ABSTRACT
Background: On 11 March 2011, the Great East Japan Earthquake followed by a powerful tsunami hit the Pacific Coast of Northeast Japan and damaged Tokyo Electric Power Company’s Fukushima Daiichi Nuclear Power Plant, causing a radiation hazard in Fukushima Prefecture. The objective of this report is to describe some results of a questionnaire-based pregnancy and birth survey conducted by the Radiation Medical Science Center for the Fukushima Health Management Survey.
Materials and Methods: Questionnaires were sent to women who received maternal and child health handbooks from municipal officers in Fukushima Prefecture between 1 August 2010 and 31 July 2011, with the aim of reaching those who were pregnant at the time of the disaster. Mailing began 18 January 2012. Data were analyzed separately for six geographic areas in Fukushima Prefecture.
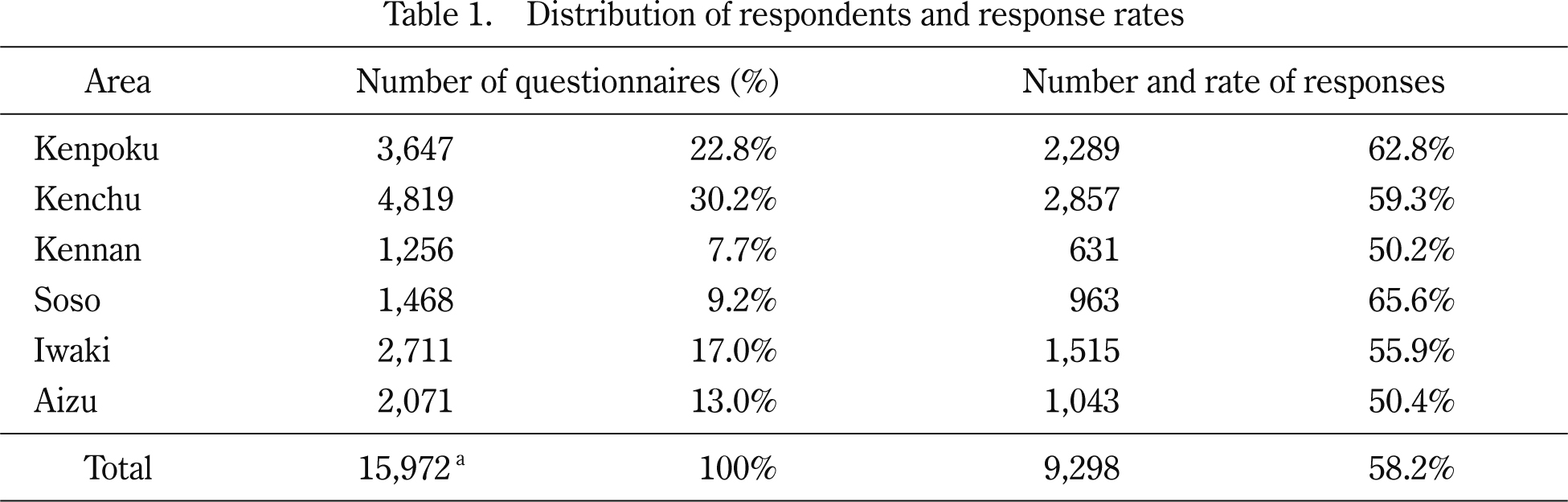
Results: The total number of women meeting survey criteria was 15,972. The number of responses received to date is 9,298 (58.2%). Data from 8602 respondents were analyzed after excluding 634 invalid responses and 5 induced and 57 spontaneous abortions (less than 22 gestational weeks). The incidences of stillbirth (over 22 completed gestational weeks), preterm birth, low birth weight and congenital anomalies were 0.25%, 4.4%, 8.7% and 2.72%, respectively. These incidences are similar to recent averages elsewhere in Japan.
Conclusion: Considering the pregnancy and birth survey data in aggregate, our disaster seemed to provoke no significant adverse outcomes over the whole of Fukushima prefecture. But post-disaster prenatal care and support intended for patients’ safety and security should be coupled with ongoing surveillance and rigorous data analysis.
INTRODUCTION
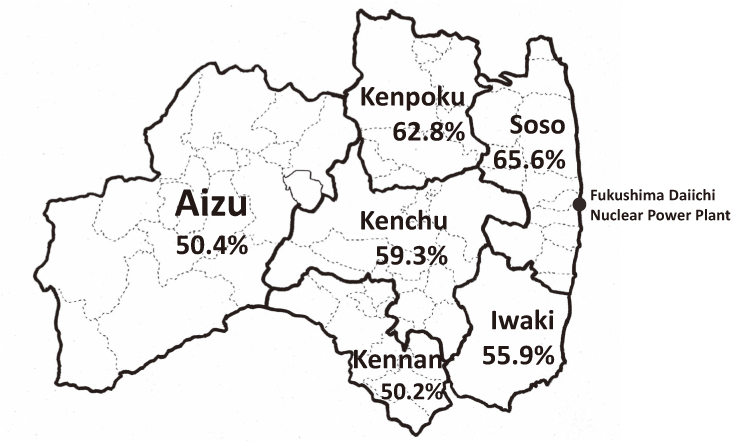
The Great East Japan Earthquake occurred on 11 March 2011. After that a powerful tsunami hit the Fukushima Daiichi Nuclear Power Plant, thereby causing a radiation hazard in Fukushima prefecture. The radioactive plume from the damaged nuclear power plant was carried north, along with wind and rain, toward the prefecture’s most populated Kenpoku area1). Soon after the disaster, the Fukushima prefectural government launched the Fukushima Health Management Survey to investigate long-term low-dose radiation exposure caused by the accident2).
The pregnancy and birth survey, one of 4 detailed surveys comprising the Fukushima Health Management Survey, aimed to collect data that might improve obstetrical and prenatal care, and to support women who were pregnant or delivered babies in Fukushima prefecture during and after the disaster2).
In general, disasters potentially influence a range of reproductive and birth outcomes. Even without direct exposure to a disaster, circumstances may lead to an increased risk of adverse outcomes, -for instance, more unplanned pregnancies and sexually transmitted infections3). However, the literature on disasters indicates limited effects on birth outcomes. Several studies of terrorist attacks4-9), nuclear reactor accidents10-16), and natural disasters (earthquakes17-20) and hurricanes21,22)) have been identified. Disasters of various types may affect on fetal growth, although there is no clear causal link to shortened gestation or preterm birth3).
The objective of this report is to describe some results of a pregnancy and birth survey after the disaster based on questionnaires from the Radiation Medical Science Center for the Fukushima Health Management Survey.
MATERIALS AND METHODS
This pregnancy and birth survey sought women who received maternal and child health handbooks from municipal officers in Fukushima Prefecture between 1 August 2010 and 31 July 2011, and women who had handbooks issued in other prefectures but received prenatal care or delivered babies in Fukushima Prefecture after the disaster. The objective was to reach women who were pregnant at the time of the disaster. This survey was approved by the ethics committee of Fukushima Medical University, which is guided by local policy, national law, and the World Medical Association Declaration of Helsinki (approval #13047).
Questionnaires, which can be seen on our web site23), have been mailed out since 18 January 2012. A total of 16,001 questionnaires were ultimately distributed.
General demographic and perinatal outcome data include, maternal age, parity, gestational age at delivery, whether preterm (22-37 gestational weeks), birth weight itself and normal vs. low birth weight (less than 2,500 g), live birth vs. stillbirth (fetal deaths at 22 completed weeks and over of gestation) and delivery mode. Major congenital anomalies recorded include, cataract, cardiac malformation, kidney or urinary tract malformation, spina bifida, microcephaly, hydrocephalus, cleft lip or palate, intestinal atresia (esophagus, duodenum, ileum), imperforate anus, and poly or syndactylism.
Data were also analyzed in aggregate and in six geographic areas (Kenpoku, Kenchu, Kennan, Soso, Iwaki and Aizu: Fig. 1).
Demographic and perinatal outcome data of the subjects are presented as mean +/− one standard deviation or as incidences where appropriate. Discrepancies with the total number of valid respondents exist because there were missing data in each subject area.
For statistical comparisons, Pearson’s chi-square test followed by residual analysis were applied to incidences of stillbirth, preterm delivery, low birth weight and congenital anomalies. The significance level was set at p<0.05. Data analyses were performed by SPSS ver. 21.0 (IBM Japan, Tokyo).
RESULTS
The number of responses as of 31 March 2013, excluding 29 outside Fukushima, was 9,298 (58.2%) (Table 1). The number of responses by geographic area appear in Table 1. The data of 8602 respondents considered for this report exclude 634 invalid responses (5 no answer, 1 death of participant, 20 multiple responses, 32 inconsistent answers, 460 deliveries before 11 March 2011, and 116 during pregnancy) and 5 induced and 57 spontaneous abortions (less than 22 gestational weeks). The response rates were highest in Soso (where the Fukushima Daiichi Nuclear Power Plant is located), Kenpoku and Kenchu (downwind of the major over-land radiation plume). See Table 1 and Fig. 1.
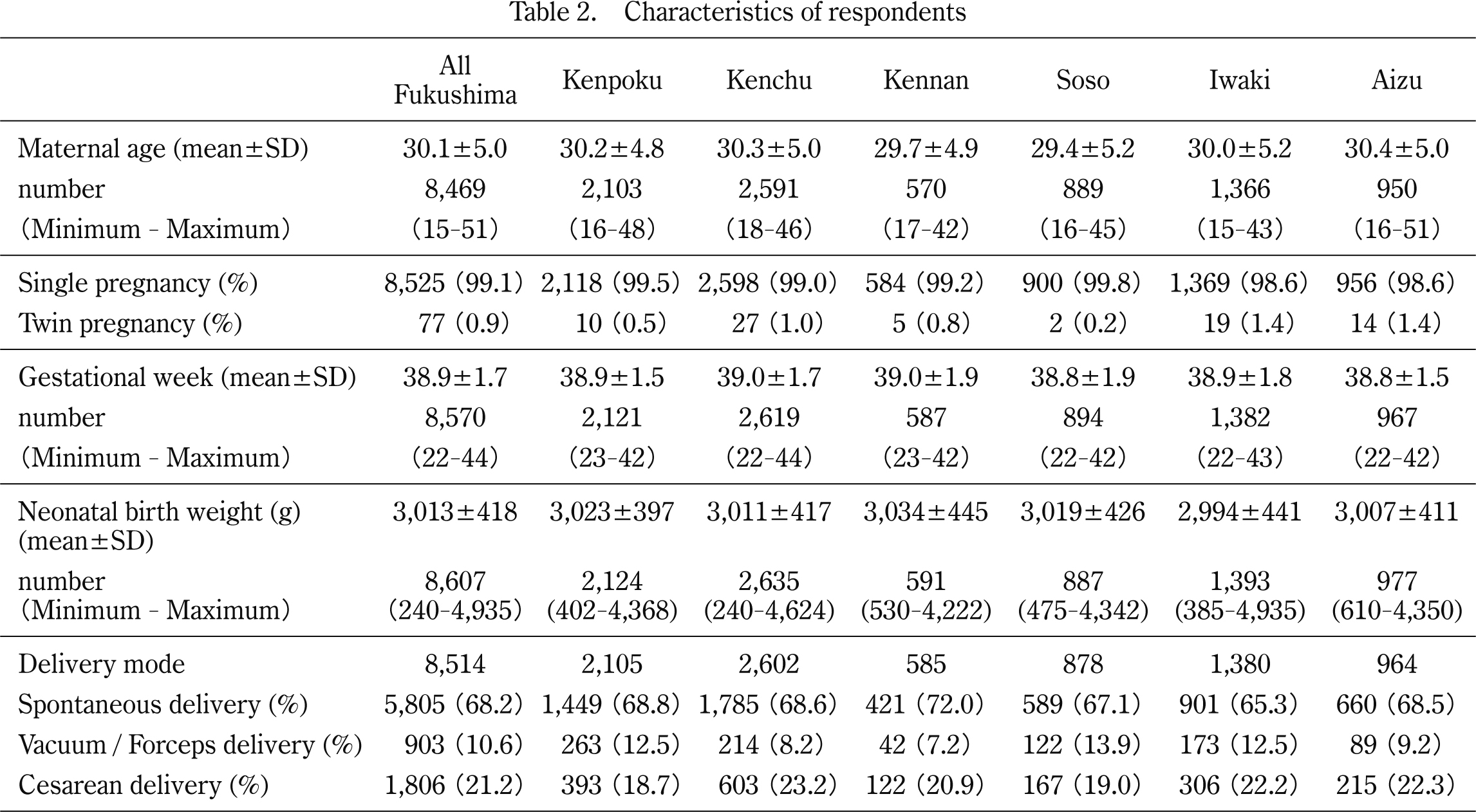
Table 2 shows demographic and perinatal outcomes. The overall mean maternal age was 30.1±5.0, but lower in Soso and Kennan. The twin pregnancy rate was 0.9%, and higher in Iwaki and Aizu. The overall gestational age at delivery was 38.9±1.7 weeks, with no difference seen among geographic areas. The overall mean neonatal birth weight was 3,013±418 g, but lower in Iwaki. The overall rate of cesarean delivery was 21.2%, but lower in Kenpoku and higher in Kenchu.
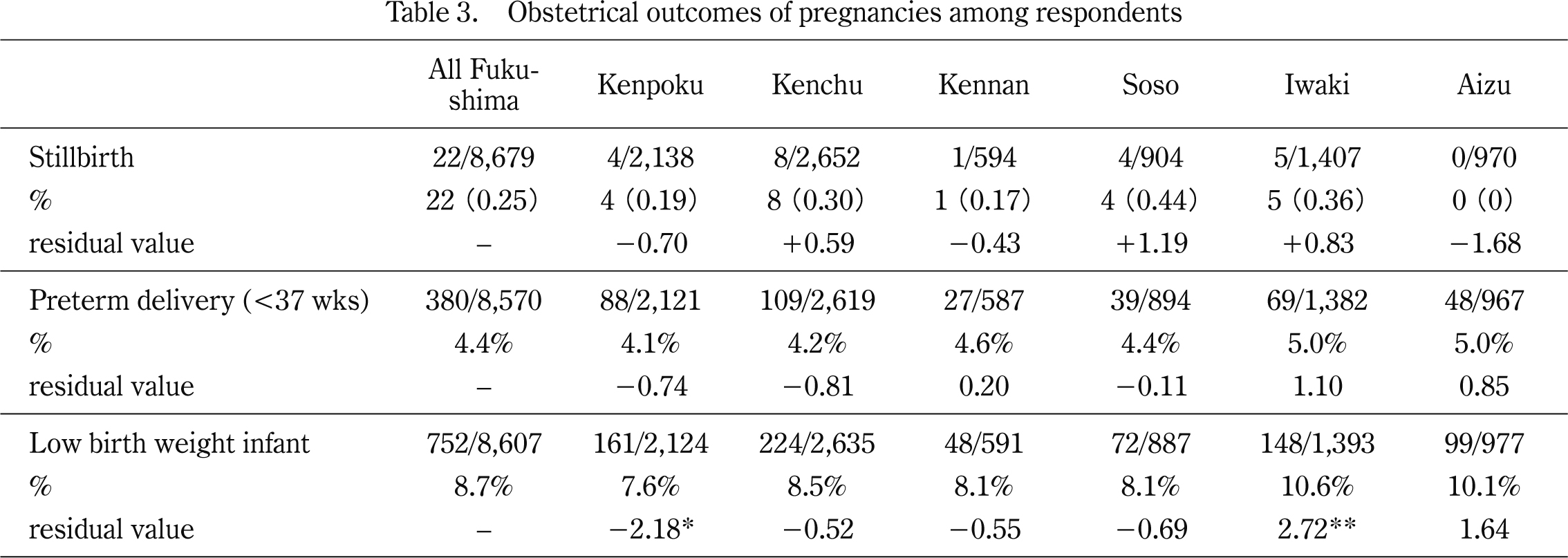
Table 3 shows obstetrical outcomes of pregnancies among respondents. The overall incidences of stillbirths, preterm birth and low birth weight infants were 0.25%, 4.4% and 8.7%, respectively. By area, there were no significant differences in the rate of stillbirth (p=0.399) or preterm delivery (p=0.766). However, the incidence of low birth weight varied, being significantly lower in Kenpoku and higher in Iwaki.
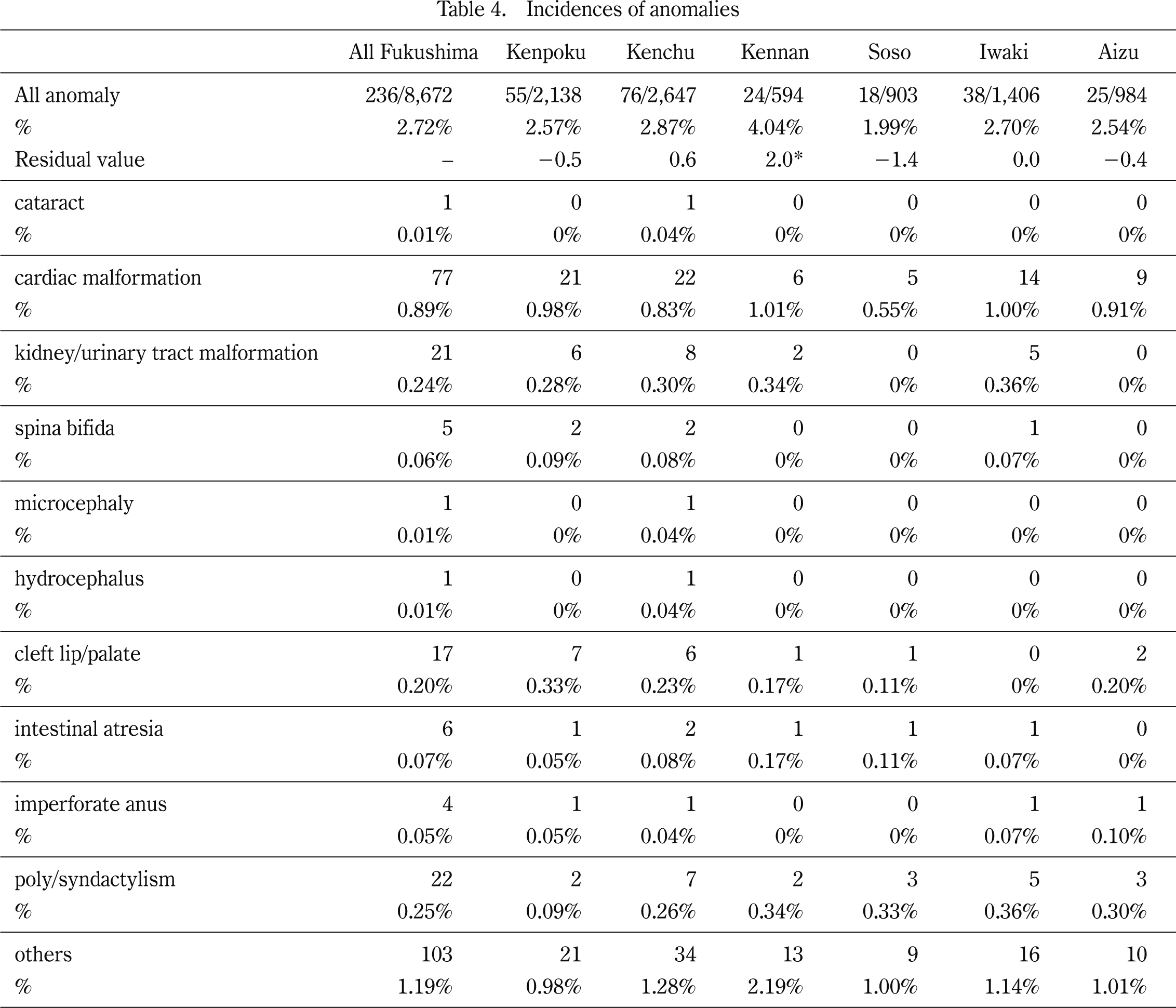
Table 4 shows the incidence of congenital anomalies in each area. The overall incidence of congenital anomalies was 2.72%. The highest incidence of any anomaly was cardiac malformation at 0.89%. There were no significant differences of anomaly by region (p=0.275). However, the incidence of all anomalies in Kennan was significantly higher by residual analysis.
DISCUSSION
The Radiation Medical Science Center conducted a cohort study of all people living in Fukushima Prefecture after the earthquake: a basic survey (to estimate external radiation exposure) and 4 detailed surveys. The detailed surveys comprise a thyroid ultrasound examination for all Fukushima children aged 18 years or younger, a comprehensive health check for all residents from the evacuation zones, an assessment of mental health and lifestyles of all residents from the evacuation zones, and the pregnancy and birth survey described herein2). This long-term large-scale epidemiologic study is expected to provide valuable data in the investigation of the health effects of low-dose radiation and disaster-related stress.
In this report, in the entire Fukushima Prefecture, the post-disaster incidences of stillbirth, preterm birth, low birth weight and congenital anomalies were 0.25%, 4.4%, 8.7% and 2.72%, respectively. These incidences are similar to recent averages in Japan. By area, there were no significant differences in the rate of stillbirth or preterm delivery. However, the incidence of low birth weight varied, being significantly lower in Kenpoku and higher in Iwaki. The reasons for these significant differences are unclear. It will be necessary to examine birth weights by the multiple factor analysis including maternal complications.
The incidence of stillbirth is gradually decreasing in Japan as quality perinatal care improves. In 2011, the incidence of stillbirth was 0.33%24). However, the incidence of preterm birth and low birth weight are gradually and slowly increasing in Japan as more high risk pregnancies occur such as advanced maternal age and medical complicated pregnancies. In 2011, the incidences of preterm birth and low birth weight were 5.7%25) and 9.6%26), respectively.
Disasters, in and of themselves, potentially influence various aspects of perinatal health. The Chinese Wenchuan earthquake, which caused nearly 70,000 deaths in 2008, was associated with many birth complications, including higher rates of low birth weight, preterm birth, birth defects, and lower Apgar scores in a large study of survivors17). The Taiwan earthquake of 1999 was also associated with high levels of low birth weight and psychiatric distress, but no changes in birth length, in a hospital-based cohort 18). Pregnant women, who had experienced the 1994 Northridge earthquake in California, gave birth earlier than expected, and the effect was strongest for those exposed in the first trimester19). An increase in preterm delivery was seen in one hospital after 2 of 5 Israeli earthquakes20). Through these observations, we could conclude no significant adverse outcomes in a pregnancy and birth survey of Fukushima Prefecture after our disaster. Moreover, these results suggest that routine pregnancies in Fukushima received appropriate prenatal care after the disaster.
The overall incidence of congenital anomalies in Fukushima was 2.72%. There were no significant differences in all congenital anomalies or each malformation in the prefecture as a whole or in each geographic area except Kennan (by residual analysis). The lowest number of births in Kennan seemed to have accidentally induced the increased incidence of all anomalies.
In general, the World Health Organization reports congenital anomalies (also referred to as birth defects) as affecting approximately 1 in 33 infants (3.33%)27). In Japan, the percentage of birth defects was reported to be 2.31% in 2010 according to a report of the ICBDMS Japan Center28).
Several prominent environmental or technical disasters have been reported about congenital anomalies. These include the nuclear reactor accidents at Chernobyl, Ukraine, in 1986 and at Three Mile Island, Pennsylvania, in 1979. Chernobyl involved a much larger radiation leak and affected many more people than Three Mile Island or Fukushima. Reviews of the effects of the Chernobyl disaster indicate increased rates of microcephaly and neural tube defects11); however, most birth defects did not increase in most countries12-15). Although the data for the most exposed areas are limited11), a suggestion of an increase in congenital anomalies in the immediate vicinity of Chernobyl has been reported16). The World Health Organization concluded in the “Health Effects of the Chernobyl Accident and Special Health Care Program 2006” that the Chernobyl accident did not significantly increase neonatal anomalies or stillbirths related to radiation exposure29).
Finally, although it is possible to underestimate incidences when using a self-administered questionnaire with variable response rate, we could conclude no significant adverse outcomes from the pregnancy and birth survey over the whole Fukushima prefecture after the disaster. Residents in Fukushima are still suffering from the catastrophe caused by the Great East Japan Earthquake, which was followed by a powerful tsunami and the Fukushima Daiichi Nuclear Power Plant accident. Furthermore, another type of damage was the created by the nuclear accident in the form of ‘fuhyohigai’, which is defined as economic, psychological and political damage attributed to baseless rumors or confused public anxiety under extreme disasters of this scale. Although pregnancy and birth survey data in aggregate showed no statistical anomalies, post-disaster prenatal care and support intended for patients’ safety, security, and normalization of living conditions should be coupled with ongoing surveillance and rigorous data analysis.
APPENDIX
The Fukushima Health Management Survey Group Chairpersons:
Masafumi Abe (Executive Director, Radiation Medical Center for the Fukushima Health Management Survey); Shunichi Yamashita, Kenji Kamiya, and Seiji Yasumura (Senior Directors, Radiation Medical Center for the Fukushima Health Management Survey); Makoto Akashi (National Institute of Radiological Sciences); Kazunori Kodama and Kotaro Ozasa (The Radiation Effects Research Foundation).
REFERENCES
- 1. Nagata T, Kimura Y, Ishii M. Use of a geographic information system (GIS) in the medical response to the Fukushima nuclear disaster in Japan. Prehosp Disaster Med, 27: 213-215, 2012.
- 2. Yasumura S, Hosoya M, Yamashita S, et al. Fukushima Health Management Survey Group. J Epidemiol, 22: 375-383, 2012.
- 3. Harville E, Xiong X, Buekens P. Disasters and perinatal health: a systematic review. Obstet Gynecol Surv, 65: 713-728, 2010.
- 4. Perera FP, Tang D, Rauh V, et al. Relationships among polycyclic aromatic hydrocarbon-DNA adducts, proximity to the World Trade Center, and effects on fetal growth. Environ Health Perspect, 113: 1062-1067, 2005.
- 5. Berkowitz GS, Wolff MS, Janevic TM, Holzman IR, Yehuda R, Landrigan PJ. The World Trade Center disaster and intrauterine growth restriction. JAMA, 290: 595-596, 2003.
- 6. E Endara SM, Ryan MA, Sevick CJ, Conlin AM, Macera CA, Smith TC. Does acute maternal stress in pregnancy affect infant health outcomes? Examination of a large cohort of infants born after the terrorist attacks of September 11, 2001. BMC Public Health, 9: 252, 2009.
- 7. Lauderdale DS. Birth outcomes for Arabic-named women in California before and after September 11. Demography, 43: 185-201, 2006.
- 8. Lederman SA, Rauh V, Weiss L, et al. The effects of the World Trade Center event on birth outcomes among term deliveries at three lower Manhattan hospitals. Environ Health Perspect, 112: 1772-1778, 2004.
- 9. Maric NP, Dunjic B, Stojiljkovic DJ, Britvic D, Jasovic-Gasic M. Prenatal stress during the 1999 bombing associated with lower birth weight-a study of 3,815 births from Belgrade. Arch Womens Ment Healt, 13: 83-89, 2010.
- 10. Goldhaber MK, Staub SL, Tokuhata GK. Spontaneous abortions after the Three Mile Island nuclear accident: a life table analysis. Am J Public Health, 73: 752-759, 1983.
- 11. Wertelecki W. Malformations in a chornobyl-impacted region. Pediatrics, 125: e836-843, 2010.
- 12. Little J. The Chernobyl accident, congenital anomalies and other reproductive outcomes. Paediatr Perinat Epidemiol, 7: 121-151, 1993.
- 13. Hoffmann W. Fallout from the Chernobyl nuclear disaster and congenital malformations in Europe. Arch Environ Health, 56: 478-484, 2001.
- 14. Dolk H, Nichols R. Evaluation of the impact of Chernobyl on the prevalence of congenital anomalies in 16 regions of Europe. EUROCAT Working Group. Int J Epidemiol, 28: 941-948, 1999.
- 15. Zafra Anta MA, Amor Cabrera MA, Díaz Mier F, Cámara Moraño C. Health effects of the Chernobyl disaster. Fifteen years afterwards. (in Spanish) An Esp Pediatr, 56: 324-333, 2002.
- 16. Feshchenko SP, Schröder HC, Müller WE, Lazjuk GI. Congenital malformations among newborns and developmental abnormalities among human embryos in Belarus after Chernobyl accident. Cell Mol Biol, (Noisy-le-grand) 48: 423-426, 2002.
- 17. Tan CE, Li HJ, Zhang XG, et al. The impact of the Wenchuan earthquake on birth outcomes. PLoS One, 4: e8200, 2009.
- 18. Chang HL, Chang TC, Lin TY, Kuo SS. Psychiatric morbidity and pregnancy outcome in a disaster area of Taiwan 921 earthquake. Psychiatry Clin Neurosci, 56: 139-144, 2002.
- 19. Glynn LM, Wadhwa PD, Dunkel-Schetter C, Chicz-Demet A, Sandman CA. When stress happens matters: effects of earthquake timing on stress responsibility in pregnancy. Am J Obstet Gynecol, 184: 637-642, 2001.
- 20. Weissman A, Siegler E, Neiger R, Jakobi P, Zimmer EZ. The influence of increased seismic activity on pregnancy outcome. Eur J Obstet Gynecol Reprod Biol, 31: 233-236, 1989.
- 21. Xiong X, Harville EW, Mattison DR, et al. Exposure to Hurricane Katrina, post-traumatic stress disorder and birth outcomes. Am J Med Sci, 336: 111-115, 2008.
- 22. Hamilton BE, Sutton PD, Mathews TJ, et al. The effect of Hurricane Katrina: Births in the US Gulf Coast region, before and after the storm. Natl Vital Stat Rep, 58: 1-32, 2009.
- 23. Questionnaire for Pregnancy and Birth Survey: http://www.fmu.ac.jp/univ/chiiki/health_survey/pdf/maternal/01_3.pdf
- 24. Foetal Deaths and Foetal Death Rates at 22 Completed Weeks and Over of Gestation by Prefecture. In: Maternal and child health statistics of Japan. Mother’s & Children’s Health Organization, p90, 2013.
- 25. Live Births and Percentages by Period of Gestation, 1980-2011. In: Maternal and child health statistics of Japan. Mother’s & Children’s Health Organization, p49, 2013.
- 26. Live Births and Percentages by Birthweight and Sex, 1951-2011. In: Maternal and child health statistics of Japan. Mother’s & Children’s Health Organization, p45, 2013.
- 27. Congenital anomalies in WHO homepage; http://www.who.int/mediacentre/factsheets/fs370/en/
- 28. International Clearing House for Birth Defects Monitoring Systems(ICBDMS) Japan Center: http://www.icbdsrj.jp/data.html, in Japanese, accessed January 2014
- 29. Bennett B, Repacholi M, Carr Z. Health effects of the Chernobyl accident and special health care programmes. Report of the UN Chernobyl Forum Expert Group “Health”. Geneva: World Health Organization; 2006.