Editorial
What is the Role of Cholesterol Absorption and Synthesis Biomarkers in Humans?
2023 年 30 巻 10 号 p. 1307-1308

詳細
2023 年 30 巻 10 号 p. 1307-1308
See article vol. 30: 1336-1349
In our daily clinic, we measure serum cholesterol to assess the risk for atherosclerosis1). However, we do not care much about the cholesterol homeostasis (its balance between absorption and synthesis) in humans. It has been shown that cholesterol homeostasis is strictly regulated by absorption from the intestine and its synthesis in the liver. Generally, approximately 70% of serum cholesterol is derived from synthesis in the liver, while the remaining 30% of serum cholesterol comes from absorption from the intestine2). This situation is easy to understand when we think of the difference of efficacy of statin (inhibitor of cholesterol synthesis) and ezetimibe (inhibitor of cholesterol absorption), as well as the greater efficacy of combination therapy of both drugs3). However, this balance between cholesterol absorption and synthesis greatly varies according to different situations, such as diabetes and certain genetic disorders, including sitosterolemia caused by biallelic loss of function mutations in ATP-binding cassette subfamily G member 5 (ABCG5) or ATP-binding cassette subfamily G member 8 (ABCG8), where cholesterol absorption, rather than cholesterol synthesis, is greatly enhanced (Fig.1)4).
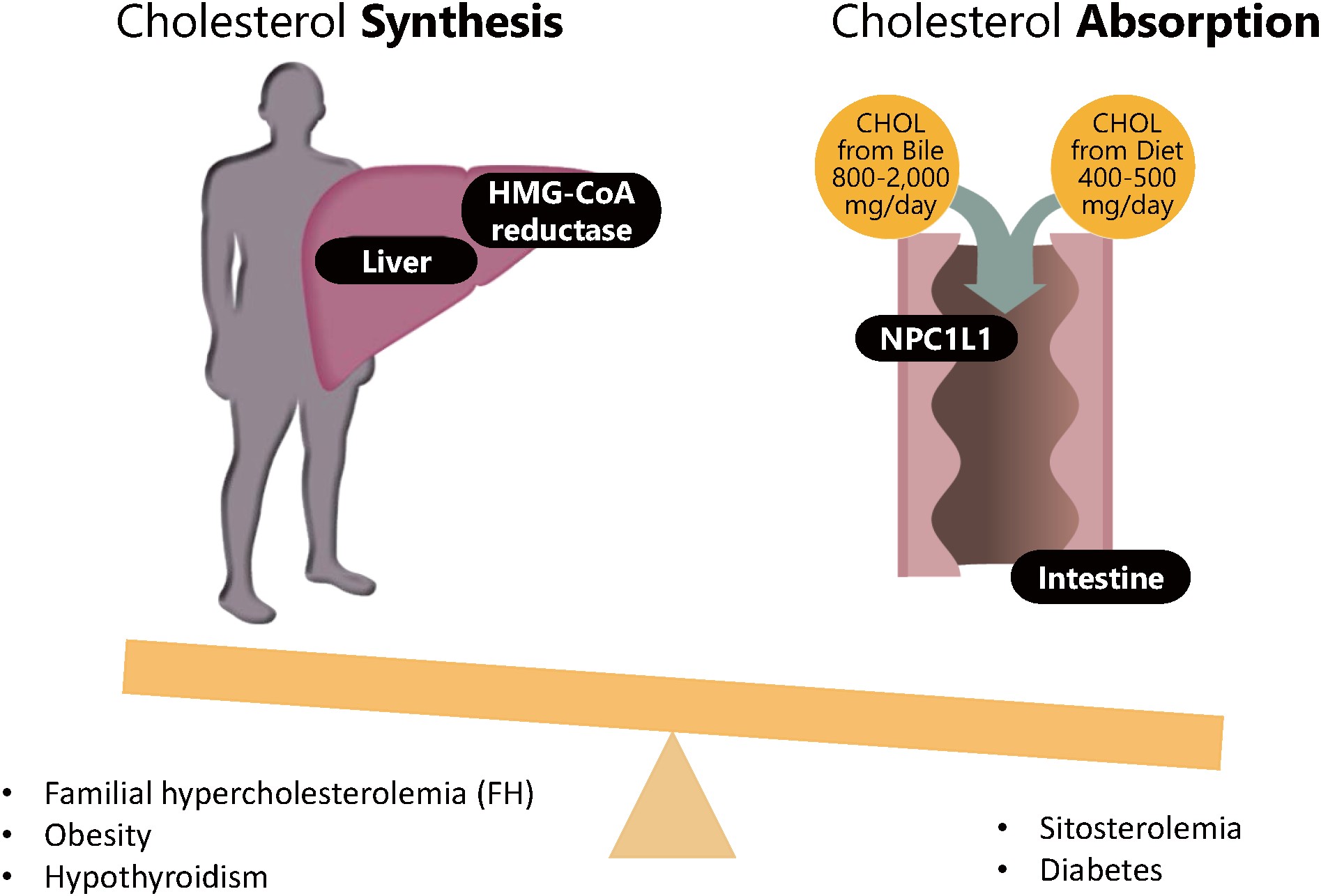
Cholesterol homeostasis in different situations
In accordance with the abovementioned notion, ezetimibe (inhibitor of cholesterol absorption) is more effective among patients with diabetes5), and more strikingly effective for patients with sitosterolemia6). Thus, biomarkers for cholesterol absorption and synthesis can be used to choose better strategies to reduce serum cholesterol, although statins are now recommended for the first usage, in general, based on their abundant clinical evidence without any assessments of cholesterol homeostasis. In this article, Ishibashi. et al.7) demonstrated “reference values” of cholesterol absorption and synthesis biomarkers among Japanese “healthy” individuals without diabetes or other genetic dyslipidemias. Currently, we never assess theses biomarkers before the initiation of cholesterol-lowering therapies. However, we might use these values to assess if a particular patient exhibits increased cholesterol absorption or synthesis, which should be used to better understand the situation or background of their dyslipidemia8).
Although statins (inhibitor of cholesterol synthesis) are now considered the first choice to reduce serum cholesterol, in general, precision medicine for hypercholesterolemia can be provided regarding this issue9, 10).
None
None
None