Abstract
Background: Atrial septal defect is the third most common type of congenital heart disease. Surgical closure was the standard treatment for atrial septal defects before transcatheter closure was approved as minimally invasive treatment in Japan in 2006. In our hospital, this procedure has been performed since 2015.
Objective: To evaluate the safety and effectiveness of transcatheter closure of atrial septal defects in our hospital.
Methods: Thirty patients (mean age 57.0 ± 19.7 years, 11 males), who underwent transcatheter closure of atrial septal defect between September 2015 and February 2018 at the Fukushima Medical University Hospital, were enrolled. All procedures were performed under general anesthesia with angiographic and transesophageal echocardiographic guidance. Safety and effectiveness were evaluated by the procedural results and complications.
Results: All 30 patients successfully underwent transcatheter closure of atrial septal defects and no patient developed complications. New York Heart Association functional class was improved, and the right ventricular area and right atrium area were decreased, postoperatively.
Conclusion: Transcatheter closure is a safe and effective treatment for atrial septal defects, and thus could be an alternative option to open heart surgery.
Introduction
Atrial septal defect is a common congenital heart disease and has two types: primum and secundum. Primum atrial septal defect is a variant of common atrioventricular canal defects. Secundum atrial septal defect is a defect that develops in the fossa ovalis due to the defective septum primum. Closure of atrial septal defects either percutaneously or surgically is indicated in patients with a hemodynamically significant shunt that causes enlargement of the right heart1).
Catheter intervention for structural heart disease has spread in recent years worldwide. Transcatheter closure of secundum atrial septal defects has been covered by public insurance in Japan since 2006. In Fukushima prefecture, transcatheter closure of atrial septal defects started from 2015 at Fukushima Medical University Hospital. We investigated the safety and effectiveness of transcatheter closure of atrial septal defects in our institution.
Methods
We enrolled 30 patients who underwent transcatheter closure of secundum atrial septal defects between September 2015 and February 2018. During this period, three patients were referred to our hospital due to atrial septal defects;however, they were not indicated for transcatheter closure because of small superior, inferior, or posterior rims by transesophageal echocardiography.
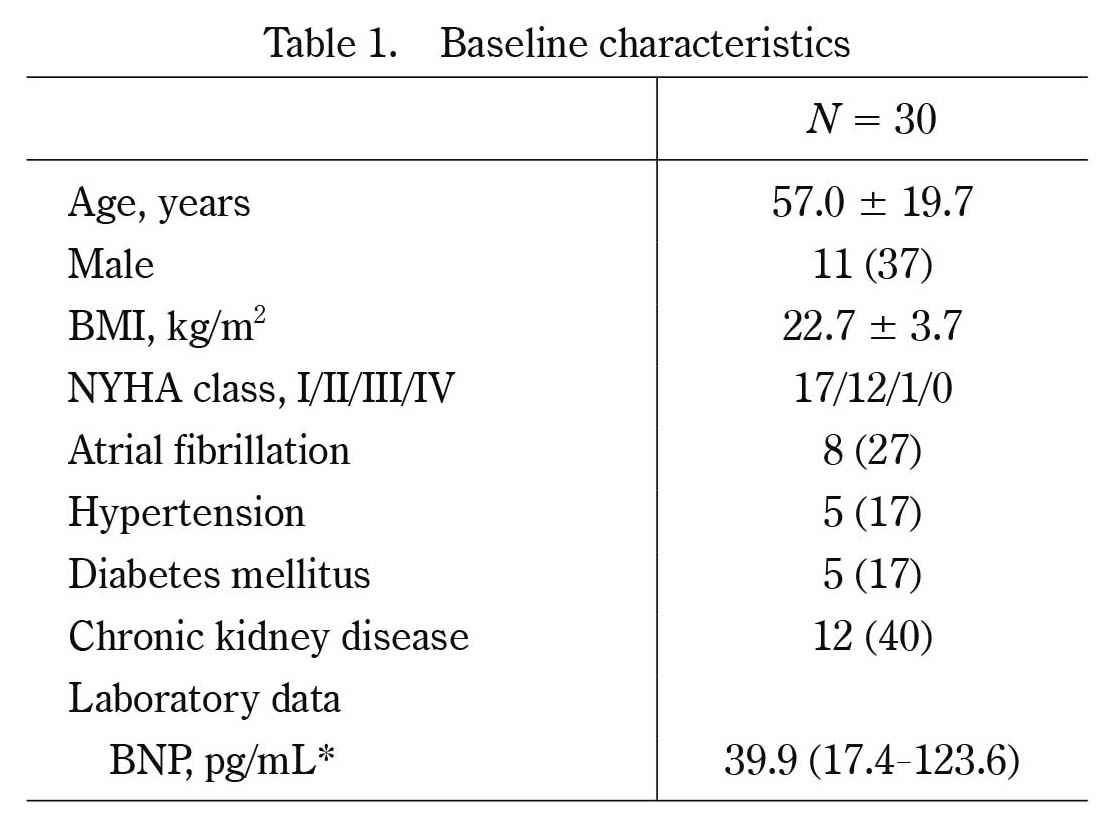
Baseline data including age, sex, body mass index, New York Heart Association class, past history, plasma levels of brain natriuretic peptide, echocardiographic findings, hemodynamic findings, and procedural data were collected.
Procedure of transcatheter closure of atrial septal defects is shown below. The implantation methods are similar between both devices of AmplatzerⓇ Septal Occluder (Saint-Jude Medical, Zaventem, Belgium) and FigullaⓇ Flex II ASD Occluder (Occlutech GmbH, Jena, Germany). All procedures were performed under general anesthesia with angiographic and transesophageal echocardiographic guidance. Before the procedure, we determined the size of occluder device by transesophageal echocardiography but not by a sizing balloon. First, a guide wire was inserted to the atrial septal defect through the right femoral vein. The occluder was screwed to the tip of the delivery cable, immersed in saline and drawn into the loader. A long guiding sheath and dilator were advanced over the guidewire through the atrial septal defect to the left atrium. After deployment of the left-sided disc in the left atrium, the system was pulled back. The occluder was thereafter fully deployed by withdrawing the sheath to expand the right atrial disc. Then, a residual shunt was evaluated by transesophageal echocardiography. Figure 1 shows an angiographic picture during the occluder deployment. The patients were discharged from the hospital 3 to 5 days after atrial septal occlusion. They received thienopyridine daily for a month and aspirin daily for 6 months. During the follow-up, blood sampling for brain natriuretic peptide measurement and transthoracic echocardiography were carried out at 1, 3, 6, and 12 months after atrial septal occlusion.
Data were analyzed using the Statistical Package for Social Sciences version 25 (SPSS Inc., Chicago, IL, USA). Continuous data are expressed as mean ± SD, and skewed data are presented as median and interquartile range. Categorical variables are expressed as numbers and percentages. The data were analyzed using Wilcoxon signed rank test. A P value of < 0.05 was considered statistically significant.
Results
The baseline characteristics of the 30 patients are shown in Table 1. The echocardiographic findings at baseline demonstrated preserved left ventricular systolic function, enlargement of right ventricle and both atria as shown in Table 2. The atrial septal defect diameter measured by transesophageal echocardiography was 18.6 ± 6.8 mm. The hemodynamic findings showed high mean pulmonary blood flow/systemic blood flow ratio of 2.30 ± 0.80. Five out of eight patients with atrial fibrillation underwent pulmonary vein isolation for atrial fibrillation before transcatheter closure of atrial septal defects.
All patients successfully underwent transcatheter closure. AmplazterⓇ Septal Occluder and FigullaⓇ Flex II ASD Occluder were used in 18 and 12 patients, respectively. No device-related complications were observed during the follow-up period of 312 ± 485 days (4 to 807 days) until April 2018 (Table 3). A slight residual shunt was detected immediately after atrial septal occlusion in all patients. However, among 22 patients, who underwent follow-up echocardiography 6 months after atrial septal occlusion, no residual shunt was detected. A septuagenarian patient with elevated brain natriuretic peptide of 506 pg/mL and mitral regurgitation before atrial septal occlusion needed additional diuretics treatment postoperatively.
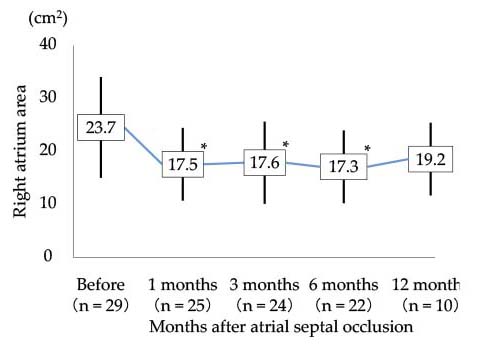
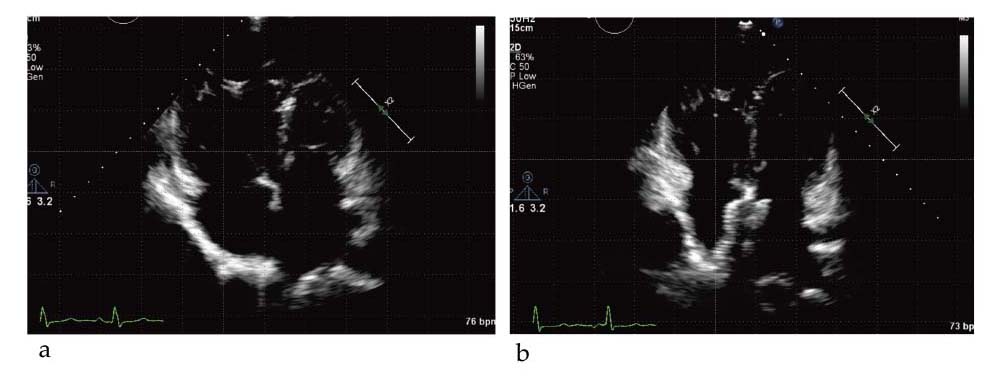
After atrial septal occlusion, New York Heart Association class was improved (Figure 2). Right ventricular diastolic area, tricuspid valve annular diameter, and right atrium area were decreased (Figures 3, 4, and 5). Tricuspid regurgitation peak gradient and brain natriuretic peptide levels were not significantly changed (Figures 6 and 7) and echocardiographic images showed decreased size of the right ventricle and right atrium after atrial septal occlusion (Figure 8).
Three patients had pulmonary hypertension defined as mean pulmonary artery pressure of ≥ 25 mmHg. Two out of the three patients showed decrease in pulmonary artery pressure estimated by tricuspid regurgitation peak gradient of echocardiography 3 months after atrial septal occlusion. The remaining patient had residual pulmonary hypertension 6 months after atrial septal occlusion.
Discussion
Atrial septal defect is the third most common type of congenital heart disease, with an estimated incidence of 56 per 100,000 livebirths2). In most patients, atrial septal defects lead to a left-to-right shunt. The shunt results in impaired right atrial function, right ventricular dilatation, and pulmonary hypertension3). Most patients with atrial septal defect remain asymptomatic throughout most of childhood. Adult patients with large defects present with symptoms, including fatigue, palpitations, syncope, shortness of breath, edema, manifestations of thromboembolism, and cyanosis4).
First surgical closure for atrial septal defects under direct vision was performed in 19525). In 1997, Sharafuddin, et al. published an article on AmplatzerⓇ Septal Occluder for transcatheter closure of atrial septal defects6). Subsequently, Cowley CG, et al. reported advantages of this occluder such as fewer complications and shorter hospitalization than surgery7). Recently, the FigullaⓇ ASD Occluder has been developed and shown similar outcomes compared with AmplatzerⓇ Septal Occluder8).
In the majority of cases, transcatheter occlusion is safe and effective;however, complications associated with this procedure for atrial septal defects have been reported. The reported incidence of complications ranges from 0% to 9.4%9-11), including device embolization, device malposition, and cerebrovascular events.
In Fukushima Prefecture, transcatheter closure of atrial septal defect has been approved only at Fukushima Medical University Hospital. The procedural results in the present study had no complication, showing the safety of the procedure. Echocardiographic data demonstrated a decrease in the right ventricular area and right atrium area, suggesting that atrial septal occlusion improved volume overload of the right heart.
A septuagenarian patient with mitral regurgitation and elevated brain natriuretic peptide needed additional diuretics treatment after atrial septal occlusion. We should be careful of left-sided volume loading after atrial septal occlusion.12)
A limitation in this study is that although the incidence of late complications after transcatheter atrial septal occlusion is low, long-term follow-up is needed to verify the safety. A previous case report showed erosion 4 years after atrial septal occlusion13). Another case report described device thrombosis that occurred 7 years after atrial septal occlusion14).
In conclusion, transcatheter closure is a safe and effective treatment for atrial septal defect.
Conflict of Interest Disclosure
Tetsuro Yokokawa belongs to endowed departments supported by Actelion Pharmaceuticals Japan Ltd. Akiomi Yoshihisa belongs to a department supported by Fukuda Denshi Co, Ltd.
References
- 1. Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease). Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol, 52: e143-263, 2008.
- 2. Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol, 39: 1890-1900, 2002.
- 3. Di Salvo G, Drago M, Pacileo G, et al. Atrial function after surgical and percutaneous closure of atrial septal defect: a strain rate imaging study. J Am Soc Echocardiogr, 18: 930-933, 2005.
- 4. Geva T, Martins JD, Wald RM. Atrial septal defects. Lancet, 383: 1921-1932, 2014.
- 5. Lewis FJ, Taufic M. Closure of atrial septal defects with the aid of hypothermia;experimental accomplishments and the report of one successful case. Surgery, 33: 52-59, 1953.
- 6. Sharafuddin MJ, Gu X, Titus JL, et al. Transvenous closure of secundum atrial septal defects: preliminary results with a new self-expanding nitinol prosthesis in a swine model. Circulation, 95: 2162-2168, 1997.
- 7. Cowley CG, Lloyd TR, Bove EL, et al. Comparison of results of closure of secundum atrial septal defect by surgery versus Amplatzer septal occluder. Am J Cardiol, 88: 589-591, 2001.
- 8. Pac A, Polat TB, Cetin I, et al. Figulla ASD occluder versus Amplatzer Septal Occluder: a comparative study on validation of a novel device for percutaneous closure of atrial septal defects. J Interv Cardiol, 22: 489-495, 2009.
- 9. Chessa M, Carminati M, Butera G, et al. Early and late complications associated with transcatheter occlusion of secundum atrial septal defect. J Am Coll Cardiol, 39: 1061-1065, 2002.
- 10. Jalal Z, Hascoet S, Baruteau AE, et al. Long-term Complications After Transcatheter Atrial Septal Defect Closure: A Review of the Medical Literature. Can J Cardiol, 32: 1315.e1311-1315.e1318, 2016.
- 11. Abaci A, Unlu S, Alsancak Y, et al. Short and long term complications of device closure of atrial septal defect and patent foramen ovale: meta-analysis of 28,142 patients from 203 studies. Catheter Cardiovasc Interv, 82: 1123-1138, 2013.
- 12. Masutani S, Senzaki H. Left ventricular function in adult patients with atrial septal defect: implication for development of heart failure after transcatheter closure. J Card Fail, 17: 957-963, 2011.
- 13. Mendirichaga R, Smairat RA, Sancassani R. Late tissue erosion after transcatheter closure of an atrial septal defect. Catheter Cardiovasc Interv, 89: 502-504, 2017.
- 14. Kalayci B, Kalayci S. Right atrial ball thrombus associated with atrial septal occluder device: A late complication of transcatheter atrial septal defect closure. Anatol J Cardiol, 18: E9, 2017.