for planning pilot studies in clinical and translational research. Clin Transl Sci 2011; 4: 332–337.
- 23. Hamilton BB, Laughlin JA, Fiedler RC, Granger CV. Interrater reliability of the 7-level functional independence measure (FIM). Scand J Rehabil Med 1994; 26: 115–119.
- 24. Heinemann AW, Linacre JM, Wright BD, Hamilton BB, Granger C. Relationships between impairment and physical disability as measured by the functional independence measure. Arch Phys Med Rehabil 1993; 74: 566–573.
- 25. Kidd D, Stewart G, Baldry J, Johnson JJ, Rossiter D, Petruckevitch A, Thompson AJ. The functional independence measure: A comparative validity and reliability study. Disabil Rehabil 1995; 17: 10–14.
- 26. Ottenbacher KJ, Hsu Y, Granger CV, Fiedler RC. The reliability of the functional independence measure: A quantitative review. Arch Phys Med Rehabil 1996; 77: 1226–1232.
- 27. Chino N, Sonoda S, Domen K, Saitoh E, Kimura A. Stroke Impairment Assessment Set (SIAS). The Japanese Journal of Rehabilitation Medicine 1994; 31: 119–125.
- 28. Liu M, Chino N, Tuji T, Masakado Y, Hase K, Kimura A. Psychometric properties of the Stroke Impairment Assessment Set (SIAS). Neurorehabil Neural Repair 2002; 16: 339–351.
- 29. Fujiwara T, Kasashima Y, Honaga K, Muraoka Y, Tsuji T, Osu R, Hase K, Masakado Y, Liu M. Motor improvement and corticospinal modulation induced by Hybrid Assistive Neuromuscular Dynamic Stimulation (HANDS) therapy in patients with chronic stroke. Neurorehabil Neural Repair 2009; 23: 125–132.
- 30. Hess JA, Kincl LD, Mandeville DS. Comparison of three single-person manual patient techniques for bed-to-wheelchair transfers. Home Healthc Nurse 2007; 25: 577–579.
- 31. Krishnan RH, Pugazhenthi S. Design and development of a wheel chair based manual self-transfer device for elderly and disabled. J Med Devices 2016; 10: 024501.
- 32. Rice LA, Smith I, Kelleher AR, Greenwald K, Hoelmer C, Boninger ML. Impact of the clinical practice guideline for preservation of upper limb function on transfer skills of persons with acute spinal cord injury. Arch Phys Med Rehabil 2013; 94: 1230–1246.
- 33. Sabari J, Shea M, Chen L, Laurenceau A, Leung E. Impact of wheelchair seat height on neck and shoulder range of motion during functional task performance. Assist Technol 2016; 28: 183–189.
- 34. Tsai CY, Hogaboom NS, Boninger ML, Koontz AM. The relationship between independent transfer skills and upper limb kinetics in wheelchair users. Biomed Res Int 2014; 2014: 984526.
- 35. Dean CM, Shepherd RB. Task-related training improves performance of seated reaching tasks after stroke: A randomized controlled trial. Stroke 1997; 28: 722–728.
- 36. Dean C, Shepherd R, Adams R. Sitting balance I: Trunk-arm coordination and the contribution of the lower limbs during self-paced reaching in sitting. Gait Posture 1999; 10: 135–146.
- 37. Saverino A, Benevolo E, Ottonello M, Zsirai E, Sessarego P. Falls in a rehabilitation setting: functional independence and fall risk. Eura Medicophys 2006; 42: 179–184.
- 38. Vieira ER, Svoboda S, Belniak A, Brunt D, Rose-St Prix C, Roberts L, da Costa BR. Work-related musculoskeletal disorders among physical therapists: An online survey. Disabil Rehabil 2016; 38: 552–557.
- 39. Gruis KL, Wren PA, Huggins JE. Amyotrophic lateral sclerosis patients’ self-reported satisfaction with assistive technology. Muscle Nerve 2011; 43: 643–647.
- 40. Kjellberg K, Lagerstrom M, Hagberg M. Work technique of nurses in patient transfer tasks and associations with personal factors. Scand J Work Environ Health 2003; 29: 468–477.
- 41. Tsai CY, Boninger ML, Hastings J, Cooper RA, Rice L, Koontz AM. Immediate biomechanical implications of transfer component skills training on independent wheelchair transfers. Arch Phys Med Rehabil 2016; 97: 1785–1792.
- 42. Tanabe S, Saitoh E, Koyama S, Kiyono K, Tatemoto T, Kumazawa N, Kagaya H, Otaka Y, Mukaino M, Tsuzuki A, Ota H, Hirano S, Kanada Y. Designing a robotic smart home for everyone, especially the elderly and people with disabilities. Fujita Medical Journal 2019; 5: 31–35.
Appendices
Funding Statement
The authors received no support for this work.