Abstract
Symptomatic thoracic disc herniation is clinically rare. There are few cases of disc herniation of the thoracic spine in top athletes described in the literature. We herein present a rare case of chest wall pain due to thoracic disc herniation in a professional baseball pitcher. A 30-year-old, left-handed pitcher complained of left-sided chest wall pain in the region of his lower ribs during a game. Neurological examination revealed hypoesthesia of the left side of the chest at the level of the lower thoracic spine. Magnetic resonance imaging (MRI) of the thoracic spine showed a left-sided paramedian disc herniation at the T9-T10 level. The player was initially prescribed rest, administration of pregabalin (150 mg twice a day), and subsequent physical rehabilitation. He was able to resume full training and pitching without medication 6 months after the onset. A follow-up MRI of the thoracic spine showed a reduction in the size of the herniated disc compared to the initial findings. Though relatively rare, thoracic disc herniation should be considered in cases of chest wall pain in athletes.
Introduction
Symptomatic thoracic disc herniation is clinically rare. There are few cases of disc herniation of the thoracic spine in top athletes described in the literature1-4). The clinical presentation of a thoracic disc herniation can vary widely depending on its location and morphologic characteristics1). The most common initial symptom described is thoracic pain occurring midline, unilaterally, or bilaterally, or in a radicular distribution, followed later by sensory and motor disturbances2,3,5).
Herein, we present a case of chest wall pain due to thoracic disc herniation in a professional baseball pitcher.
Case Presentation
This case is that of a 30-year-old, left-handed, Japanese professional baseball pitcher. He trained 6 times a week at a top-professional level, and his past history was significant for a previous injury resulting in an episode of low back pain a few years earlier. Before the season started, he tried to change his throwing style from three-quarter delivery to a sidearm delivery, in which the arm arcs laterally to the torso. Four months after the season started, he complained of the onset of back and left-sided chest wall pain and a pulling sensation in the region of the lower ribs during a game. He experienced aggravation of the pain by lateral bending, rotation and flexion of the trunk and the act of coughing, but he denied any numbness or weakness when examined by the team trainer. There was no local tenderness or bruising. He was referred to a local hospital on the suspicion of a spontaneous pneumothorax, abdominal core muscle injury, or a rib fracture. However, the x-ray, CT, and MRI studies ordered to explore these differential diagnoses were all normal, and a tentative diagnosis of rib cage and back muscle strain was made. He continued to throw approximately 20-30 times in games, twice a week for one month, on a farm team, while receiving non-steroidal anti-inflammatory drugs orally. One month after the onset, he started to feel numbness and radicular pain on the left side, at the lower thoracic level (almost T9-T11), and he was referred to our institution.
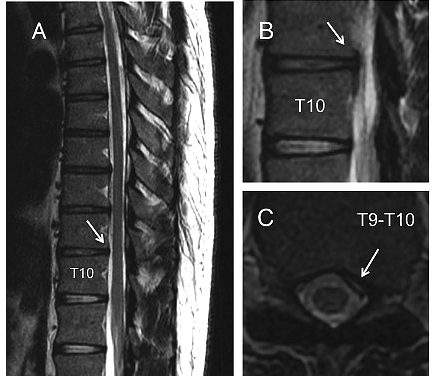
On physical examination by an orthopedic surgeon, the thoracic radicular pain was exacerbated by bending forward. Neurological examination revealed hypoesthesia of the left side of the chest at the level of the lower thoracic spine. Therefore, a possible thoracic disc herniation was suspected. This suspicion was confirmed by magnetic resonance imaging (MRI) of the thoracic spine, on which a left-sided paramedian disc herniation at the T9-T10 level was found (Figure 1).
He was initially prescribed two weeks’ rest with administration of pregabalin (150 mg twice a day). The pregabalin was effective for his numbness and radicular pain (pain on numerical rating scale recovered from 7.0 to 1.0), and he subsequently gradually increased his physical exercise. He had no further symptoms during rehabilitation to the level of full training. He resumed full training and pitching in top condition without medication‚ 6 months after the onset. A follow-up MRI of the thoracic spine showed a reduction in the size of the herniated disc compared to the initial findings (Figure 2).
Discussion
In this report, we present a rare case of chest wall pain secondary to thoracic disc herniation in a professional baseball pitcher. We recognized two important clinical issues. First, thoracic disc herniation can cause chest wall pain in athletes. Second, a detailed neurological examination and thoracic spine MRI confirmation are both useful for the diagnosis of this condition.
Thoracic disc herniation is an uncommon cause of chest wall pain2,3,5,6); however, it can cause chest wall pain in athletes. Despite the prevalence of thoracic disc degeneration using MRI assessments was almost 15% in men aged <50 years and rose to 80% in men aged ≥80 years7), the incidence of symptomatic thoracic disc herniation reported in the literature is between 0.25% and 0.75% of all intervertebral disc herniations3,8-10), resulting in < 2% of all spinal disc surgeries performed3,8,11). Degeneration is the primary etiology of thoracic disc herniation, but acute trauma has also been reported to be an important factor, especially in young patients2,3). There are few studies that have evaluated the incidence of symptomatic thoracic disc herniation in professional athletes. During the 12 National Football League seasons (2000-2012) studied, only 4 thoracic disc herniations of 257 herniations (incidence of 2%) were detected4). Unlike lumbar or cervical disc herniations, thoracic disc herniations do not have a typical clinical presentation, and the symptoms may be acute, subacute, or chronic2,12). The symptoms experienced in athletes with chronic thoracic pain progressively deteriorate, usually starting with pain and progressing to neurological deficits of a varying degree13). The pain can be intermittent or constant and may be aggravated by coughing or straining. Thoracic disc herniation can radiate not only to the upper extremities, thoracic region, abdominal region, flanks, groin, and testicles, but also to the lower extremities2,13-20).
Additionally, a detailed neurological examination and MRI of the thoracic spine are useful in the diagnosis of this condition. Chest wall pain is relatively common in baseball players, and there are several causes such as abdominal oblique muscle injuries and rib fractures6,21,22). The physical findings of this case mimicked these injuries, except for the hypoesthesia of the left side of the chest. Pain due to a rib fracture may radiate along the distribution of the intercostal nerve, but sensory disturbances, such as hypoesthesia, are rare23). Immediate MRI and/or ultrasound evaluation are usually indicated to identify injured abdominal core muscles or rib fractures in professional baseball players for whom minimizing time spent on the Disabled List is important21,24). However, the MRI protocols for the evaluation of core muscles and rib bone are different from the protocol for the evaluation of the thoracic spine. Therefore, MRI of the thoracic spine should be considered for players who complain of chronic, unusual “side pain,” especially with a neurological deficit.
The majority of cases of thoracic disc herniation are successfully treated with conservative management, which was also tried in this case3,6). However, thoracic herniations lead to a significantly higher loss of playing time (almost half a year) than do cervical or lumbar disc herniations in athletes4). Although selective spinal root or intercostal nerve blockade and epidural steroid injections can be used to treat thoracic radiculopathy25), we used only administered pregabalin on the patient’s request. Moreover, we speculated that changing his throwing style from three-quarter delivery to a sidearm delivery that lead to increase thoracic kyphosis promotes the thoracic disc herniation caused by greater axial load with disc compression. Therefore, the rehabilitation was focused on the improvement of the mobility of the thoracic spine to keep the thoracic spine in relative extension in his new throwing style. The long-term prognosis of thoracic disc herniation has been considered to be good3,6), but not all cases have a good long-term outcome1). Long-term follow-up is needed.
In conclusion, thoracic disc herniation can cause chest wall pain in athletes, and detailed neurological examination and MRI confirmation are useful for the diagnosis of this condition. We must be aware that thoracic disc herniation can mimic abdominal oblique muscle injuries and rib fractures. Some thoracic disc herniations may remain unrecognized, and thus there may be many more “hidden” thoracic disc herniation cases among athletes. This report reminds physicians and trainers that MRI of the thoracic spine should be considered for chronic, unusual “side strain” cases, especially in young athletes with a neurological deficit.
Conflict of Interests
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Consent
The patient described in this paper has given his informed consent for the case report to be published.
References
- 1. Baranto A, Börjesson M, Danielsson B, Hellström M, Swärd L. Acute chest pain in a top soccer player due to thoracic disc herniation. Spine (Phila Pa 1976), 34(10): E359-362, 2009.
- 2. Arce A, Dohrmann J. Thoracic disc herniation. Improved diagnosis with computed tomographic scanning and a review of the literature. Surg Neurol, 23: 356-361, 1985.
- 3. Vanichkachorn J, Vaccaro A. Thoracic disc disease: diagnosis and treatment. J Am Acad Orthop Surg, 8: 159-169, 2000.
- 4. Gray L, Buchowski M, Bumpass B, Lehman A, Mall A, Matava J. Disc herniations in the National Football League. Spine (Phila Pa 1976), 38(22): 1934-1938, 2014.
- 5. Wilke A, Wolf U, Lageard P, et al. Thoracic disc herniation: a diagnostic challenge. Man Ther, 5: 181-184, 2000.
- 6. Gregory L, Biswas C, Batt E. Musculoskeletal problems of the chest wall in athletes. Sports Med, 32(4): 235-250, 2002.
- 7. Teraguchi, M, Yoshimura, N, Hashizume, H, et al. Prevalence and distribution of intervertebral disc degeneration over the entire spine in a population-based cohort: the Wakayama Spine Study. Osteoarthritis Cartilage, 22: 104-110, 2014.
- 8. Brown W, Deffer A Jr, Akmakjian J, et al. The natural history of thoracic disc herniation. Spine, 17: S97-102, 1992.
- 9. Carson J, Gumpert J, Jefferson A. Diagnosis and treatment of thoracic intervertebral disc protrusions. J Neurol Neurosurg Psychiatry, 34: 68-77, 1971.
- 10. Stone J, Lichtor T, Banerjee S. Intradural thoracic disc herniation. Spine, 19: 1281-1284, 1994.
- 11. Alvarez O, Roque CT, Pampati M. Multilevel thoracic disk herniations: CT and MR studies. J Comput Assist Tomogr, 12: 649-652, 1988.
- 12. Arseni C, Nash F. Thoracic intervertebral disc protrusion: a clinical study. J Neurosurg, 17: 418-430, 1960.
- 13. Fukuta S, Miyamoto K, Iwata A, Hosoe, H, Iwata, H, Shirahashi, K, Shimizu, K. Unusual back pain caused by intervertebral disc degeneration associated with Schmorl node at Th11/12 in a young athlete successfully treated by anterior interbody fusion: a case report. Spine (Phila Pa 1976), 34(5): E195-198, 2009.
- 14. Abbott H, Retter H. Protrusions of thoracic intervertebral disks. Neurology, 6: 1-10, 1956.
- 15. Epstein A. The syndrome of herniation of the lower thoracic intervertebral discs with nerve root and spinal cord compression. J Neurosurg, 11: 525-538, 1954.
- 16. Tahmouresie A. Herniated thoracic intervertebral disc─an unusual presentation: case report. Neurosurgery, 7: 623-625, 1980.
- 17. Ozturk C, Tezer M, Sirvanci M, et al. Far lateral thoracic disc herniation presenting with flank pain. Spine J, 6: 201-203, 2006.
- 18. LaBan M, Gorin G. A thoracic disc herniation presenting as an abdominal hernia. Am J Phys Med Rehabil, 86: 601, 2007.
- 19. Tokuhashi Y, Matsuzaki H, Uematsu Y, et al. Symptoms of thoracolumbar junction disc herniation. Spine, 26: E512-518, 2001.
- 20. Kuzma A, Doberstein T, Rushlow R. Postfixed brachial plexus radiculopathy due to thoracic disc herniation in a collegiate wrestler: a case report. J Athl Train, 48(5): 710-715, 2014.
- 21. Conte A, Thompson M, Marks A, Dines S. Abdominal muscle strains in professional baseball: 1991-2010. Am J Sports Med, 40(3): 650-656, 2012.
- 22. Karlson A. Thoracic region pain in athletes. Curr Sports Med Rep, 3(1): 53-57, 2004.
- 23. Miller L, Harris D, Kaeding C. Stress fractures of the ribs and upper extremities: causation, evaluation, and management. Sports Med, 43(8): 665-674, 2014.
- 24. Stevens J, Crain M, Akizuki H, Beaulieu F. Imaging and ultrasound-guided steroid injection of internal oblique muscle strains in baseball pitchers. Am J Sports Med, 38(3): 581-585, 2010.
- 25. O Conner C, Andray T, Russo B, et al. Thoracic radiculopathy. Phys Med Rehabil Clin N Am, 13: 623-644, 2002.