Humanistic planning for urban older adults
Investigation and Analysis on Travel and Health of the Elderly in the Old Residential Areas in Beijing

2023 Volume 11 Issue 1 Pages 85-103
Details
2023 Volume 11 Issue 1 Pages 85-103
In the context of aging, community has become the main activity place for the elderly, and their daily travel is closely related to their health. This paper aims to understand the overall travel and activity characteristics, health level of the elderly with different attributes in the old residential areas, the relationship between travel conditions and health level, the difficulties faced by daily travel and suggestions to improve the travel environment and health level of the elderly. Three old residential areas in Chaoyang District, Beijing were selected to investigate 15 elderly people on their daily travel, activities and health in the form of observation, questionnaire and interview. The survey results show that the daily travel modes of the elderly mainly include walking, cycling and public transportation. About 1 / 3 of the elderly need auxiliary tools. About 80% of the elderly suffer from diseases and 20% of the elderly have normal body mass index(BMI). The self-rated mental health (MSH) of the elderly is the best. The relationship between the average activity duration of the elderly and their health level under different travel conditions is mainly shown as follows: with the increase of travel time per trip, the outdoor activity duration of the elderly shows a trend of "first increase and then decrease", the number of diseases decreases, and the average BMI fluctuate. The next step is to expand the research scope and explore the travel and health status of the elderly in different community types, so as to provide basis for improving the travel environment and the health of the elderly.
Population aging has become an irreversible worldwide trend in the 21st century, and the "aging" characteristics of China's elderly population are obvious. According to the standards of the World Health Organization (WHO), the population aged 65 and over accounts for 7% of the total population, which can be regarded as an aging society. China entered an aging society as early as 2000. At present, China is in a period of rapid aging (1999-2022). The speed of population aging is accelerating, showing a development trend of "fast speed, large scale, high peak value and aging"(Wang, 2015; Yang, Zhang, & Chen, 2020). According to the seventh national census, China's elderly population over the age of 60 exceeds 264 million, accounting for 18.70% of the total population (among which, the population aged 65 and over is 190.64 million, accounting for 13.50%), which means that China is very close to the "moderately aging" Society (Figure 1).
As of the end of 2020, the total household population of registered residence in Beijing was 14 million and 8 thousand, of whom 3 million and 786 thousand were elderly people aged 60 and above, accounting for 27% of the total population (Office of Beijing Committee of Aging, 2021). Beijing is facing the impact of population aging.
In addition, in 2000, China's overall life expectancy was 72 years, and the healthy life expectancy was 65 years; In 2019, the average life expectancy was 77.4 years (74.7 years for men and 80.5 years for women), and the healthy life expectancy was 68.5 years (67.2 years for men and 70.0 years for women), which means that residents have been living with diseases for more than 8 years; More than 180 million elderly people suffer from chronic diseases (accounting for 75%). This means that the elderly in China have a high proportion of diseases, early and long illness time. The proportion of urban and rural residents in China who often participate in physical exercise is 33.9%. Almost half of the elderly never exercises and their sleep quality is not high. Only about 30% of the elderly are in good health (Dang, Wei, & Liu, 2018). Lack of exercise has been described as the biggest public health problem in the 21st century.

Note: The abscissa is the year, the ordinate is the unit of hundred, and the data of 2030, 2040 and 2050 are the prediction data (Du & Li, 2021).
With the increase of the age of the elderly, the audio-visual ability decreases day by day, the physical health becomes worse, the life-space of the elderly gradually shrinks, and the community has become the main place for the daily activities of the elderly. The old residential area is a community with a relatively concentrated aging population, inhabited by a large number of elderly people. These communities have been built for a long time, and various facilities are not complete enough. The elderly also is facing various obstacles in their daily travel. “Age in Place” is the will of most elderly people. The elderly generally has a strong sense of belonging to the place where they live for a long time (Gu & Chai, 2015). Since 2011, Beijing, Shanghai and other cities have successively proposed the "9073" or "9064" elderly care service pattern, that is, it is planned that 90% of the elderly will adopt local elderly care (i.e. home-based or community-based elderly care). Old residential areas often lack the consideration of suitability for the elderly, and home-based elderly care puts forward special requirements for residential environment, supporting facilities and travel conditions (Yao & Qin, 2021). The aging transformation of old residential areas is the necessity of development.
At present, most of the elderly over the age of 60 have retired, and daily activities have become an important part of their life. A large number of studies show that (Gu Wang, & He, 2012; Wang, Liao, &Guo, 2018), active participation in daily activities can help the elderly maintain good physical function and mental state, slow down the decline of cognitive ability, and effectively prevent the occurrence of some elderly diseases. Activity derived travel, for the elderly, travel itself is also an activity. Pay attention to the daily travel of the elderly in the old residential areas, grasp the characteristics and regular pattern, understand the daily life needs of the elderly, and create a community travel environment more in line with the actual needs for the elderly, so as to make it convenient and willing to travel, so that the elderly has a good health.
This paper selected the elderly in three old residential areas in Chaoyang District, Beijing as the research object. Through observation, questionnaire and interview, this paper analysed the overall travel and activity characteristics of the elderly in the old residential areas, the health level of the elderly with different attributes, the relationship between travel conditions and health, the difficulties faced by daily travel, and obtains some preliminary conclusions and countermeasures. Combined with the policies of old community reconstruction and healthy aging in Beijing, it is hoped that these conclusions and countermeasures will be helpful to improve the travel conditions of the elderly and increase the travel opportunities of the elderly, so as to maintain and improve the health level of the elderly and improve the quality of life of the elderly.
With the intensification of population aging all over the world, the concepts of "active aging", "healthy aging" and "aging in place" have been put forward. Scholars at home and abroad have carried out a large number of relevant research on the topics of elderly travel behaviour (characteristics and influencing factors), health status, aging in old communities (spatial behaviour of elderly people in communities, the relationship between community environment and health), and the relationship between travel and health.
Foreign research on the travel of the elderly mainly focuses on mobility and accessibility, which is mainly reflected in four aspects, including 1) describing and compare the travel characteristics of the elderly between different countries or regions, and discuss, summarize and analysing the travel characteristics and their influencing factors (Rosenbloom, 2001); 2) studying the change trend of the travel characteristics of the elderly in corresponding countries through the survey data, and study and analysing the urban traffic development and its contradictions; 3) quantitatively analysing the travel characteristics (travel times, travel time, travel distance, and so on.) of people over 65 years old and people aged 19-64 years old, and put forward relevant measures and suggestions to improve the travel of the elderly (Collia, Sharp, & Giesbrecht, 2003); 4) studying and analysing the travel characteristics and influencing factors of the elderly, such as family composition, income, travel tools and other factors. There are only a few studies on the travel behaviour characteristics of the elderly in China. Domestic scholars have mainly carried out research on the travel situation of the elderly in combination with the actual situation in China from two aspects, including 1) analysing the travel characteristics and influencing factors of the elderly (Li, 2014; Qi, 2018; Song & Wang, 2018; J. Wang et al., 2018; Xia, 2015; Xia & Guan, 2013; Zhang et al., 2007); 2) analysing the spatial characteristics of travel behaviour of the elderly (Ma & Xie, 2020; Xu et al., 2019). Domestic urban elderly behaviour research mainly focuses on shopping, leisure, medical treatment, physical exercise and other activities of the elderly, while less attention is paid to the travel process when participating in activities (Gu & Chai, 2015).
The physical and mental health of the elderly has attracted more and more attention from the Chinese government and academia. Since 2017, the outline of "healthy Beijing 2030" plan, healthy China action (2019-2030) and healthy Beijing action (2020-2030) have been released successively. The WHO believes that self-rated health is an important indicator of the health and health expectancy of the population. The future health status, quality of life, incidence rate and mortality of individuals are related to the self-rated health related (Meng & D Arcy, 2015). Many scholars have made empirical analysis on the health status of elderly groups with different characteristics. From the existing research, using logistic regression method to explore the factors affecting the health status of the elderly can be roughly divided into five categories, including natural attributes, socio-economic status, lifestyle, sickness status, psychological factors and so on (Jiang et al., 2015). Many scholars have also carried out research on the impact of exercise intervention on the physical and mental health of the elderly (Li, 2010; Li & Zhou, 2015).
Domestic scholars in urban and rural planning, architecture, gerontology and other disciplines have carried out research on the aging suitability renewal of old communities from the perspectives of community built environment, community renewal planning and community space governance (Yao & Qin, 2021). The research topics are mainly based on the research on the spatial behaviour characteristics of the elderly, suggestions on the improvement of the living environment and facility allocation of the old community, the social participation of the elderly in the transformation, the relationship between the community built environment and the health of the elderly (mainly including the factors of the community built environment affecting the health of the elderly (Liu & Yang, 2016; Song et al., 2018) and the action mechanism of the community built environment on the health of the elderly (Bowling & Stafford, 2007; Guo et al., 2021; Wu et al., 2019), the demand characteristics and travel capacity of community facilities for the elderly optimize the planning and location of public service facilities (Hu et al., 2016; Li et al., 2017; Xu et al., 2011), and so on. The attention to the mental health and social health of the elderly has not been really introduced into the aging renewal planning of the old community. The travel demand of the elderly with different economic conditions, age groups and health levels in different old communities are also different, which further research is necessary.
People pay more and more attention to the contribution of travel to the level of physical activity (Dong et al., 2015; Song & Wang, 2018), as well as the impact on obesity (Fox & Hillsdon, 2007; Smith et al., 2008)and related health status (Crotti et al., 2021; Ferdman, 2021; Kroesen & De Vos, 2020; Pae & Akar, 2020). Studies showed that the health status of the elderly is closely related to their travel. Travel conditions and travel opportunities are mostly reflected by the built environment. The improvement of the built environment related to travel can effectively improve the health status of the elderly group (Huang et al., 2020). Bert van wee et al. Comprehensively described the relationship between travel behaviour and health outcomes from the perspective of conceptual model. The impact of travel behaviour on health can be positive or negative, and varies depending on travel mode and environment (van Wee & Ettema, 2016). In 2003, Rauh pointed out in his research that the impact of built environment on human health can be conceptualized into three travel related fields: land use mode, urban design characteristics and transportation system (Rauh, 2003). The transportation system determines the convenience of individual travel to the destination; the land use pattern reflects the distribution position and compactness of different functional spaces in the city, and determines the difficulty of individual to destination; urban design features such as the number of carriageways and calming facilities will affect the safety and attractiveness of streets, and ultimately affect individual travel modes. This paper reflected the travel conditions of the elderly by using factors such as whether there is an elevator in the residential area, whether auxiliary tools are needed for travel, main travel modes, time from home to destination and so on.
The travel behaviour of the elderly is generally concerned by urban planning, geography, sociology, economics, medicine and other disciplines. Research on health is mainly carried out in sports, medicine and other fields. At present, the research on the travel and health of urban elderly in the field of transportation is generally insufficient. The research scope is mainly concentrated in Beijing, Shanghai and other cities, and the research is carried out at the micro scale of community. This paper focused on the daily travel and health of the elderly in the old residential areas. The research was carried out in the form of observation, questionnaire and interview. The method adopted is more conducive to in-depth understanding of the daily travel conditions and health level of the elderly.
The elderly population refers to the population above the age limit of the elderly. The elderly population refers to the population above the age limit of the elderly. Different cultural circles have different definitions for the elderly. The World Health Organization defines the elderly as people over the age of 60, while some western developed countries believe that 65 is the dividing point. China stipulates that the starting age standard of the elderly is 60 years old. In addition, considering that residents under the age of 60 who retire early also enter the elderly life, they were also included in the scope of this study.
The old residential areaThe definition of old residential areas refers to the residential areas in the city and county (Chengguan Town) built before 2000, with backward public facilities affecting the basic life of residents and strong residents' willingness to transform. Shanty towns (residential houses) that have been included in the urban shed reconstruction plan and are to be reconstructed by demolition and new construction (reconstruction, expansion, renovation), as well as areas and villages in the city where residents mainly build their own houses, do not belong to the category of old residential areas.
The old residential areas mentioned in this paper refers to the residential community built earlier (before 2000), with low construction standards, lack of elevators for going upstairs and downstairs, aging infrastructure, imperfect supporting facilities and lack of perfect management mechanism.
HealthIn 1989, WHO redefined health as "health is not only free of disease or weakness, but also includes physical health, mental health, good social adaptation and moral health". According to the existing research, the measurement indicators of the health status of the elderly in China's academic circles are mainly divided into subjective indicators and objective indicators. The commonly used objective indicators mainly include chronic disease, loss of working time due to illness, daily activity ability, physical indicators, and so on. The commonly used subjective indicator is self-rated health. Self-rated health status refers to the individual's cognition and expectation of their own real health status, which is closely related to physical, mental health and social adaptability.
In this paper, the self-rated health measurement scale (SRHMS) was used for the subjective evaluation of physical health, mental health, social health and overall health, and the number of diseases and body mass index (BMI) were used for the objective evaluation of physical health. BMI is a standard commonly used in the world to measure the degree of body weight and health (Table 1). BMI calculation formula is:
Where, H stands for height in meter; W stands for body weight in kilograms.
Table 1. BMI reference standard (Dong et al., 2001)
| light | normal | overweight | obesity | |
|---|---|---|---|---|
| WHO | <18.5 | 18.5~24.9 | 25.0~29.9 | ≥30 |
| China | <18.5 | 18.5~23.9 | 24.0~27.9 | ≥28 |
SRHMS covers 48 items of self-rated physical health subscale, self-rated mental health subscale, self-rated social health subscale and one overall health self-rated item. The score range of each item is 0-10 points. Except that items 4, 5, 7, 24, 25, 26, 27, 28, 29 and 30 are reverse scoring questions, the higher the score of other items, the better the health status.
The theoretical maximum scores of self-rated physical health (PSH), self-rated mental health (MSH), self-rated social health (SSH) and self-rated health (SH) were respectively 170, 150, 120 and 440; The theoretical minimum value is 0. In order to facilitate understanding, the score of the scale was transformed into a percentage system (Gao et al., 2021).
Where,
The normal distribution method was adopted in this demarcation norm, and the score of self-rated scale
From the perspective of micro individuals, this paper explored the travel behaviour and travel conditions of different elderly individuals in the old residential areas through observation, questionnaire and interview. Using the method of statistical analysis, this paper attempted to analyse the travel and health of the elderly, understand the overall travel and activity characteristics of the elderly in the community, the health level of the elderly with different attributes, the relationship between the travel conditions and health of the elderly, and the difficulties faced by daily travel.
We first learned about the daily travel activities of the elderly in the three old residential areas with high aging rate in Chaoyang District of Beijing through observation and interview. Then from each area (7 people in community A, 8 people in community B, 4 people in community B1, 4 people in community B2), according to age, gender, living conditions, whether there is an elevator, scope of activities (inside and outside the community), a total of 15 representative respondents were selected to participate in this study. The survey mainly focused on the socio-economic attributes of the elderly (including gender, age, income, occupation, education level, marital status, and so on.), living conditions (housing type, family members, living time, whether there is an elevator, and so on.), travel and activity (including travel mode, travel purpose, frequency, type, place and time of physical activities), health status (BMI, number of diseases, living habits, self-rated health), difficulties in daily travel and improvement suggestions (Appendix A). The survey was conducted from September to November, 2021.
The proportion of male and female respondents was relatively balanced, with men accounting for 47%. The age was mainly distributed in 60-75 years old, accounting for 80%. The education level was mainly primary school and junior middle school, accounting for 66.7%. About half of the elderly have a personal monthly income of 3000 ~ 5000 yuan. 80% of elderly couples live alone. 80% of the elderly live in the community for more than 10 years and 50% for more than 20 years (Figure 2 – Figure 3). The elderly like to live in the family and community of their choice as long as possible, and maintain a certain degree of independence and quality of life. Among the elderly respondents who did not install elevators in residential units, about 40% said they had difficulties in getting up and down stairs (at least one floor).
Travel and activity characteristics of the elderlyThe main travel mode for the elderly has walking, bicycle, bus and others. About 1/3 of the elderly need auxiliary tools, such as walking stick (20%) and wheelchair (13.3%). The longest acceptable walking distance for the elderly was 60% within 2 km and 80% within 3 km; The maximum acceptable walking speed of the elderly was less than 2 km/h in 1/3 and less than 4 km/h in 2/3 (Figure 4). The walking distance and activity duration are affected by age. The acceptable walking distance per trip of the elderly gradually decreases with age.


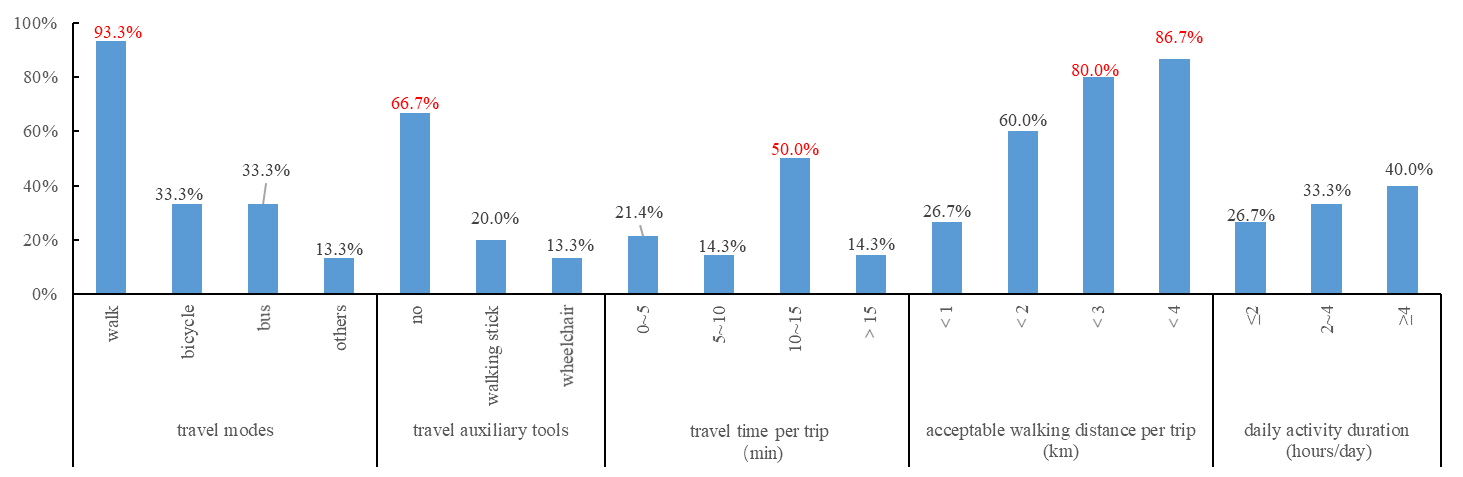
The activity places for the elderly were mainly distributed in the community, and 20% of the life-space of the elderly was restricted to the neighbourhood area. The travel time was mainly 10-15 minutes, and the outdoor activity duration of the elderly mainly concentrated at 8-11 a.m. and 2-5 p.m. Their daily physical activities mainly include housework and leisure activities. The leisure activities that the interviewed elderly were keen on include running, walking, tennis, table tennis, cycling, Tai Chi, Baduanjin, chess, dancing, singing, waist drum, long gun and arrow practice. The average daily outdoor activity duration of the elderly in different age groups was more than 3 hours (Table 2). The most popular individual sports among Shenzhen residents were running and walking, followed by cycling, gymnastics, Tai Chi, qigong, yoga and Baduanjin (Wu et al., 2018). The older adults in Harbin, China had an average activity duration of 1272 min/week, indicating that older adults were willing to carry out a high level of leisure-time physical activity despite the cold climate (Yuan et al., 2022).
In addition, the most important thing for the elderly in their daily travel is safety, and they are very afraid of falling. The main factors that adversely affect the daily travel of the elderly have the smoothness of the road (occupied sidewalks, mixed traffic of people and vehicles), pedestrian crossing facilities (the spacing of road intersections is too large, and it is difficult to pass through a green light time. It is difficult for pedestrian overpasses or underpasses to cross the street), leisure facilities (the distribution of pedestrian rest facilities and fitness facilities was unreasonable), and so on.
| Age | Average walking distance per trip interval (km) |
Average daily activity duration (hours) |
|---|---|---|
| <70 | [2.76 , 3.43] | 3.38 |
| 70~79 | [1.69 , 2.14] | 3.14 |
| ≥80 | [0.00 , 0.20] | 3.75 |
Among the respondents, about 80% of the elderly suffered from one or more diseases. About 20% of the elderly reached the standard BMI value, and about 70% of the elderly were overweight (BMI ≥24.0). More than half of the elderly said their sleep quality was not high (Figure 5). According to WHO estimates, almost half of China's elderly never exercise and sleep quality is not high (Dang et al., 2018).

The scores of PSH, MSH, SSH and SH of the elderly in the old community as a whole and by gender were calculated according to the percentage system, as shown in Table 3 below.
| PSH | MSH | SSH | SH | ||
|---|---|---|---|---|---|
| Total | 67.41±17.01 | 78.44±10.63 | 66.89±10.92 | 71.03±8.38 | |
| gender | Male | 68.82±15.72 | 83.05±4.54 | 72.26±7.45 | 74.61±7.01 |
| Female | 70.84±14.85 | 73.43±13.70 | 64.17±11.09 | 69.90±7.02 | |
The scores of SH, PSH, MSH and SSH of the elderly in the old residential areas were (71.03 ± 8.38), (67.41 ± 17.01), (78.44 ± 10.63), (66.89 ± 10.92). Among the four self-rated health of the elderly, the total score of MSH was the best; the total scores of MSH, SSH and SH in men were higher than those in women, and the total score of PSH in women was higher than that in men.
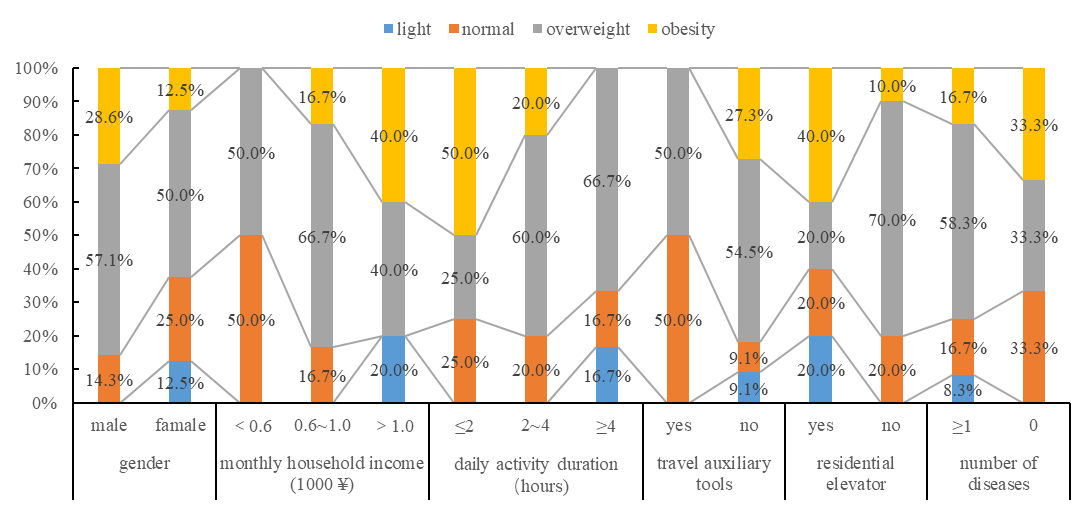
Health of the elderly under different attributes Based on BMI valueWomen with normal BMI accounted for 25.0%, higher than men (14.3%), and obesity was just the opposite. More than half of men and women were overweight. The proportion of normal decreased and obesity increased with the increase of monthly household income. The obesity rate of the elderly with elevators in the residential area (40%) was much higher than that without elevators (10%), but the proportion of overweight elderly without elevators was also very high (70%). The proportion of overweight and obesity was higher in the elderly who do not need auxiliary tools. With the increase of activity duration, the overweight of the elderly showed an upward trend, and the normal and obesity showed a downward trend. For the BMI of the elderly with one or more diseases, normal and overweight accounted for 16.7% and 58.3% (Figure 6).
In order to simplify the analysis, the number of diseases of the elderly is divided into two categories: 0 and ≥ 1. Female and the elderly who have lived for more than 20 years have a higher proportion of suffering from one or more diseases. For the elderly whose main daily travel mode was walking, cycling, bus and others, the prevalence rate showed a downward trend; The proportion of the elderly with disease was directly proportional to activity duration, that is, the elderly with disease had longer activity duration which was 2.22 hours per day, 0.89h more than the elderly without disease (Figure 7).

The female elderly was healthier than the male, and the proportion of PSH and SH "Poor" of the male elderly was higher than that of the female; The proportion of PSH, MSH, SSH and SH "Good" in female elderly was higher than that in male. The elderly without elevators in residential areas were healthier than those with elevators. The "Poor" ratio of PSH and SH of the elderly without elevators in residential areas was higher than that of the elderly with elevators; The proportion of PSH, MSH, SSH and SH "Good" of the elderly without elevator in the residential area was higher. With the extension of the activity duration of the elderly, the proportion of MSH, SSH and SH "Good" of the elderly increased, and the proportion of SSH "Poor" of the elderly decreased. (Figure 8 - Figure 10).



Figure 11 shows that the elderly without elevators spend 0.4h longer outdoors, have 0.4 fewer diseases and have a lower mean BMI than the elderly with elevators. The elderly without elevators (especially those living on the third floor or above) spend more outdoor-activity duration and have better self-rated health, which may be related to their fewer trips downstairs (less than 1-2 times a day) but more activities (such as walking-shopping-going home) and longer time (such as 1-2 hours or even longer) downstairs each time. The elderly who need assistive tools have 0.39 more kinds of diseases, 0.25h more time outdoors and lower mean BMI than the elderly who do not need assistive tools.

The elderly who mainly walk and ride bicycles have higher morbidity and longer outdoor activities; The elderly who travel by bus or other means have fewer diseases, shorter outdoor activities, and higher mean BMI; Among the elderly with different travel modes, the average BMI of the elderly with the main travel mode of walking behaviour is the lowest; The average BMI of the elderly under different travel conditions is more than 24, and they are overweight.
The duration of outdoor activities of the elderly increased first and then decreased with the increase of travel time. The number of diseases of the elderly was inversely proportional to the travel time. The closer the activity place and the shorter the travel time of the elderly, the more kinds of diseases they had; That is, the older people who suffered from more than one disease, the closer their activity place was to their home.
Through the investigation and analysis of the daily travel and health status of the elderly in the old residential areas, this paper studied the overall travel and activity characteristics of the elderly, the health of the elderly with different attributes, the relationship between travel conditions and health, and the difficulties faced by daily travel. On this basis, this paper tried to put forward some suggestions for the improvement of travel and health of the elderly in the old residential areas.
(1) Daily travel and health of the elderly in the old residential areas
The daily travel modes of the elderly in the old residential areas mainly included walking, bicycle, bus, and so on. about 1 / 3 of the elderly need auxiliary tools for travel, and the activity duration of a day was mostly within 4 hours. The daily activities of the elderly are mainly in the community, and 20% of the elderly have restricted life-space. About 80% of the elderly suffered from diseases, and about 20% of the elderly had normal BMI. The self-rated mental health (MSH) of the elderly was the best.
There are obvious differences in BMI of the elderly under different gender, family income, activity duration, whether there is an elevator in the residential area, and whether auxiliary tools are needed; There are significant differences in the number of diseases among the elderly under different gender, living time, travel mode and activity duration; The self-rated health (PSH, MSH, SSH, SH) of the elderly shows significant differences under different gender, activity duration, whether there is an elevator in the residential area, and whether auxiliary tools are needed.
The travel conditions of the elderly are reflected by factors such as whether there is an elevator in the residential area, whether auxiliary tools are needed for travel, main travel modes, and single travel time. The relationship between the average activity duration of the elderly and their health level under different travel conditions is mainly shown as follows: with the increase of travel time per trip, the outdoor activity duration of the elderly shows a trend of "first increase and then decrease", the number of diseases decreases, and the average BMI fluctuates. The elderly without elevators spend 0.4h longer outdoors, have 0.4 fewer kinds of diseases and have a lower mean BMI than the elderly with elevators. The elderly who need assistive tools have 0.39 more kinds of diseases, 0.25h more time outdoors and lower mean BMI than the elderly who do not need assistive tools.
(2) Suggestions on improving the travel environment and health level of the elderly in old residential areas
In the context of aging society, how to reasonably meet the travel needs of the elderly, improve the travel conditions of the elderly, increase the travel opportunities of the elderly, and make the elderly "comfortable, convenient and willing to travel", maintain health and happiness is a problem worthy of consideration and to be solved.
The most important thing for the elderly in their daily travel is safety, and they are very afraid of falling. Walking and cycling are the main travel modes of the elderly. In order to ensure the safety of walking and cycling of the elderly, it is necessary to consider the fatigue of walking for a long time and the acceptable walking distance of the elderly, and reasonably add pedestrian rest facilities; There is an urgent need to solve the problems of occupied sidewalks, unclear traffic signs and lack of bicycle lanes. The elderly with or without elevators in the residential area showed reverse differences in activity duration, BMI value and number of diseases. The installation of elevators in the old residential areas can provide more travel opportunities for the elderly with "poor” health. It is suggested that the elderly who have no difficulty in getting up and down stairs could reduce taking elevators, which is more beneficial to their own health. For this, the stair handrails in the old residential areas are indispensable.
In addition, the elderly mainly carries out housework and leisure activities in their daily life. When the distribution of community leisure facilities is insufficient or the availability is low, the distance between from home and the community fitness place exceeds the acceptable walking (riding) distance of the elderly, and the elderly feel unsafe during travel, the opportunities for travel of the elderly will be reduced. In the long run, it will have an adverse impact on the physical and mental health of the elderly. With the increase of travel time from home to the activity destination, the outdoor activity time of the elderly presented the trend of "increasing first and then decreasing". The activity places and facilities for the elderly can be arranged in layers and reasonably planned within the walking range of 5, 10 and 15 minutes from home. The establishment and addition of community canteens for the elderly (meal aid for the elderly and dining table for the elderly) will better meet the dining service needs of the elderly in the old residential areas.
The sample of this study is limited. In the next stage, the research needs to expand the research scope and conduct supplementary investigation to understand the travel and health status of the elderly in different types of communities, so as to provide a more sufficient basis for exploring the relationship between the two, improving the travel environment of the old residential areas and the health level of the elderly. In addition, the relationship between health and travel of the elderly is a phenomenon that needs long-term observation, and more survey data of different time sections are needed.
Conceptualization, W.L. and H.G.; methodology, W.L., H.G.; software, W.L.; investigation, W.L.; resources, H.G.; data curation, W.L.; writing—original draft preparation, W.L.; writing—review and editing, H.G. and W.L.; supervision, H.G. All authors have read and agreed to the published version of the manuscript.
The authors declare that they have no conflicts of interest regarding the publication of the paper.
This research was funded by the National Natural Science Foundation of China (Grant No.71971005) and the Natural Science Foundation of Beijing, China (Grant No. 8202003)
1.Gender:_______;Age:______;Height:_____(m);Weight:______(kg)
2. Are you retired now?
3. What was your occupation before retirement? What is your education level?
4. Who do you live with now? What is your residential type?
5. Your monthly personal and familial income are _____ and _____
6. How long do you stay in this community_____________ years?
7. What floor do you live on? What are the highest floors?
8. Is there an elevator in your residential unit?
9. What are your daily means of transportation?
10. What is your main purpose of daily travel?
11. How many times do you go out in a day? What time do you go out? Where are you going? What activities do you participate in? How long?
12. How long does it take to walk from home to the destination and how far is it?
13. How long do you spend outdoors every day?
14. What factors encourage or restrict your travel? What factors make you dissatisfied with the travel, activities and other environment in the community? What do you think needs to be improved most?
Table A-2 Self-rated health assessment scale1.How are your eyesight?
2.How is your listening?
3.How's your appetite?
4.Do you often feel unwell in your intestines and stomach (such as abdominal distension, diarrhea, constipation, etc.)?
5.Do you feel tired easily?
6.How was your sleep?
7.Do you have different degrees of pain in your body?
8.Are you having trouble dressing yourself?
9.Do you have any difficulty combing by yourself?
10.Do you have any difficulty in undertaking daily housework?
11.Can you go shopping alone?
12.Are you having trouble eating by yourself?
13.Do you have any difficulty bending down and knees?
14.Do you have any difficulty getting up and down the stairs (at least one floor)?
15.Do you have any difficulty walking half a mile?
16.Do you have any difficulty walking three miles?
17.Do you have difficulty in participating in activities with high energy? consumption?
18.What do you think of your physical health as a whole compared with your peers?
19.Are you optimistic about the future?
20.Are you satisfied with your current living conditions?
21.Do you have confidence in yourself?
22.Do you feel safe in your daily living environment?
23.Do you feel happy?
24.Do you feel nervous?
25.Do you feel bad and depressed?
26.Are you afraid for no reason?
27.Do you feel at ease after repeatedly confirming what you have done?
28.Do you feel lonely when you are with others?
29.Do you feel restless and restless?
30.Do you feel empty, bored or meaningless to live?
31.How is your memory?
32.Is it easy for you to concentrate on one thing?
33.How about your ability to think or deal with problems?
34.Overall, what do you think of your mental health
35.Can you handle the unpleasant things that happen to you in your life, study and work properly
36.Can you quickly adapt to the new living, learning and working environment
37.How do you evaluate your role in work, study and life?
38.Is your family life harmonious?
39.Do you have many close colleagues, classmates, neighbours, relatives or partners?
40.Do you have any friends who can share happiness and sadness with you
41.Do you talk about problems with your friends or relatives?
42.Do you often keep in touch with your relatives and friends (such as visiting each other, telephone greetings, correspondence, etc.)?
43.Do you often participate in some social and collective activities (such as party and League, trade union, student union, religion, friend gathering, sports competition, entertainment, etc.)?
44.Can you rely on your family to a large extent when you need help?
45.Can you rely on your friends to a large extent when you need help?
46.When you encounter difficulties, do you take the initiative to seek help from others?
47.Compared with your peers, what do you think of your social functions? (such as interpersonal relationship, social communication, etc.) on the whole
48.Compared with your peers, what do you think of your health status in genera?

| Very Poor | Poor | General | Good | Very Good | ||
|---|---|---|---|---|---|---|
| PSH | Male | [0,53.11) | [53.11,60.96) | [60.96,76.68) | [76.68,84.54) | [84.54,100] |
| Female | [0,55.99) | [55.99,63.42) | [63.42,78.27) | [78.27,85.69) | [85.69,100] | |
| Total | [0,50.40) | [50.40,58.91) | [58.91,75.91) | [75.91,84.42) | [84.42,100] | |
| MSH | Male | [0,78.51) | [78.51,80.78) | [80.78,85.31) | [85.31,87.58) | [87.58,100] |
| Female | [0,59.72) | [59.72,66.58) | [66.58,80.28) | [80.28,87.13) | [87.13,100] | |
| Total | [0,67.81) | [67.81,73.13) | [73.13,83.76) | [83.76,89.08) | [89.08,100] | |
| SSH | Male | [0,64.81) | [64.81,68.54) | [68.54,75.98] | [75.98,79.71) | [79.71,100] |
| Female | [0,53.08) | [53.08,58.63) | [58.63,69.71] | [69.71,75.26) | [75.26,100] | |
| Total | [0,55.97) | [55.97,61.43) | [61.43,72.35] | [72.35,77.81) | [77.81,100] | |
| SH | Male | [0,67.60) | [67.60,71.11) | [71.11,78.11] | [78.11,81.62) | [81.62,100] |
| Female | [0,62.88) | [62.88,66.39) | [66.39,73.41] | [73.41,76.91) | [76.91,100] | |
| Total | [0,62.65) | [62.65,66.84) | [66.84,75.22] | [75.22,79.41) | [79.41,100] |
Note: For example, a woman, 72 years old, converts her scale score into a percentage system, with a physical health score of 73.14, a mental health score of 84.05, a social health score of 54.30 and an overall score of 61.28. With reference to the demarcation norm, it can be concluded that PSH, MSH, SSH and SH of the elderly are general, good, poor and very poor.