Editorial
Is Oxidative Stress a Key Player for Progression of Cardiovascular Disease in Dialysis Patients?
2021 年 28 巻 3 号 p. 227-229

詳細
2021 年 28 巻 3 号 p. 227-229
See article vol. 28: 249-260
It is generally recognizing that a major cause of death is cardiovascular disease (CVD) in patients undergoing dialysis. Japanese data from January to December 2018 showed that the percentage of death due to CVD among all causes of death was 33.1%, with congestive heart failure, stroke, and myocardial infarction being 23.5%, 6.0%, and 3.6%, respectively 1) . Previous studies reported that most patients with end stage kidney disease already had vascular and valvular calcification and significant coronary artery disease prior to dialysis initiation 2) . The data from the United States also showed that the most frequent CVDs among dialysis patients were congestive heart failure, coronary artery disease, and peripheral artery disease 3) . From these findings, the presence of CVD in dialysis patients must always be checked.
CVD is much more frequent in dialysis patients than in the general population because chronic kidney disease (CKD) patients, particularly dialysis patients, have not only many classical risk factors but also non-classical risk factors for CVD. Among the non-classical risk factors, oxidative stress is one of the most important. The activation of the renin-angiotensin-aldosterone system and sympathetic nerve system, chronic kidney disease-mineral bone disorder, uremic toxins, hypertension, anemia, malnutrition, diabetes mellitus, etc. increase oxidative stress ( Fig. 1) . Most dialysis patients have these conditions and therefore increased oxidative stress. Sasaki et al. analyzed a cohort data of 517 hemodialysis patients and examined the relationship of an oxidative stress marker, derivatives of reactive oxygen metabolites (d-ROMs), with CVD events and all-cause mortality in 5 years 4) , showing that d-ROMs were significantly correlated with all-cause mortality but not CVD events. However, a significant association was not observed between d-ROMs and all-cause mortality after adjustment by several confounders including an inflammatory marker, C-reactive protein. Oxidative stress and inflammation are closely linked with each other, both greatly contributing to the CVD progression. Moreover, in the study, no significant difference was observed in the d-ROM levels between CVD and non-CVD patients. Although these findings may reflect that dialysis patients have various crucial risk factors for CVD other than oxidative stress, it is possible that a way to evaluate the state of oxidative stress might influence the results of the study. Previous studies of CKD patients including dialysis patients reported that other oxidative stress markers such as advanced glycation end products, myeloperoxidase, oxidized albumin, 8-hydroxy-2’-deoxyguanosine, etc. were related to CVD events and/or all-cause mortality 5) . Possibly, if the study was performed using other oxidative stress markers, one might get different results.
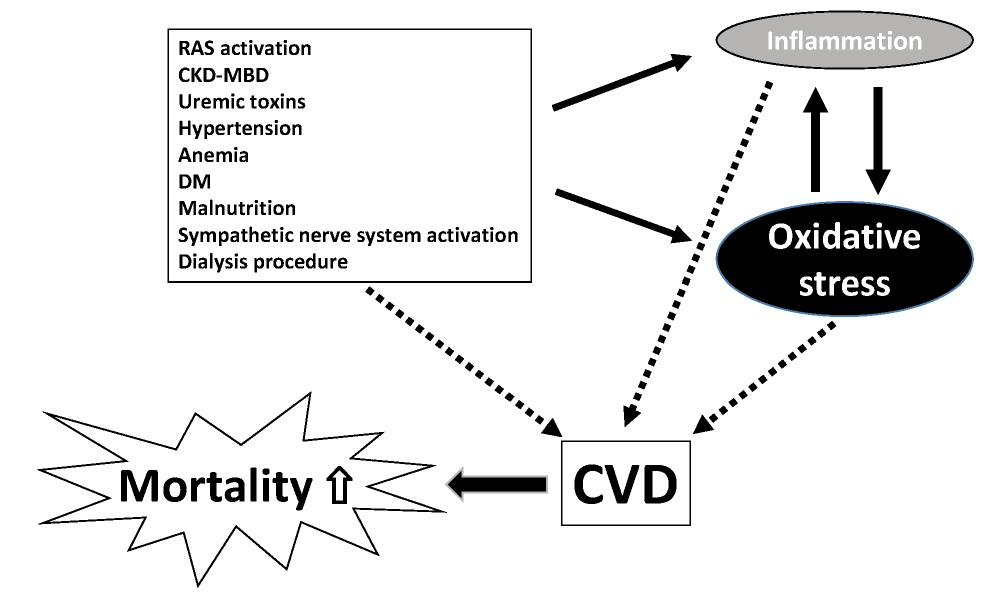
CVD, cardiovascular disease; RAS, renin-angiotensin-aldosterone system; CKD-MBD, chronic kidney disease-mineral bone disorder; DM, diabetes mellitus
The experimental studies demonstrated that the suppression of oxidative stress promptly attenuates CKD and CVD progression 6, 7) . To date, a number of clinical studies aimed at preventing CKD and CVD progression by antioxidative agents had also been performed. The studies, which are fresh in our memory, are two randomized controlled trials using bardoxolone methyl, a Nrf2-inducing agent. Surprisingly, one of them, the BEAM trial, demonstrated that the treatment with bardoxolone methyl improved kidney function as measured by an increase of the estimated glomerular filtration rate in type 2 diabetic patients with CKD 8) . Another study, the BEACON trial, unfortunately, did not demonstrate its effectiveness because of safety concerns, due to an increase in CVD cases 9) . Taking the problem into account, the further study, the TSUBAKI trial, was performed in Japan, which demonstrated that bardoxolone methyl could ameliorate the kidney function of type 2 diabetic patients with CKD similar to the result of the BEAM trial 10) . Now, a phase Ⅲ trial, the AYAME trial, including approximately 700 type 2 diabetic patients with CKD, is ongoing in Japan. Proving the effect of bardoxolone methyl on not only CKD but also CVD is expected in the near future.
In contrast, whether suppression of oxidative stress has a favorable impact on CVD in dialysis patients remains unclear. Until now, although several clinical studies using antioxidative agents such as vitamin C, vitamin E, coenzyme Q, L-carnitine, tempol, and N-acetylcystein were performed for dialysis patients, the number of study participants was relatively small. In addition, some of them reported that antioxidative agents could decrease oxidative stress but could not prove that they could reduce CVD events. As mentioned above, since dialysis patients have many risk factors for CVD, controlling only one risk factor cannot reduce CVD events. The control of oxidative stress alone is not enough to prevent CVD events in dialysis patients, and various risk factors, including anemia, CKD-MBD, hypertension, dyslipidemia, and diabetes mellitus, should be controlled appropriately. Oxidative stress is not the sole key player for CVD progression in dialysis patients. It should be kept in mind that there are various key players for CVD progression in these patients.
Hideki Fujii has received a speaking fee and a donation for research from Kyowa Kirin Co., Ltd.