Abstract
Abstract: A study was conducted to evaluate the success rates of bypassing or removing fragments of instruments that had fractured within the roots of mandibular molars using a HBW Ultrasonic Ring. Forty extracted first permanent mandibular molars with root canal curvature were included. The teeth were distributed randomly into four groups according to the type of instrument and the root canal third where they had fractured. The success rate for removal of instrument fragments was 100% for both of two stainless steel groups, 90% for a nitinol middle third group, and 80% for a nitinol apical third group. The mean time required for instrument removal was around 40 min. The HBW Ultrasonic Ring showed acceptable experimental results for retrieval of broken instrument fragments.
Introduction
The separation or fracture of an endodontic instrument within the root canal system represents an unfortunate negative event that can potentially affect the outcome of endodontic treatment, as it hampers adequate chemo-mechanical disinfection, debridement, and shaping of the pulp canal. The mode of such separation has not yet been clearly explained, but interaction of metal torsional and bending forces, instrument overuse, and subsequent distortion, deformation, and flexural fatigue are likely contributing factors [1]. Fracturing of a wide range of instruments has been reported, although the literature has mostly described fracture of stainless steel (SS) files and rotary NiTi (nitinol) instruments; the latter have been considered to have a higher risk of separation/fracture than traditional SS instruments [2].
For management of instrument parts or fragments, either orthograde maneuvers (file removal, fragment bypassing, cleaning/shaping and sealing the root canal to the level of the fragment obstruction) or surgical approaches have been described [3]. In general, the optimum management option is considered to be removal of the fragment so that cleaning and shaping of the root canal system can be completed effectively. However, even if fragment removal is achieved, any attempt may lead to ledge formation, over-enlargement, or weakening of the prepared pulp canal due to excessive loss of the dentin walls, making the root prone to fracture [4].
Ultrasonic techniques under observation with a dental operating microscope have been reported to be successful and safe for removal of separated instrument parts [4,5]. In 2020, Galván-Pacheco et al. [6] reported a technique utilizing the HBW Ultrasonic Ring, a device that performs instrumentation and irrigation simultaneously; it also activates endodontic instruments, transforming them into potential ultrasonic instruments. Potentially, the HBW Ultrasonic Ring could also be a highly effective technique for removal of intracanal separated instrument parts. Although the technique is time-consuming, it has a range of clinical advantages for both gaining access to an obstruction and removal of a separated fragment, preserving dentin wall integrity to a large extent [5].
The aims of the present in vitro study were to assess the effectiveness of the HBW Ultrasonic Ring for removal of intentionally fractured instruments within the pulp canal (at two different levels), and to determine whether the effectiveness would differ in terms of outcome through comparison of retrieved fragments from rotatory NiTi or manual SS instruments.
Materials and Methods
The present in vitro study was conducted at the Postgraduated Department of Endodontics, Faculty of Dentistry, Autonomous University of San Luis Potosí, and its protocol was approved by the institutional ethics committee (code: CEIFE-042021). On the basis of the calculated total sample size [5,7], 40 extracted intact human first permanent mandibular molars were collected from patients attending the faculty. All patients provided informed consent to the use of their extracted teeth for scientific research. All experimental procedures were standardized and previously calibrated according to a predesigned protocol [5], and performed by two experienced endodontists/authors (JGP and VMG).
Molars with mesial roots with a minimum length of 12 mm and moderate root canal curvature (at least 25º), and fully formed/closed apices were included. Any molars whose mesial roots exhibited pre-existing canal treatment, cracks, or any other type of structural defect (fractures, pathological resorption, perforations, etc.) were excluded. Through block randomization, the included teeth were divided into four study subgroups (10 specimens each) according to the type of instrument fragment and the level at which it was intentionally located inside the root canal (middle or apical third): (1) SS-Mid (2) SS-Ap (3) NiTi-Mid, and (4) NiTi-Ap. All included molars were conventionally accessed and any remaining pulp tissue was eliminated. Then, patency was established in the mesiobuccal canals with a size 10 K-file (Dentsply-Maillefer, Tulsa, OK, USA). The teeth were then subjected to a disinfection process with 5.25% NaOCl, distilled water, and 17% EDTA, followed by drying and sterilization in a high-pressure steam autoclave.
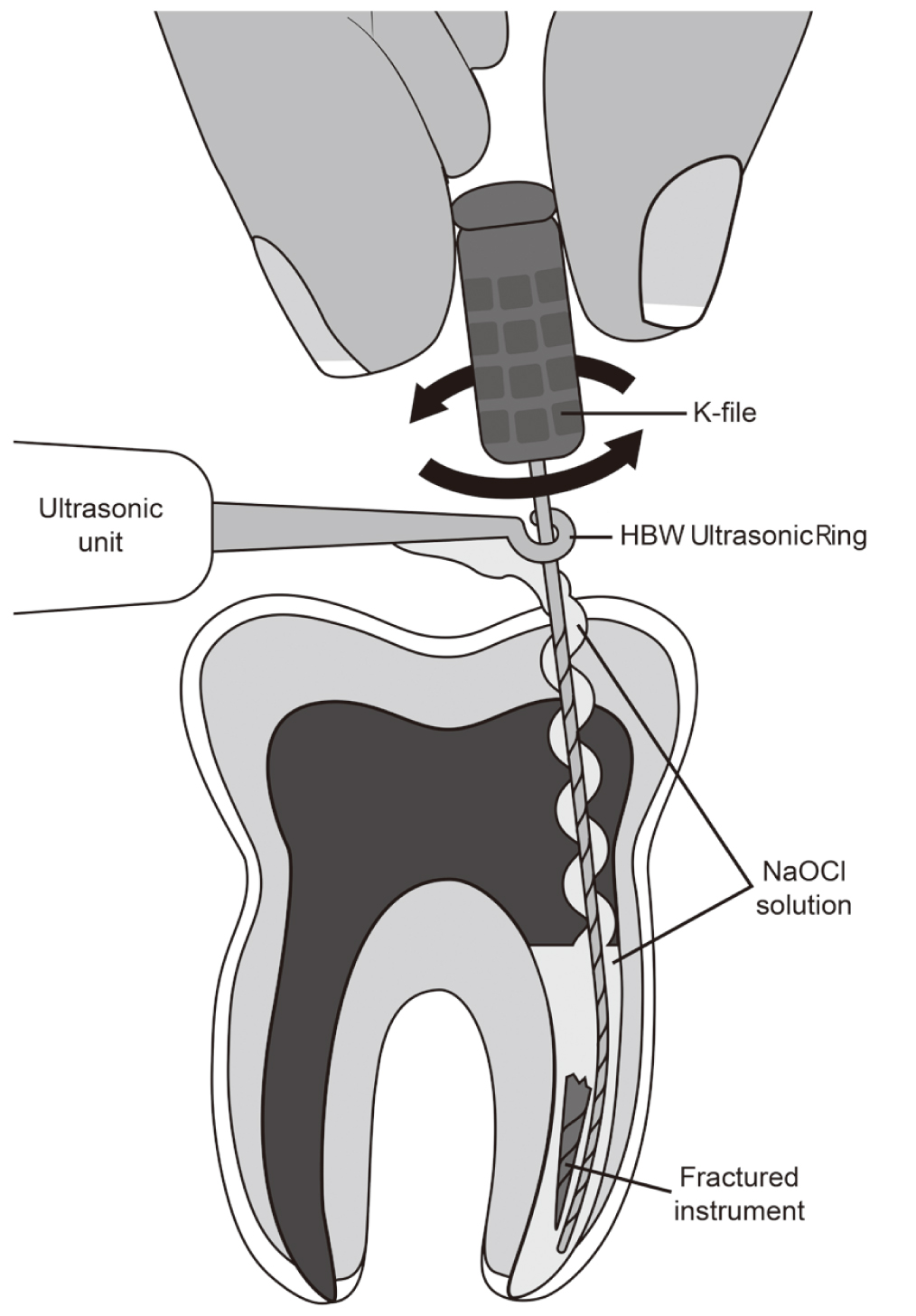
To facilitate the experimental procedures, the teeth were placed on a special iron platform, mounted in silicone. The canal instrumentation was carried out using either K-files (up to #20) or rotary NiTi instruments (Protaper Gold SX, S1, S2, and F1. Dentsply-Maillefer), with profuse 1% NaOCl irrigation between sessions. Intentional instrument separation was achieved by notching the K file SS #25 or the Ni-Ti file Protaper gold F2, respectively, with a high-speed handpiece to a depth of half the file thickness, at a point 4 mm from its tip. Then, the files were manually reintroduced into the canal and through an X-Smart Plus low-speed motor. Control of the level of instrument separation inside the canal, middle or apical third, was achieved by varying the amount of apical pressure, speed of rotation, and torque. Recovery of the separated instrument part was carried out as follows. The lodged instrument was bypassed through the surrounding dentin to create a space and enlarge the canal to the level of the obstruction. For this purpose, an #8 K Mani file was used and, if necessary, #10 and #15 K Mani files were also applied. The files were activated ultrasonically by the HBW Ultrasonic Ring, which is a stainless-steel device connected to an ultrasound unit (NSK Varios 370. NSK Latin America, México City, México). The power setting was low (28 kHz), and profuse irrigation with 1% NaOCl was applied. To perform the bypass, clockwise and counterclockwise movements of the #8 K Mani file were performed until the file achieved the working length. After this, a radiograph was obtained to confirm the bypass. Then, entry and exit movements of HBW Ultrasonic Ring-activated K file #8, 10, or 15 were performed until the fragment became loose and then was completely removed and retrieved (Fig. 1). The average time required to complete the process was around 45 min. After retrieval of the fragment, the tooth was radiographed in order to confirm complete removal of the fragments and to record possible perforations or transportations in the treated root canal (Fig. 2).
Data analysis included descriptive statistics (frequencies and percentages). For comparative analysis, chi-squared of independence and Fisher’s exact tests were performed. Phi/Cramer’s V tests for nominal data were also carried out to assess the strength of association between both independent and dependent variables (values: 0.1 = low association, 0.3 = moderate association, and 0.5 = high association). SPSS v.23 software (IBM SPSS Statistics for Windows, Armonk, NY, USA) was used, with a 0.05 level of significance.
Results
In both of the SS file subgroups (third and apical levels), all of the 20 separated instrument parts were retrieved with an overall success rate of 100%. In the NiTi subgroups, two fragments in the apical third and one in the middle third could not be recovered, corresponding to an overall success rate of 85% (20% and 10% failure rate per subgroup, respectively). The first unsuccesful fragment recovery (NiTi-Mid) was due to the fact it proved impossible to perform the bypass as radiography suggested the NiTi file was deeply screwed. The second event (NiTi-Ap) was due to secondary fracture of the K SS #8 bypass file. The third event (also in the NiTi-Ap subgroup) was because the file had perforated the root apex laterally at the time of its separation, so its recovery was not intended. In both groups there were no cases of fragment transportation beyond the apex during the file removal process. Furthermore, the success rates were compared using intra- and inter-study group approaches according to the type of instrument used and the fragment location. These comparative results are fully described in Table 1.
Table 1
Comparison of intra- and intergroup success rates for recovery of separated instrument fragments
|
Retrieved fragments
(frequency and %) |
P-value
(X2 and FE tests) |
Phi/Cramer’s
V value |
| Intragroup comparisons |
|
|
|
| SS-Mid vs. SS-Ap |
10 (100%)/10 (100%) |
1.0 |
0.026 |
| NiTi-Mid vs. NiTi-Ap |
8 (80%)/9 (90%)
9 (90%)/8 (80%) |
0.531 |
0.140 |
| Intergroup comparisons |
|
|
|
| SS-Mid vs. NiTi-Mid |
10 (100%)/8 (80%)
10 (100%)/9 (90%) |
0.305 |
0.229 |
| SS-Ap vs. NiTi-Ap |
10 (100%)/9 (90%)
10 (100%)/8 (80%) |
(0.474) |
0.333 |
X2, Chi-squared forindependence; FE, Fisher’s exact test
Discussion
In current endodontic practice, management of an intra-canal instrument part or fragment is a challenging clinical procedure, and no consensus has yet been reached on the optimal approach [4]. In such cases, removal of the part or fragment from the canal is considered preferable to leaving it in situ. Only after removal of the fragment can the root canal be optimally cleaned and shaped [5]. Several factors must be carefully considered when deciding how to deal with fractured/separated instrument parts blocking the root canal [8]. If removal is attempted, the probability of success should be balanced against any potential risk or complications.
The present study outcomes suggested that the HBW Ultrasonic Ring technique/ultrasonic tip system is highly successful for removal of SS and NiTi files lodged in the middle and apical thirds of curved root canals. However, as is the case with other ultrasonic techniques, the file removal procedure results in loss of some root dentin, in order to achieve straight-line access, enhance visualization, and loosen the fragment; this increases the risk of tooth fracture [5,9]. Clinicians should also consider that even after a fragment has been removed from the canal wall, further instrumentation may compromise the integrity of the tooth and increase the risk of damage to the root [5]. When an attempt is made to remove an instrument part from the root canal, a full understanding of the management options and related complications, such as potential loss of dentin tissue, should be judiciously considered. Various in vivo and in vitro studies have assessed the success rate of ultrasonic techniques for removal of fractured instrument parts. The majority of those studies advocated the use of ultrasonic tips over other systems, as they require less loss of dentin structure [5]. Pruthi et al. [5] compared the effectiveness of two systems – ultrasonic tips versus the Terauchi system – for removal of separated instrument parts in 80 extracted first permanent mandibular molars. The overall success rates were 90% and 95% respectively, but the mean time required for removal was shorter for the Terauchi system. On the basis of these reports, it can be concluded that the results of the present in vitro study, where the success rates for retrieval of file fragments ranged between 80% and 100%, are roughly equivalent.
First permanent mandibular molars were chosen for the present experimental study as they are associated with a high frequency of instrument fracture [8]. Furthermore, they have thin, narrow, curved root canals that are prone to iatrogenic damage even during conventional canal preparation [8,10]. It has been reported that dentin thickness in the mesial root of first mandibular molars averages around 1 mm in non-instrumented canals [10]. Therefore, there is an increased risk of root perforation. Close inspection of preoperative radiographs and knowledge of root anatomy is crucial before deciding on the file removal procedure, to minimize any damage to the surrounding dentin and the risk of perforation [8].
Future well-conducted randomized and controlled clinical trials will be necessary in order to confirm these findings. A recent systematic review and meta-analysis concluded that such methodological designs are required in endodontics investigations to broaden the limited evidence available for either maintaining or changing current clinical management of separated instrument fragments within the root canal.
In conclusion, the results of the present study indicate that the HBW Ultrasonic Ring is effective overall for the removal and recovery of separated/fractured endodontic instruments in the pulp canal without the need to perform a staging platform with modified Gates-Glidden burs or some other canal-opening instrument, thus avoiding any unnecessary removal of dentin tissue.
Acknowledgments
The authors want to thank Ms. Ilse Garrocho-Cortés for her valuable help in the writing of the present paper.
Conflicts of Interest
The authors have no conflicts of interest to declare in relation to this study.
References
- 1. Alfouzan K, Jamieh A (2018) Fracture of nickel titanium rotary instrument during root canal treatment and re-treatment. A 5-year retrospective study. Int Endod J 51, 157-163.
- 2. McGuigan MB, Louca C, Duncan HF (2013) Endodontic instrument fracture: causes and prevention. Br Dent J 214, 341-348.
- 3. Madarati AA, Hunter MJ, Dummer PM (2013) Management of intracanal separated instruments. J Endod 39, 569-581.
- 4. Fu M, Zhang Z, Hou B (2011) Removal of broken files from root canals by using ultrasonic techniques combined with dental microscope: a retrospective analysis of treatment outcome. J Endod 37, 619-622.
- 5. Pruthi PJ, Nawal RR, Talwar S, Verma M (2020) Comparative evaluation of the effectiveness of ultrasonic tips versus the Terauchi file retrieval kit for the removal of separated endodontic instruments. Restor Dent Endod 45, e14.
- 6. Galván-Pacheco J, Vitales-Noyola M, González-Amaro AM, Bujanda-Wong H, Aragon-Piña A, Mendez-González V, Pozos-Guillén A (2020) Evaluation of in vitro biofilm elimination of Enterococcus faecalis using a continuous ultrasonic irrigation device. J Oral Sci 62, 415-419.
- 7. Zhong B (2009) How to calculate sample size in randomized controlled trials? J Thorac Dis 1, 51-54.
- 8. Souter NJ, Messer HH (2005) Complications associated with fractured file removal using an ultrasonic technique. J Endod 31, 450-452.
- 9. Nevares G, Cunha RS, Zuolo ML, Bueno CE (2012) Success rates for removing or bypassing fractured instruments: a prospective clinical study. J Endod 38, 442-444.
- 10. Isom TL, Marshall JG, Baumgartner JC (1995) Evaluation of root thickness in curved canals after flaring. J Endod 21, 368-371.