Abstract
Calcification in a lung tumor suggests that it is a benign tumor such as a hamartoma or a sclerosing lung cell tumor. In contrast, carcinoid, lung cancer, carcinosarcoma, and sarcoma rarely harbor calcification. Primary lung adenocarcinomas with gross calcification that is suggestive of bone formation are very rare. It is difficult to distinguish between calcification and bone formation purely on the basis of image definitive diagnosis of bone formation being difficult in the absence of a large surgical specimen. Lung cancers with bone formation are exceedingly rare: to the best of our knowledge, only 13 cases have been reported. Careful attention is needed when differentiating between benign and malignant tumors. Here, we report a case of primary lung adenocarcinoma with gross calcification that was suggestive of bone formation.
Introduction
Calcification in a lung tumor suggests that it is a benign tumor such as a hamartoma or a sclerosing lung cell tumor.1 Although carcinoid,1 lung cancer,2–4 carcinosarcoma,5 and sarcoma6 rarely harbor calcification, a malignant tumor should be included in the differential diagnosis. Moreover, it is very rare to find gross calcification that is suggestive of bone formation in lung cancers. Because it is difficult to differentiate between calcification and bone formation purely on the basis of image, a definitive diagnosis of bone formation cannot be made without obtaining a large surgical specimen.
Case report
A 44-year-old man was referred to our hospital because of an abnormal shadow on a chest radiograph. Chest computed tomography (CT) four months later showed a 4 cm diameter tumor with a coarse high-density area in the right S10.
Laboratory tests showed high carcinoembryonic antigen (CEA) (62.7 ng/mL) and triglyceride (TG) (220 mg/dL) concentrations level. Thyroid and parathyroid function were normal (Table 1).
Table1
Laboratory data
| Hematology |
Biochemistry |
Serology |
| WBC |
5,400/μl |
T-Bil |
0.7 mg/dl |
CRP |
0.3>mg/l |
| Neutrophils |
70% |
AST |
20 IU/L |
|
|
| Eosinophils |
2% |
ALT |
20 IU/L |
Tumor marker |
| Lymphocytes |
24% |
LDH |
169 IU/L |
CEA |
62.7 ng/ml |
| Monoctes |
4% |
ALP |
201 IU/L |
CYFRA |
1.8 ng/ml |
| RBC |
525×104/μl |
TP |
6.8 g/dl |
ProGRP |
46.2 pg/ml |
| Hb |
15.0 g/dl |
Alb |
4.4 g/dl |
IL-2R |
390 U/ml |
| Hct |
44.6% |
BUN |
12.5 mg/dl |
|
|
| Plt |
25.6×104/μl |
Cre |
0.85 mg/dl |
T-SPOT |
negative |
|
|
Na |
141 mEq/L |
|
|
|
|
K |
4.1 mEq/L |
|
|
|
|
Cl |
105 mEq/L |
|
|
|
|
Ca |
9.2 mg/dl |
|
|
|
|
FBS |
102 mg/dl |
|
|
|
|
HbA1c (NGSP) |
5.6% |
|
|
|
|
Total cholesterol |
215 mg/dl |
|
|
|
|
Triglyceride (TG) |
220 mg/dl |
|
|
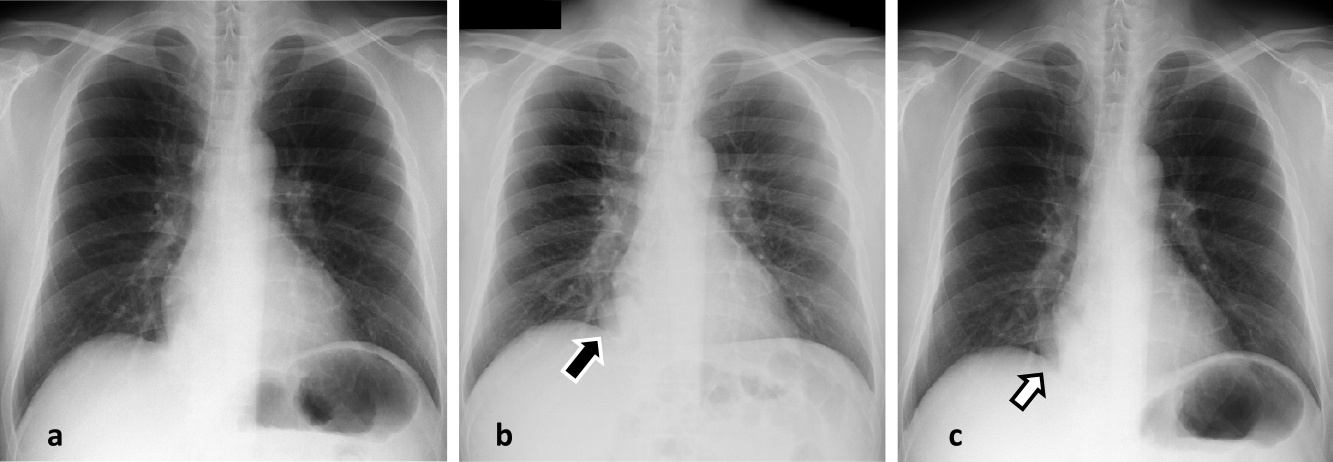
A chest radiograph taken 2 years before presentation was normal, whereas a coin-like nodular shadow was detected in the lower right lobe one year before presentation to our institution. That nodule gradually increased in size and was recognized as a significant mass four months before referral to our institution (Figure 1).
Chest CT showed a 4 cm diameter mass with irregular edges, pleural indentation, and gross calcification in the right S10. The fat component of the tumor was unclear. The mediastinal and hilar lymph nodes were not enlarged (Figure 2).
The tumor was suspected of being a lung hamartoma. However, because the tumor was seen to partially project into the bronchus on review of the chest CT images and the concentration of the tumor marker CEA was high, it was considered that the possibility of a malignant tumor warranted a bronchoscopy to establish a definitive diagnosis.
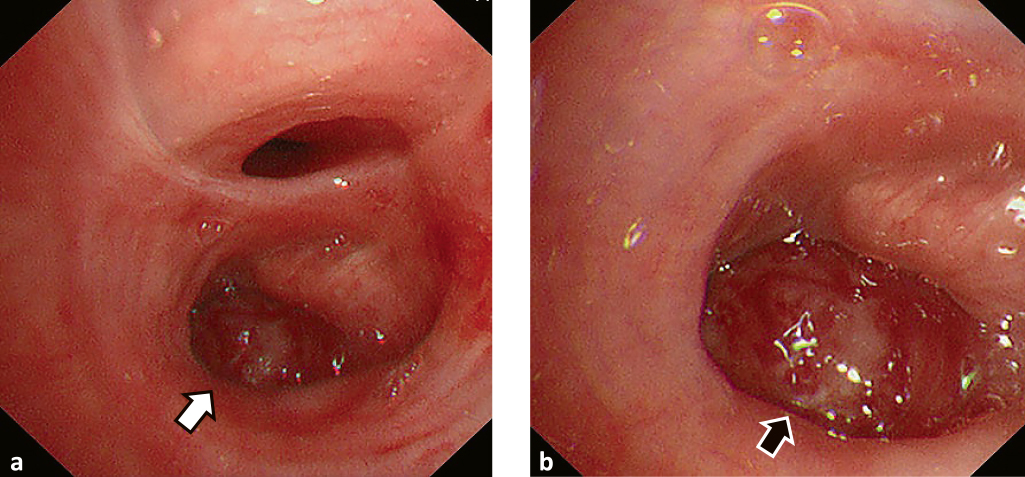
Bronchoscopy revealed a polyp-like tumor with an irregular surface protruding into and occluding the entrance of the right lower bronchus. A biopsy was taken from the tumor (Figure 3).
Pathological examination of the biopsy specimen revealed irregular ductal hyperplasia with atypical cells, and many small areas of calcification, some of which were within the tumor. Von Kossa staining confirmed calcium deposition. Immunostaining was positive for CK7, TTF-1 and Napsin A, and negative for CK20. Thus, the pathological diagnosis was primary lung adenocarcinoma with remarkable calcification (Figure 4).
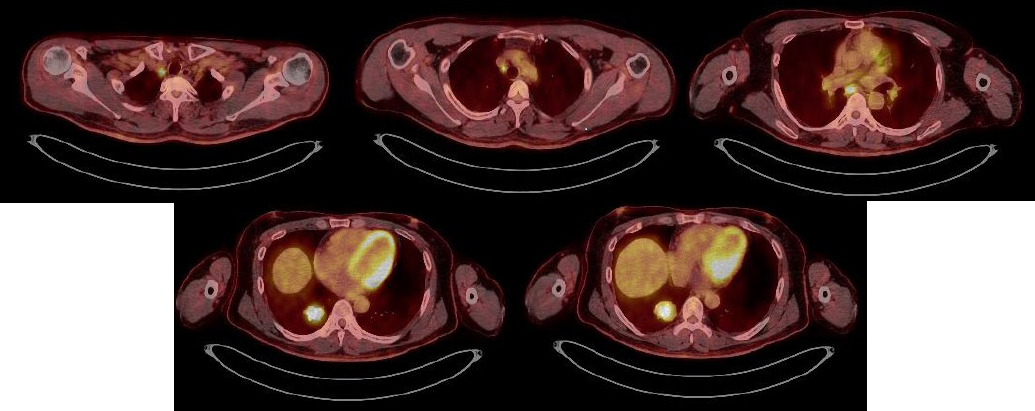
Fluorodeoxyglucose-positron emission tomography (FDG-PET)/CT showed accumulation in a mass lesion with SUV max 12.64 in the right lower lobe S10. Accumulation in lymph nodes was as follows: #1R (SUV max 13.15), #4R (SUV max 5.52), #7 (SUV max 8.97) (Figure 5).
Brain MRI showed no significant occupying lesion.
Although FDG-PET/CT showed accumulation in the mediastinal lymph nodes, a thoracic surgeon considered that lymph node dissection could be performed via a right thoracic approach. However, because pleural dissemination was noted intraoperatively, only an exploratory thoracotomy was performed. The postoperative diagnosis was pT2aN3M1a, stage IV. The patient is currently undergoing chemotherapy.
The authors obtained the patient’s consent for publication of details of his case.
Discussion
Calcification detected by image, which may be central, layered, hole, diffuse, or popcorn-like, strongly suggests that a nodular shadow in the lung is benign.7
Gross calcification is usually associated with benign lesions such as ectopic calcification due to old inflammation and bone or cartilage formation. However, calcification or bone formation occurs in lung cancer or sarcoma.
Mahoney et al.2 reported that chest CT showed calcification in 5.7% of 353 patients with lung cancer. Grewal et al.3 reported detecting calcification in 10.6% of 500 patients. Okimoto et al.4 reported detecting calcification in 5.6% of 320 patients with tumors of confirmed histological types. These findings suggest that 5% to 10% of lung cancers are associated with calcification.
When a lung nodule or mass shadow is accompanied by gross calcification, care should be taken to distinguish between benign and malignant lesions. As in the present case, when high concentrations of tumor markers or imaging findings suggestive of malignancy are observed, it is necessary to make a definitive diagnosis by performing examinations like a bronchoscopy rather than merely following the patient up.
Unfortunately, our patient’s tumor could not be removed to determine whether the gross calcification seen on image represented bone formation. It is difficult to distinguish between calcification and bone formation purely on the basis of imaging studies; thus, definitive diagnosis of bone formation is difficult in the absence of a large surgical specimen. Lung cancer with bone formation is exceedingly rare: to the best of our knowledge, only 13 cases8–12 have been reported. These patients comprised nine men and four women of average age 63 years. The histologic types were one squamous cell carcinoma, one adenosquamous cell carcinoma, and 11 adenocarcinomas. Kuribayashi et al. reviewed 2269 surgically resected primary lung carcinomas and identified 33 (about 1.5%) with heterotopic ossification, including 15 with intratumoral heterotopic ossification and 18 with extratumoral heterotopic ossification. All cases with intratumoral heterotopic ossification were adenocarcinomas.13
Lung cancers with bone formation are believed to progress slowly and reportedly have a good prognosis if diagnosed at an early stage.14 However, our patient’s tumor progressed quickly; thus, the prognosis of lung cancer with gross calcification is not necessarily good. More cases need to be accumulated.
Acknowledgments
The authors thank Takashi Suda (Department of Respiratory Surgery) and Makoto Kuroda (Department of Clinical Pathology) for participating in a discussion of this report. They also thank Dr Trish Reynolds, MBBS, FRACP, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.
Notes
Conflict of Interest
None of the authors have any actual or perceived conflicts of interest of a financial nature regarding the work in this manuscript.
References
- 1. Kusumoto M. Diagnostic imaging of unusual lung tumors. Japanese Journal of Lung Cancer 2015; 55: 1037–1044 (in Japanese).
- 2. Mahoney MC, Shipley RT, Corcoran HL, Dickson BA. CT demonstration of calcification in carcinoma of the lung. AJR Am J Roentgenol 1990; 154: 255–258.
- 3. Grewal RG, Austin JH. CT demonstration of calcification in carcinoma of the lung. J Comput Assist Tomogr 1994; 18: 867–871.
- 4. Okimoto N, Asaoka N, Fujita K. Computed tomography of lung cancer: Frequency and characteristics of calcification. Internal Medicine 2003; 42: 906–907.
- 5. Boh S, Kamimura R, Tsujimoto M, Okada E, Watanabe A. A case of pulmonary carcinosarcoma with calcification in the tumor observed on computed tomography. Japanese Journal of Lung Cancer 2012; 52: 27–31 (in Japanese).
- 6. Hasegawa T, Okabe N, Yaginuma H, Ohsugi J, Higuchi M, Suzuki H. A case of primary pulmonary synovial sarcoma initially diagnosed as a benign lung tumor due to calcification of the tumor. The Journal of the Japanese Association for Chest Surgery 2014; 28: 488–494 (in Japanese).
- 7. Oikado K, Tominaga J, Sato Y. Hai no sekkaika kotsuka.( Calcification and bone formation in lung). Clinical Imagiology 2015; 31: 1124–1139 (in Japanese).
- 8. Sakon K, Sasaki M, Okada A, Ikeda T, Imamura Y. A case of primary adenosquamous carcinoma of the lung with marked bone formation. The Journal of the Japanese Association for Chest Surgery 2014; 28: 109–114 (in Japanese).
- 9. Hino Y, Kaji M, Miyahara N, Kobayashi R, Suemasu K. Primary lung adenocarcinoma with stromal ossification showing slow growth. Japanese Journal of Lung Cancer 2012; 52: 393–396 (in Japanese).
- 10. Ueshima Y, Kurioka H, Yamada R, Takumi C, Hiraoka N, Ono S. The Journal of the Japanese Respiratory Society 2005; 43: 523–526 (in Japanese).
- 11. Kato F, Iwasaki A, Miyoshi T, Nakajima H, Hirayama T, Yamamoto S, Hiratsuka M, Shiraishi T, Shirakusa T, Hayashi H. A case of primary adenocarcinoma of the right lung with ossification. The Journal of the Japanese Association for Chest Surgery 2006; 6: 856–859 (in Japanese).
- 12. Tsuchiya T, Nishimura Y, Funada Y, Nakajima T, Hozumi A, Kotani Y, Nishiuma T, Matsumoto K, Ohbayashi C, Yokoyama M. Pulmonary adenocarcinoma with central ossification. The Journal of the Japanese Respiratory Society 2000; 38: 283–287 (in Japanese).
- 13. Kuribayashi H, Tsuta K, Mizutani E, Maeshima AM, Yoshida Y, Gemma A, Kudoh S, Asamura H, Matsuno Y. Clinicopathological analysis of primary lung carcinoma with heterotopic ossification. Lung Cancer 2009; 64: 160–165.
- 14. Zhang Q, Yin L, Li B, Meng R, Dao R, Hu S, Qiu X. Pulmonary adenocarcinoma with osseous metaplasia: a rare occurrence possibly associated with early stage? Onco Targets Ther 2013; 6: 1631–1634.