Abstract
Objectives: Efforts to improve performance in the workplace with respect to positive mental health have increased, and cognitive behavioral therapy (CBT) has recently attracted attention as an intervention measure to this end. Here, we conducted a randomized controlled trial to evaluate the effectiveness of a brief training program on CBT for improving work performance of employees. Methods: The participants were employees of an electric company in Japan. The intervention consisted of 1 group session of CBT (120 min) and web-based CBT homework for 1 month. We evaluated employees in both the intervention and control groups at baseline and follow-up after three months. The main outcome was work performance, which was evaluated by a subjective score from 1 to 10. The secondary outcome was self-evaluation of cognitive flexibility. Analyses were conducted based on ITT. Results: In the intervention group, 84 participants attended the group session, with 79 subsequently completing at least 1 instance of online homework. ITT analysis showed that the subjective performance of the intervention group was significantly improved compared with that of the control group (1.47 vs. 0.69, mean difference 0.78 [95% confidence interval {CI}, 0.05 to 1.51], Cohen's d=0.31). The ability to recognize dysfunctional thinking patterns and change them to positive ones significantly improved in the intervention group compared to the control group (0.71 vs. 0.26, mean difference 0.45 [95% CI 0.06 to 0.83], d=0.33). However, after adjustment for baseline scores, no significant difference was observed. The ability to view a situation from multiple perspectives and expand one's repertoire of thought patterns in the intervention group also significantly improved (0.83 vs. 0.35, mean difference 0.48 [95% CI 0.35 to 0.95], d=0.29), but here again, significance was lost after adjusting for baseline scores. Discussion: Our results suggest that a brief training program that combines a group CBT session with web-based CBT homework improved subjective work performance. In addition, this program might help improve employees' cognitive flexibility.
(J Occup Health 2015; 57: 169–178)
Introduction
Interest in maintaining and promoting positive mental health has increased in recent years. The World Health Organization defines positive mental health as a state of well-being in which each individual can recognize their own potential, deal with stress, contribute to the community and work productively. The WHO mental health action plan for 2013 to 2020 emphasizes the importance of providing public mental health intervention via non-pharmacological approaches1, 2). These increased efforts to ensure positive mental health are believed to influence mental health measures in the workplace3). Previous mental health services in the workplace have included the early detection and treatment of mental illness. At present, however, increasing emphasis is being placed on improving work performance from the view point of positive mental health2, 4).
A shift in approach from a risk-reduction model to a competence-enhancement model is required to improve work performance2). Several measures have been taken, the most reliable of which is intervention using psychotherapy techniques combined with cognitive behavioral therapy (CBT)5–7). CBT improves dysfunctional cognition and enhances the ability to manage problems in daily life8).
A number of studies have been conducted to elucidate the mechanism by which CBT improves mental health9, 10). The most probable theory is that CBT enhances cognitive flexibility, thereby inducing positive psychological changes11, 12). Cognitive flexibility is the ability to accept difficult situations and make them controllable, to perceive life events and the behaviors of others from multiple perspectives, and to formulate solutions from those perspectives. Mastering CBT has been reported to improve all of these abilities6).
A study of healthy subjects reported that scoring cognitive flexibility helped to estimate how well subjects performed in vigilance tasks13) and that cognitive flexibility enhanced creativity and the ability to form new ideas14). In addition, people with a positive disposition tended to have a higher level of cognitive flexibility and completed tasks that required creativity15). We therefore consider enhancement of cognitive flexibility with CBT to improve work performance13). To our knowledge, however, only a few studies have analyzed whether or not intervention using CBT actually improves the performance of employees16, 17).
CBT has mainly been used in face-to-face psychotherapy. However, there are several factors preventing the distribution of effective mental health and medical services, such as medical economy, equity, and lack of analysis. Therefore, low-intensity and easy-to-implement intervention programs based on CBT are recommended. Such programs include the provision of information and psychological education via books, materials, and group sessions, as well as CBT via e-mail, phone, and online programs that can be independently accessed1, 18). Such brief CBT programs to reduce depression and anxiety have indeed been found easy to implement in the workplace and effective19, 20).
Here, we conducted a randomized controlled trial consisting of a brief training program based on CBT (short-term and available in the workplace) among employees to evaluate subsequent improvements in work performance.
Methods
Participants and study design
All participants were employees working in the headquarters of an electric company in Japan. Employees included managers, engineers, and office workers. We explained the purpose and process of the study via e-mail, and those who consented were enrolled. No exclusion criteria were set. Participants were allocated into non-blinded intervention or control groups.
Ethics statement
The study protocol was reviewed and approved by the Safety and Hygiene Committee of the electric company and by the Institutional Ethics Committee of Kitasato University. The Safety and Hygiene Committee of the company deemed registration of the employee's data at any facility apart from that of the study enforcer inappropriate; we therefore did not conduct center registration.
Intervention
The intervention consisted of a 120-min group class on CBT and web-based CBT homework over a one-month period. Three group sessions of 30 to 35 participants each were held for the intervention group. Intervention was provided from May to July of 2012. The contents of the program are shown in Table 1.
Table 1.
The contents of the program
| Group session (2 hours) |
Part 1. Lecture
-
- The relationship between cognition, mood, and behavior
-
- What is CBT?
-
- Benefits of learning CBT as stress management skills and how to apply it to the real life with examples
|
Part 2. Group work and discussion; cognitive restructuring skill
-
- How to fill out the column worksheet??
-
- Recognizing automatic thoughts of their own
-
- Group discussion about evidence that is against their own thought and adaptive thought
-
- How to use self-help-style online homework tools
|
| Personal web training (homework) |
Fill out the column worksheet using the web-based CBT program (recommended to take more than twice)
-
- Fill out the column worksheet by entering information as directed on the online screen
-
- The online program provides contextual explanations and advice on the column method
|
The group session was a 120-min group class presented by a CBT specialist. Participants were placed in groups of 5 to 7, with groups arranged to have most members be around the same age to ensure that they were able to speak their minds freely. First, participants learned about the relationship between, emotions, cognition and behavior, which is the basis of CBT. We included practical examples and excluded technical terms from all explanations to facilitate understanding in the session. Second, participants completed a column worksheet to aid in the application of CBT theory to real-life situations. Column worksheets are often used for cognitive restructuring in CBT by having participants fill out a column including situation, mood, automatic thought, evidence that supports their automatic thought, evidence that is against their automatic thought, adaptive thoughts, and mood changes. This process helps people separate their problems from themselves, deal with them in an objective manner, and replace dysfunctional thinking with realistic and balanced thinking. In this training program, we referred to this column worksheet as the “Thought Balance Sheet”. Participants filled in this sheet with their experiences and situations and learned how to best utilize the sheet. In this session, participants were asked to select light, nonserious situations, as they would later discuss their concerns with the group members. Regarding automatic thought, we introduced certain thought patterns that can cause stress (such as all-or-nothing thought, should be thought, self-criticism, over-interpreting) to help subjects become aware of their own thought patterns. Participants were assigned to work on the thought balance sheet as a group by considering evidence that supports their way of thinking, does not support their way of thinking, and adaptive thought. During this process, we provided multiple opportunities for participants to discuss their concerns and listen to the opinions of others. At the end of the course, we shared the completed thought balance sheets with each of the groups as well as the results of the session. We also allocated one computer per group to demonstrate how to complete the thought balance sheet with a web-based CBT training program and created an environment for participants to independently work on the thought balance sheet after the session using this tool.
Online homework using the web-based CBT program
Participants were asked to practice the column method using a self-help-style program by reflecting on any significant work-related stress they experienced over the one-month period starting the day after the group education session. Homework was expected to help familiarize participants with the column method. As material for this homework, we used the “Depression & Anxiety Network—Mental Health Skill-up Training program” (http://www.cbtjp.net/). This website, which was developed by a CBT specialist and is accessible to the general public, provides self-help-style training programs on coping with stress for not only those with depression or anxiety disorders but also healthy people with casual concerns or difficulties. The recommended web program helps participants easily complete the thought balance sheets by providing contextual explanations and advice on the column method. Participants can complete their sheets by entering information as directed on the screen. The column method was expected to help the participants overcome their difficulties by changing negative and dysfunctional thinking patterns into flexible ones6).
We recommended that participants complete the online thought balance sheet, which takes approximately 30 minutes, at least 3 times. In previous studies evaluating the effect of low-intensity CBT, the mean number of CBT sessions ranged from 6 to 7 and showed a high dropout rate during implementation21). However, another study using an intervention method similar to that in the present study and conducted in health workers in Japan showed that CBT training using one group session and three e-mail sessions was effective in improving depression with a relatively low dropout rate19). In the present study, we asked participants to complete the web-based CBT homework at least three times to ensure feasibility and avoid placing further pressure on busy participants and exacerbating dropout rates.
We arranged for the web-based CBT program to focus mainly on the contents of the thought balance sheet and guidance from the website. We also arranged an ID and password to secure a personal account for each participant. Each account was private, and the system administrator, CBT specialist who conducted group session, and occupational physician were not allowed access. The system administrator could only verify the number of times each participant completed the thought balance sheet. This online homework was able to be accessed at the office and at home.
The occupational physician sent a reminder e-mail approximately once a week. This e-mail provided information on CBT and encouraged participants to continue completing web-based CBT. For ethical reasons, the same program (group session and online homework) was provided to the control group after analyses were completed.
Outcomes
We used an online questionnaire and evaluated baseline measures and outcomes after three months for both the intervention and control groups.
The primary outcome was subjective work performance. On a scale of 1 to 10, participants assessed their work performance three months after the intervention by answering, “How was your work performance in the past month compared to the one before? Please score below”, with response options ranging from “1: The worst in your working life” to “10: The best in your working life”.
The secondary outcome was self-rating of cognitive flexibility. This was assessed based on responses to two items originally designed to evaluate cognitive flexibility, which can be improved by training in basic concepts of CBT. The first item was, “I can recognize dysfunctional thinking patterns and change them to flexible ones”, followed by response options ranging from “1: Not applicable” to “5: Applicable”. The second item was, “I can see the situation from multiple perspectives and expand the repertoire of my way of thinking”, followed by response options ranging from “1: Never” to “5: Very well”.
Information on gender, age, family makeup, mean hours of sleep on weekdays, history of mental disease, job title, years of employment, hours of overtime a month, self-evaluation of support from their superiors or colleagues (10-point Likert scale: 0, never supportive, to 10, very supportive), and self-evaluation of stress in the workplace (10-point Likert scale: 0, never stressful, to 10, very stressful) were inquired about at baseline.
Randomization and masking
An independent researcher who had no direct contact with the participants used computer-generated randomization with a 1:1 ratio and block size of 6. No stratification was performed. Evaluators were masked to allocation. Due to the nature of the intervention, participants were aware of their allocation status.
Statistical analysis
A previous study that analyzed the effectiveness of CBT regarding quality of work reported a score of 0.48 for Cohen's d21). The sample size necessary to obtain an effect size of 0.48 with a probability of Type I error (α) less than 0.05 and Type II error (β) less than 0.20 was 95 per group. To satisfy the ITT requirement that analyses be conducted for all participants, a multiple imputation (MI) method was used on the assumption that data could be considered missing at random. MI compensates for uncertainty caused by missing data by generating several different plausible imputed data sets using a set of external covariates and appropriately combining results obtained from each22, 23). We utilized a sequential regression approach to generate 20 imputations for each missing value, as recommended by Graham24).
The effectiveness of the intervention was evaluated based on the change in the subjective work performance and cognitive flexibility of participants from baseline to follow-up after three months. These changes were also compared in the intervention and control groups using a generalized estimating equations model. Additionally, mean differences were adjusted using the baseline scores. IBM SPSS Ver. 18 (SPSS Inc., Chicago, IL, USA) statistical analysis software was used.
Results
Study flow
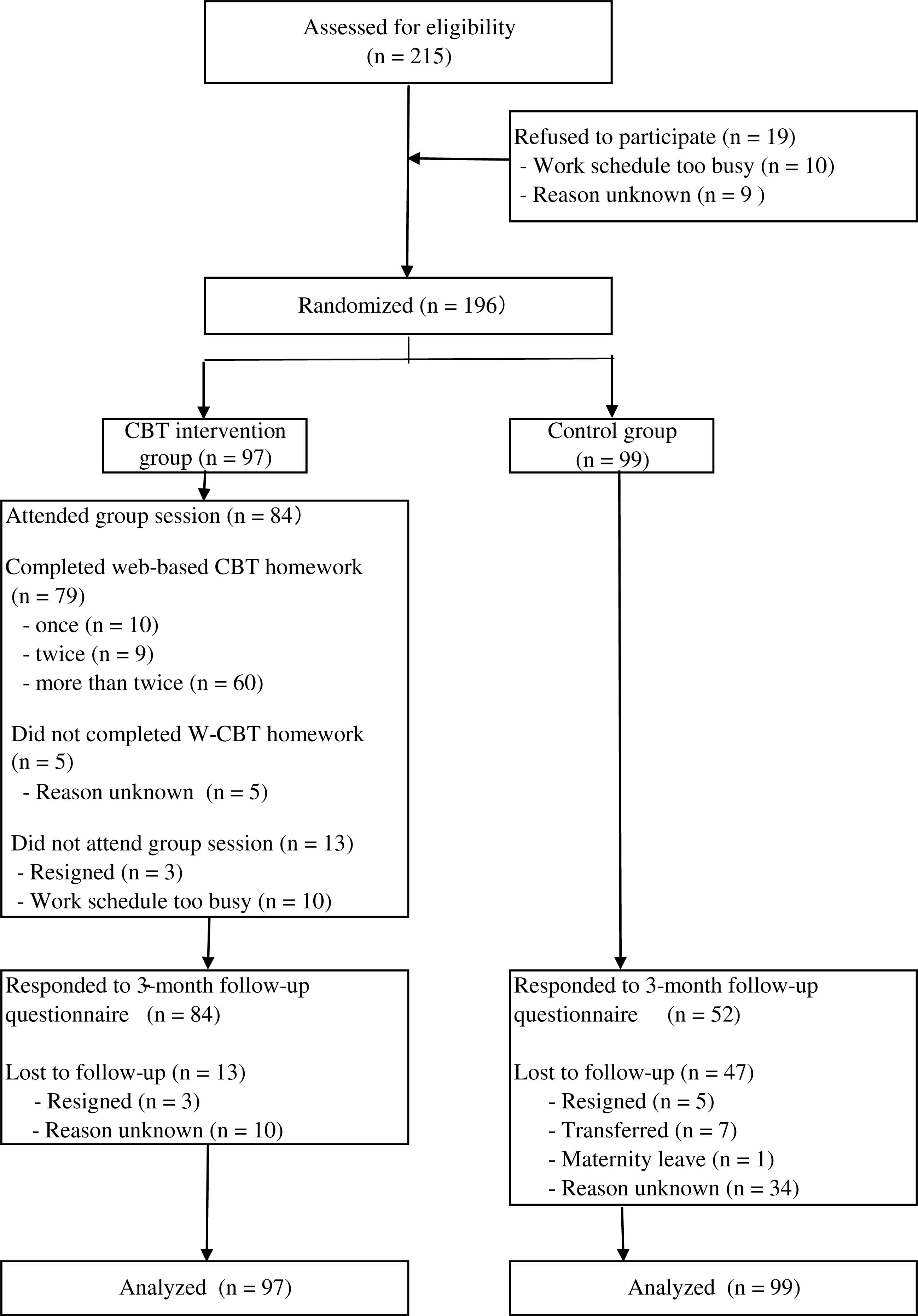
The flow of the present study is shown in Fig. 1. The participants consisted of 215 employees, with no exclusions from the study. The 196 participants who agreed to enroll were allocated to the intervention (n=97) or control group (n=99). All participants answered the baseline questionnaire. In the intervention group, 84 participants (86.6%) attended the group session. Thirteen participants did not attend, namely, three who resigned from the company and ten who were unable to attend due to their work schedule.
Of 84 who attended the group session, 79 participants completed the online homework at least once. Ten participants attended the training program on CBT once, 9 attended it twice, and 60 attended more than twice. The reasons why five participants failed to complete even one online session are unknown.
At follow-up three months after the training program on CBT, the questionnaire was completed by 84 participants in the intervention group and 52 participants in the control group. Based on the ITT principle, all participants (97 in the intervention group and 99 in the control group) were enrolled in the analyses.
Baseline characteristics
The baseline characteristics of the participants are shown in Table 2. Most participants were men (85.6% in the intervention group, 85.9% in the control group). The mean age was 46.4 years (SD=13.6) in the intervention group and 44.7 years (SD=12.7) in the control group. No significant differences were noted between the two groups for gender, age, marital status, family makeup, mean hours of sleep on weekdays, history of mental disease, job title, years of employment, hours of overtime a month, support from their superiors or colleagues, stress in the workplace, score of subjective work performance, or ability to recognize dysfunctional thinking patterns and change to flexible ones or to view a situation from multiple perspectives.
Table 2.
The baseline data of the study participants
| Characteristics |
Total n=196 |
Intervention group n=97 |
Control group n=99 |
p valuea) |
| Sex |
| Male, n (%) |
168 (85.7%) |
83 (85.6%) |
85 (85.9%) |
0.95 |
| Female, n (%) |
28 (14.3%) |
14 (14.4%) |
14 (14.1%) |
|
| Age in years, mean (SD) |
45.4 (13.1) |
46.4 (13.6) |
44.7 (12.7) |
0.37 |
| Title, n (%) |
| Managers |
43 (21.9%) |
21 (21.6%) |
22 (22.2%) |
0.43 |
| Engineers |
37 (18.9%) |
23 (23.7%) |
14 (14.1%) |
|
| Non title |
85 (43.4%) |
50 (51.5%) |
35 (35.4%) |
|
| Missing, n (%) |
31 (15.8%) |
3 ( 3.1%) |
28 (28.3%) |
|
| Years of employment, n (%) |
| Shorter than 10 years |
18 ( 9.2%) |
13 (13.4%) |
5 (7.0%) |
0.31 |
| 10 years or longer |
147 (75.0%) |
81 (83.5%) |
66 (93.0%) |
|
| Missing, n (%) |
31 (15.8%) |
3 ( 3.1%) |
28 (28.3%) |
|
| Marital status, n (%) |
| Unmarried |
41 (20.9%) |
25 (25.8%) |
16 (16.2%) |
0.52 |
| Married |
123 (62.8%) |
68 (70.1%) |
55 (55.6%) |
|
| Missing, n (%) |
31 (15.8%) |
3 ( 3.1%) |
28 (28.3%) |
|
| Family members, n (%) |
| Live alone |
31 (15.8%) |
16 (16.5%) |
15 (15.2%) |
0.48 |
| Live with family |
133 (67.9%) |
78 (80.4%) |
55 (55.6%) |
|
| Missing, n (%) |
31 (15.8%) |
3 ( 3.1%) |
28 (28.3%) |
|
| History of mental disease, n (%) |
| Have no history |
148 (75.5%) |
83 (85.6%) |
65 (65.7%) |
0.38 |
| Have history |
10 ( 5.1%) |
5 ( 5.2%) |
5 (5.1%) |
|
| Undergoing treatment |
6 ( 3.1%) |
5 ( 5.2%) |
1 (1.0%) |
|
| Missing, n (%) |
31 (15.8%) |
3 ( 3.1%) |
28 (28.3%) |
|
| Mean hours of sleep (weekdays), n (%) |
| Less than 5 h |
26 (13.3%) |
13 (13.4%) |
13 (13.1%) |
0.73 |
| 5–6 h |
118 (60.2%) |
69 (71.1%) |
49 (49.5%) |
|
| 7–8 h |
21 (10.7%) |
12 (12.4%) |
9 (9.1%) |
|
| Missing, n (%) |
31 (15.8%) |
3 ( 3.1%) |
28 (28.3%) |
|
| Hours of overtime a month, n (%) |
| 0–20 h |
124 (63.3%) |
68 (70.1%) |
56 (56.6%) |
0.33 |
| 20–45 h |
38 (19.4%) |
24 (24.7%) |
14 (14.1%) |
|
| Over 45 h |
3 ( 1.5%) |
2 ( 2.1%) |
1 (1.0%) |
|
| Missing, n (%) |
31 (15.8%) |
3 ( 3.1%) |
28 (28.3%) |
|
| Support in the workplace, mean (SD) |
6.4 (2.1) |
6.6 (2.1) |
6.1 (2.2) |
0.47 |
| Stress in the workplace, mean (SD) |
5.8 (2.2) |
5.9 (2.0) |
5.5 (2.3) |
0.41 |
| Baseline outcome scores |
| Work performance, mean (SD) |
5.9 (1.6) |
5.8 (1.7) |
5.9 (1.5) |
0.54 |
| Ability to recognize dysfunctional thinking patterns and change to flexible ones, mean (SD) |
3.3 (1.0) |
3.2 (1.0) |
3.4 (0.9) |
0.2 |
| Ability to view the situation from multiple perspectives, mean (SD) |
3.6 (1.0) |
3.5 (1.1) |
3.6 (1.0) |
0.89 |
a) A
t-test was used for numerical variables, and a Fisher's exact test for categorical variables.
Table 3 shows the results of the CBT intervention. From baseline to three months after the intervention, the mean subjective work performance score significantly increased in the intervention group compared to the control group (1.47 vs. 0.69, mean difference 0.78 [95% confidence interval {CI}, 0.05 to 1.51], p=0.04). The effect size (Cohen's d) was 0.31 and persisted even after adjustment for baseline performance scores (mean difference 0.72 [95% CI 0.01 to 1.44], p=0.049). In the per protocol analysis including 60 participants who completed the web-based CBT program at least three times, the subjective work performance score also significantly increased in the intervention group compared to the control group (mean difference 0.79 [95% CI, 0.19 to 1.38], p=0.01) and persisted even after adjustment for baseline performance scores (mean difference 0.76 [95% CI 0.27 to 1.26], p=0.003).
Table 3.
Change in the score for primary and secondary outcomes after 3-month follow up
|
Mean (SE) change |
Unadjusted difference in mean (95% CI) |
p value |
Adjusted difference in mean (95% CI)a) |
p value |
| Intervention group |
Controls |
| Work performance |
1.47 (0.30) |
0.69 (0.21) |
0.78 (0.05 to 1.51) |
0.04 |
"0.72 (0.01 to 1.44) |
0.049 |
| Ability to recognize dysfunctional thinking patterns and change to flexible ones |
0.71 (0.17) |
0.26 (0.10) |
0.45 (0.06 to 0.83) |
0.03 |
0.30 (−0.04 to 0.65) |
0.09 |
| Ability to view the situation from multiple perspectives |
0.83 (0.20) |
0.35 (0.13) |
0.48 (0.35 to 0.95) |
0.04 |
0.13 (−0.91 to 0.67) |
0.14 |
a) Adjusted for baseline scores.
The ability to recognize dysfunctional thinking patterns and change them to positive ones significantly improved in the intervention group compared to the control group (0.71 vs. 0.26, mean difference 0.45 [95% CI 0.06 to 0.83], p=0.03, d=0.33). However, after adjustment for baseline scores of ability to recognize dysfunctional thinking patterns and change them to positive ones, no significant differences were observed. The ability to view a situation from multiple perspectives and expand one's repertoire of thought patterns in the intervention group also significantly improved (0.83 vs. 0.35, mean difference 0.48 [95% CI 0.35 to 0.95], p=0.04, d=0.29). However, here again, after adjustment for baseline scores of ability to recognize dysfunctional thinking patterns and change them to positive ones, no significant differences were observed.
Study safety
This study did not exacerbate any existing psychological problems of any participants.
Discussion
Here, we demonstrated that a brief training program based on CBT is effective in improving employees' subjective work performance. Ours is one of the few randomized controlled studies to investigate the efficiency of a brief training program on CBT to improve the performance of employees from the viewpoint of positive mental health.
Studies of CBT intervention have previously involved mental disorders in the workplace and demonstrated that CBT is effective in improving depression and anxiety, as well as reducing stress21, 25–27) and absenteeism28). From the viewpoint of positive mental health, additional benefits of mental health promotion have been observed, such as improving quality of work21) and quality of life26), promoting work function29), improving performance16, 17) and reducing turnover16). However, implementation of these CBT methods requires a substantial amount of time and constant involvement from CBT specialists and is therefore difficult to perform in the workplace. A possible solution is therefore brief and easy-to-implement CBT including provision of information on CBT via books, group training, telephone, and the Internet in a self-study format. However, while intervention using brief CBT has been reported to reduce depression, anxiety, stress19, 20, 25), and absenteeism30, 31), to our knowledge, few reports have remarked on intervention via brief CBT to increase positive mental health including work performance, which is of key importance in the workplace.
Proudfoot et al. (2009) provided CBT training that consisted of 3-hour sessions once a week, for 7 weeks to employees in the sales division of a financial services company and examined their sales after 2 years. On follow-up, 65% of employees achieved figures above their sales or earnings targets. Considering that, before the training, only 2% of the participants were reaching an acceptable level, they concluded that CBT training had a positive impact on the productivity of these employees16). Lam et al. (2011) provided eight 30-min CBT sessions via telephone to 39 employees with a depression score of five or more as assessed via the Personal Health Questionnaire 9-item Depression Module (PHQ-9). Post intervention, they observed a significant improvement in both PHQ-9 score and Performance Impairment, i.e., self-evaluation of their decreased performance (scale from 0 to 3)17). However, neither this study nor that by Proudfoot et al. were randomized controlled trials. In contrast, the present study was a randomized controlled trial using a brief CBT education program that can be implemented in a variety of companies to improve work performance.
The following two points were of key importance in achieving an easy-to-implement and effective intervention for work performance using brief CBT in the workplace. The first point is that education in the workplace should be brief to minimize interruption and ensure provision to as many employees as possible. Regarding CBT education, we used a combination of simple CBT methods, such as a 120-min group session in the workplace and at least 3 sessions of online homework (each session approximately 30 min), which was less time-consuming than previous interventions using CBT18). The second point is maintenance of subject motivation. We convinced employees at the group session that CBT training can be effective not only in treating mental disorders but also in maintaining dysfunctional thinking patterns and improving work performance32, 33). In addition, an occupational physician sent a weekly e-mail reminder, as reminders have been reported to help improve rate of completion of self-help CBT training34, 35).
In the intervention group of the present study, 86.6% of subjects (84/97) attended the group session. Of these 84 subjects, 60 completed web-based CBT homework at least three times, 9 completed it twice, and 10 completed it once, with only 6.0% (5/84) never completing web-based CBT homework. In general, dropout rates for online self-training programs are relatively high, with meta-analysis showing that an average of 31.8% of participants drop out of online CBT training for the treatment of depression36). Given that the dropout rate in interventions for healthy subjects tends to be higher7), we considered the completion rate in the present study to be acceptable. This relatively high completion rate and effectiveness of the present study might be attributed to the two key points above.
The mechanism for how CBT improves work performance is unclear. The most probable theory is that CBT enhances cognitive flexibility, thereby inducing positive psychological changes that might help improve workplace performance11, 12). A previous study similarly showed that cognitive flexibility can be improved by mastering CBT6).
Cognitive flexibility involves the acceptance of difficult situations to make them controllable and the ability to perceive life events and the behavior of others from multiple points of view6), two tasks that can be improved through CBT. For example, repairing a subject's dysfunctional cognition might improve their flexibility regarding a new way of thinking and action11, 12), help them accept their role in a problem, find more solutions for the problem, and take action appropriate to a given situation37). In a study of healthy subjects, groups who had low-level cognitive restructuring tended to have low-level cognitive flexibility38).
Several reports have described the connection between cognitive flexibility and performance. Figueroa et al. (2012) investigated the prediction of good performance in a vigilance task that requires rapid responses via cognitive flexibility and found that, as this flexibility improves, so too does the score for relatively difficult tasks13). Youmas et al. (2011) showed that subjects with high cognitive flexibility noticed minor changes in the environment and reacted39). In other words, cognitive flexibility is the ability and tendency to quickly exchange one cognitive strategy for another13), which might subsequently improve performance in tasks requiring prompt decisions and action. De Dreu et al. (2008) suggested that cognitive flexibility influenced fluent creativity (number of ideas and thoughts) and originality14). Activated emotions (anger, fear, happiness, and joy) bring more creativity and originality than deactivated emotions (sadness, depression, and relaxation), and activated emotions increased fluent and original creativity by enhancing cognitive flexibility14).
In the present study, self-confidence regarding one's ability to recognize dysfunctional thinking patterns and change them to flexible ones and the ability to view a situation from multiple perspectives and expand one's repertoire of thought patterns were significantly higher in the intervention group than in the control group. After adjustment for baseline scores, confidence in both abilities improved even further, although no statistically significant differences were observed. However, we believe that these results suggest a potential relationship between improved work performance and improved confidence in ability to change dysfunctional thinking patterns into flexible ones and ability to view a situation from multiple perspectives.
Limitations of the present study
Several limitations of the present study warrant mention, as follows:
-
1) Our study was only conducted in one workplace that contained more men than women.
-
2) The number of participants who completed the web-based CBT program at least 3 times as per the protocol was 60 (61.9%), and the response rate for the questionnaire was very low in the control group.
-
3) The evaluations for performance and cognitive flexibility were subjective, and the questionnaire was our own and had not been validated.
-
4) The web-based CBT training was a self-help program, and we were unable to check the extent to which participants worked on a given assignment. As we made the website inaccessible to anyone other than the participants themselves to protect their privacy and ensure ease of use, we do not know if the participants were able to use the tool and master CBT.
-
5) Follow-up was evaluated only once, three months after the training, and we did not conduct our research in a time-interactive way. More research is therefore required to determine how long positive effects are maintained.
-
6) We did not register the trial in any database due to concerns of the company involved regarding the confidentiality of employees' health data.
A high-intensity CBT approach, such as one-on-one counseling, is personal and can provide high-quality service, but requires more time and the constant involvement of a CBT specialist. Therefore, implementation in the workplace is difficult. By using a brief CBT education program, we can effectively influence many employees who do not have the opportunity to receive CBT therapy and training2). Intervention can also help employees who are already mentally healthy further promote their mental health and improve work performance from the perspective of positive mental health40).
To our knowledge, however, only a few studies have investigated whether or not training based on CBT can improve the performance of employees. A variety of positive mental health programs need to be developed for mentally healthy employees in a variety of industries, and the effectiveness of these programs needs to be evaluated through more randomized controlled trials.
Conflicts of interest: None declared. The authors are distinct from the developers/sponsors of the present web-based CBT program system.
References
- 1) Mental health action plan 2013–2020: World Health Organization, [Online]. 2013 [cited 2014 Aug 13]; Available from: URL: http://www.who.int/mental_health/publications/action_plan/en/index.html
- 2) Fledderus M, Bohlmeijer ET, Smit F, Westerhof GJ. Mental health promotion as a new goal in public mental health care: a randomized controlled trial of an intervention enhancing psychological flexibility. Am J Public Health 2010; 100: 2372-8.
- 3) Slade M. Mental illness and well-being: the central importance of positive psychology and recovery approaches. BMC Health Serv Res 2010; 10: 26.
- 4) McDaid D, Curran C, Knapp M. Promoting mental well-being in the workplace: a European policy perspective. Int Rev Psychiatr 2005; 17: 365-73.
- 5) Sin NL, Lyubomirsky S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. J Clin Psychol 2009; 65: 467-87.
- 6) Dennis JP, Vander Wal JS. The cognitive flexibility inventory: instrument development and estimates of reliability and validity. Cognitive Ther Res 2010; 34: 241-53.
- 7) Powell J, Hamborg T, Stallard N, et al. Effectiveness of a web-based cognitive-behavioral tool to improve mental well-being in the general population: randomized controlled trial. J Med Internet Res 2013; 15: e2.
- 8) Young JE, Weinberger AD, Beck AT. Cognitive therapy for depression. In Barlow D.H. (Ed.), Clinical handbook of psychological disorders: A step-by-step treatment manual (3rd ed.). New York, Guilford Press, 2001: 264-308.
- 9) DeRubeis RJ, Evans MD, Hollon SD, et al. How does cognitive therapy work- Cognitive change and symptom change in cognitive therapy and pharmacotherapy for depression. J Consult Clin Psych 1990; 58: 862-9.
- 10) Hayes AM. Strauss JL. Dynamic systems theory as a paradigm for the study of change in psychotherapy: an application to cognitive therapy for depression. J Consult Clin Psych 1998; 66: 939-47.
- 11) Fresco DM, Rytwinski NK, Craighead LW. Explanatory flexibility and negative life events interact to predict depression symptoms. J Soc Clin Psychol 2007; 26: 595-608.
- 12) Moore MT, Fresco DM. The relationship of explanatory flexibility and explanatory style. Behav Ther 2007; 38: 325-32.
- 13) Figueroa IJ, Youmans RJ. Individual differences in cognitive flexibility predict performance in vigilance tasks. Proceedings of the human factors and ergonomics society annual meeting 2012; 56: 1099-103.
- 14) De Dreu CK, Baas M, Nijstad BA. Hedonic tone and activation level in the mood-creativity link: toward a dual pathway to creativity model. J Pers Soc Psychol 2008; 94: 739-56.
- 15) Hirt ER, Devers EE, McCrea SM. I want to be creative: exploring the role of hedonic contingency theory in the positive mood-cognitive flexibility link. J Pers Soc Psychol 2008; 94: 214-30.
- 16) Proudfoot JG, Corr PJ, Guest DE, et al. Cognitive-behavioural training to change attributional style improves employee well-being, job satisfaction, productivity, and turnover. Pers Indiv Differ 2009; 46: 147-53.
- 17) Lam RW, Lutz K, Preece M, et al. Telephone-administered cognitive-behavioral therapy for clients with depressive symptoms in an employee assistance program: a pilot study. Ann Clin Psychiatry 2011. 23: 11-6.
- 18) Cape J, Whittington C, Buszewicz M, Wallace P, Underwood L. Brief psychological therapies for anxiety and depression in primary care: meta-analysis and meta-regression. BMC Med 2010; 8: 38.
- 19) Kojima R, Fujisawa D, Tajima M, et al. Efficacy of cognitive behavioral therapy training using brief e-mail sessions in the workplace: a controlled clinical trial. Ind Health 2010; 48: 495-502.
- 20) Furukawa TA, Horikoshi M, Kawakami N, et al. Telephone cognitive-behavioral therapy for subthreshold depression and presenteeism in workplace: a randomized controlled trial. PLoS One 2012; 7: e35330.
- 21) van der Klink JJ, Blonk RW, Schene AH, et al. The benefits of interventions for work-related stress. Am J Public Health 2001; 91: 270-6.
- 22) Rubin D. Multiple imputation for nonresponse in surveys. New York: John Wiley and Sons. 1987.
- 23) Donders AR, van der Heijden GJ, Stijnen T, et al. Review: a gentle introduction to imputation of missing values. J Clin Epidemiol 2006; 59: 1087-91.
- 24) Graham JW. Missing data analysis: Making it works in the real world. Ann Rev Psychol 2009; 60: 549-76.
- 25) Graveling RA, Crawford JO, Cowie H, et al. A Review of workplace interventions that promote mental well-being in the workplace. National Institute for Health and Clinical Excellence, Edinburgh. [Online]. 2008 [cited 2014 Aug 13]; Available from: URL: http://www.academia.edu/271180/A_review_of_workplace_interventions_thatpromote_mental_wellbeing_in_the_workplace
- 26) Bhui KS, Dinos S, Stansfeld SA, White PD. A synthesis of the evidence for managing stress at work: a review of the reviews reporting on anxiety, depression, and absenteeism. J Environ Public Health 2012; 2012: 515874.
- 27) Marine A, Ruotsalainen J, Serra C, Verbeek J. Preventing occupational stress in healthcare workers. Cochrane Database Syst Rev [published online ahead of print October 18, 2006]. CD002892.
- 28) de Vente W, Kamphuis JH, Emmelkamp PM, et al. Individual and group cognitive-behavioral treatment for work-related stress complaints and sickness absence: a randomized controlled trial. J Occup Health Psych 2008; 13: 214-31.
- 29) Pomaki G, Franche RL, Murray E, et al. Workplace-based work disability prevention interventions for workers with common mental health conditions: a review of the literature. J Occup Rehabil 2012; 22: 182-95.
- 30) Grime PR. Computerized cognitive behavioural therapy at work: a randomized controlled trial in employees with recent stress-related absenteeism. Occup Med (Lond) 2004; 54: 353-9.
- 31) Bee PE, Bower P, Gilbody S, et al. Improving health and productivity of depressed workers: a pilot randomized controlled trial of telephone cognitive behavioral therapy delivery in workplace settings. Gen Hosp Psychiat 2010; 32: 337-40.
- 32) Hasson H, Brown C, Hasson D. Factors associated with high use of a workplace web-based stress management program in a randomized controlled intervention study. Health Educ Res 2010; 25: 596-607.
- 33) Donkin L, Glozier N. Motivators and motivations to persist with online psychological interventions: a qualitative study of treatment completers. J Med Internet Res 2012; 14: e91.
- 34) Christensen H, Griffiths KM, Jorm AF. Delivering interventions for depression by using the internet: randomized controlled trial. BMJ. 2004 Jan 31; 328 (7434): 265. 2004; 328: 265.
- 35) Clarke G, Eubanks D, Reid E, et al. Overcoming depression on the Internet (ODIN) (2): a randomized trial of a self-help depression skills program with reminders. J Med Internet Res 2005; 7; e16.
- 36) Kaltenthaler E, Sutcliffe P, Parry G, et al. The acceptability to patients of computerized cognitive behavior therapy for depression: a systematic review. Psychol Med 2008; 38: 1521-30.
- 37) Crowe M, Whitehead L, Carlyle D, et al. The process of change in psychotherapy for depression: helping clients to reformulate the problem. J Psychiatr Ment Health Nurs 2012; 19: 681-9.
- 38) Johnco C, Wulthrich VM, Rapee RM. The role of cognitive flexibility in cognitive restructuring skill acquisition among older adults. J Anxiety Disord 2013; 27: 576-84.
- 39) Youmans RJ, Figueroa IJ, Kramarova O. Reactive task-set switching ability, not working memory capacity, predicts change blindness sensitivity. Proceedings of the Human Factors and Ergonomics Society Annual Meeting 2011; 55: 914-8.
- 40) Schueller SM, Parks AC. Disseminating self-help: positive psychology exercises in an online trial. J Med Internet Res 2012; 14: e63.