Objective: To investigate the clinical results of lateral access corpectomy combined with release of anterior longitudinal ligament deep layer (LACADR) for kyphotic deformity after osteoporotic vertebral fractures (KOVF).
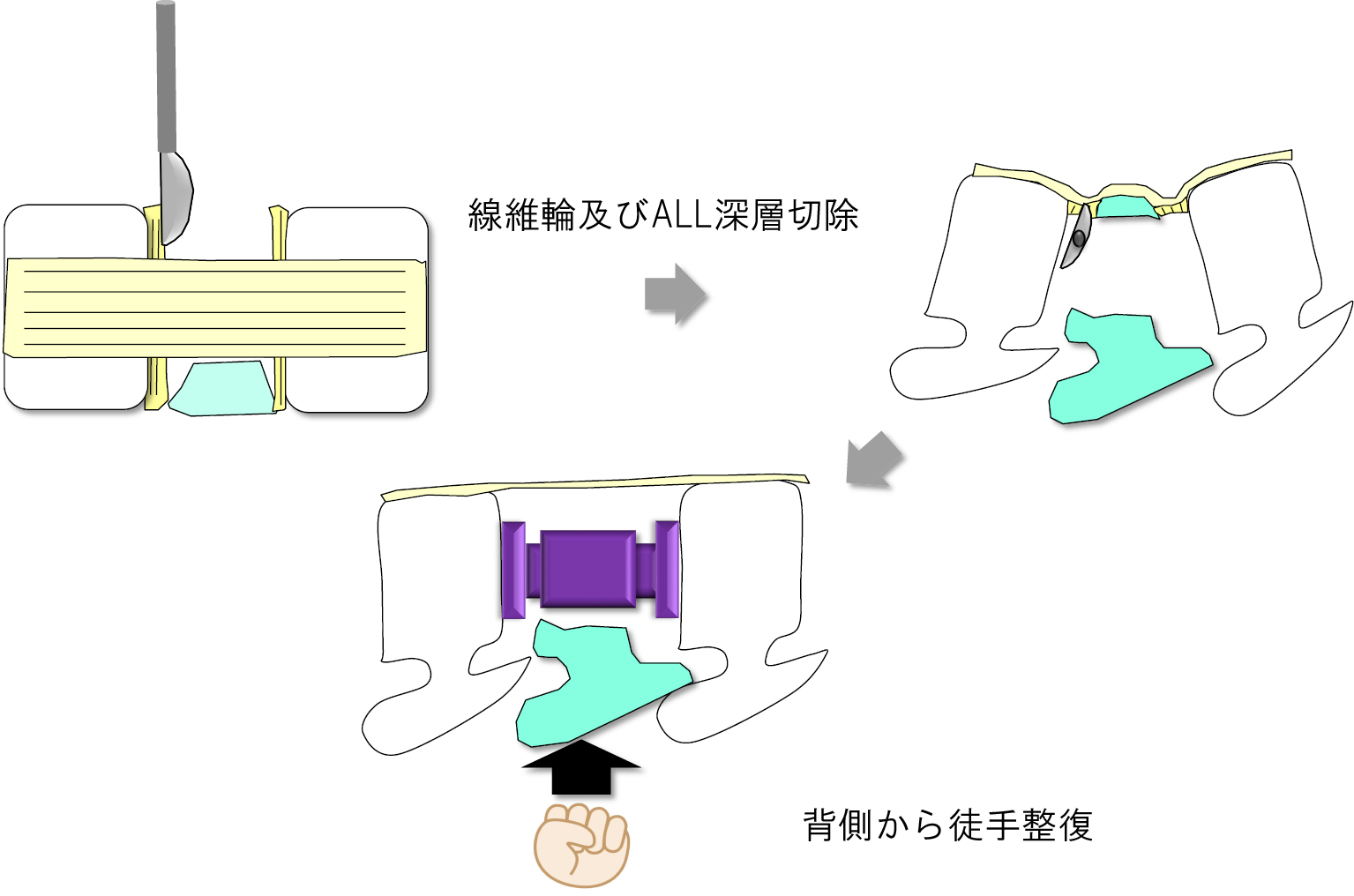
Subjects and methods: KOVF who underwent surgery using LACADR, lateral lumbar interbody fusion (LLIF), and percutaneous pedicle screw (PPS) at our hospital and was able to follow up for more than 2 years. The subjects were 12 patients with the mean age was 74.6±10.1 years, and the mean follow-up period was 47.1±10.1 months. Fractured vertebral body, blood loss and operative time, low back pain VAS, anterior interbody distance (AID) and posterior interbody distance (PID), spinal canal occupancy rate of bone fragment (ORBF), local kyphosis angle (LK), Various spinopelvic parameters, bone fusion rate, and complications were investigated. The surgical procedure is to perform LACADR and vertebral body replacement using an extreme lateral interbody fusion (XLIF®) retractor in the lateral decubitus position, then place the patient in the prone position and perform posterior fusion using PPS. Regarding LACADR, the annulus ligament and the deep layer of ALL on either craniocaudal side of the fractured vertebral body are bluntly dissected with a hump, manual reduction is performed from the dorsal side, and the X-core® is installed while maintaining that state.
Results: The fractured vertebral body was T11 in 1 case, T12 in 10 cases, L1 in 4 cases, and L2 in 1 cases. Bleeding volume was 365±150 ml, operation time was 207±92 minutes, AID improved from 19.5±5.0 mm preoperatively to final 35.5±5.9 mm, and PID improved from 25.0±3.3 mm preoperatively to final 35.1±4.5 mm. ORBF was 44.3±13.1% before surgery, 34.6±10.4% immediately after surgery, and 29.3±8.9% at the end, showing significant improvement. LK was 37.4±4.5° before surgery, 3.6±2.3° after LACADR, 3.9±2.2° after PPS, and 4.6±3.7° at the end, and was significantly improved after surgery. In spinopelvic parameters, SVA was 56.7±48.5 mm preoperatively, 33.0±26.2 mm postoperatively, final 38.0±28.1 mm (pre. vs post. p< 0.05), TK was 44.3±14.5 mm preoperatively, 32.6±12.1°postoperatively, final 35.6±18.3° (preop. vs post. p< 0.05), LLL was 28.2±19.2° preoperatively, 22.3±17.2°postoperatively, final 23.8±18.3° (preop. vs postop. p< 0.05). LL was 34.1±24.0° preoperatively, 36.1±9.4° postoperatively, and final 35.1±11.4° (preop. vs. postop. p=0.37), and no significant improvement was observed. The bone fusion rate was 85% at 12 months, and 92% at the end. As for the morphology of bone fusion, 83% were bridging type or both bridging and interbody fusion type, and 17% were intra-cage fusion type. Complications included intraoperative endplate injury in 1 case, cage subsidence in 2 cases, proximal junctional kyphosis in 1 case, and parietal pleural injury in 4 cases.
Conclusion: The radiographical results of LACADR for KOVF was investigated. Sufficient correction and indirect decompression effects and bone fusion were confirmed.