Abstract
The year 2020 will be remembered for the coronavirus disease 2019 (COVID-19) pandemic,
which continues to affect the whole world. Early and accurate identification of severe
acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is fundamental to combat the
disease. Among the current diagnostic tests, real-time reverse transcriptase–polymerase
chain reaction (RT-qPCR) is the most reliable and frequently used method. Herein, we
discuss the interpretation of RT-qPCR results relative to viral infectivity. Although
nasopharyngeal swab samples are often used for RT-qPCR testing, they require collection by
trained medical staff. Saliva samples are emerging as an inexpensive and efficient
alternative for large-scale screening. Pooled-sample testing of saliva has been applied
for mass screening of SARS-CoV-2 infection. Current policies recommend isolating people
with borderline cycle threshold (Ct) values (35<Ct <40), despite these Ct values
indicating minimal infection risk. We propose the new concept of a “social cut-off” Ct
value and risk stratification based on the correlation of Ct with infectivity. We also
describe the experience of RT-qPCR screening of saliva samples at our institution. It is
important to implement a scientific approach to minimize viral transmission while allowing
economic and social activities to continue.
Introduction
The unprecedented turmoil caused by the coronavirus disease 2019 (COVID-19) pandemic
continues worldwide, although the rapid development of vaccines1 has started to give hope for recovering normalcy in the near
future. Globally, as of December 31, 2020, over 83.8 million people were infected, and
approximately 1.8 million people died from this disease.2 In trying to curb the surge of infections, countries around the world
have imposed social restriction measures, such as limiting travel, closing businesses and
schools, banning large group events, and mandatory quarantines. The resultant impact on
people’s lives has been enormous, including unemployment, worsened food insecurity,
increased incidents of domestic violence, and diverse effects on social and individual
psychological well-being.3,4,5 To alleviate
social and economic damage while prioritizing public health, it is imperative to detect
infection early and minimize further spread of the virus.
COVID-19 Pandemic in Japan and in Tokyo
In Japan, the first case of COVID-19 was reported on January 16, 2020.6 Besides the outbreak on the Diamond
Princess cruise ship in February,7 Japan had its first wave from late March to April, during which a state of
emergency was declared. The Japanese government requested schools and businesses to close,
asked individuals to refrain from traveling and commuting, and encouraged remote learning
and working. The state of emergency was lifted on May 25, 2020, after the number of daily
infections was brought under control. The easing of restrictions resulted in a second wave
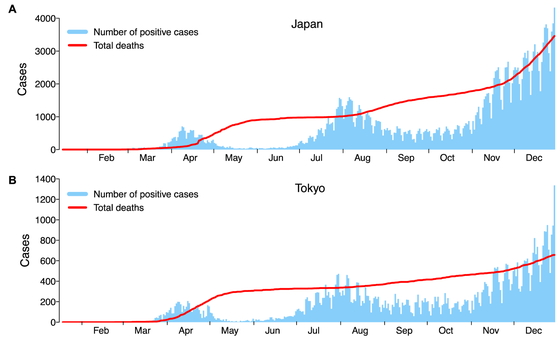
between July and August, which was brought under control in September. At the time this
manuscript was written (December 2020–January 2021), Japan was facing a third wave, during
which the highest number of daily new confirmed and severe cases were reported since the
beginning of the pandemic (Fig. 1A). As of
December 31, 2020, the total number of patients diagnosed with COVID-19 surpassed 230,304,
and 3459 people have died of COVID-19 in Japan.6 Similar to the nationwide trend, Tokyo has had three waves of infections;
it also had the highest number of infections and deaths in the country (Fig. 1B).8
Authorized Assays for the Diagnosis of COVID-19
COVID-19 is caused by infection with the novel severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2). There are two main analytical methods to detect SARS-CoV-2
infection: direct viral detection tests and antibody tests to assess current, recent, or
previous infections.3,9 Direct viral detection tests are able to detect
SARS-CoV-2 nucleic acid or protein antigens using samples from the respiratory system (such
as nasal or oral swabs, or saliva) to indicate infection with SARS-CoV-2. Therefore, direct
viral detection tests are recommended to diagnose acute and current infections in both
symptomatic and asymptomatic individuals to guide contact tracing and determine isolation
measures.
The gold standard method for detecting SARS-CoV-2 viral RNA is real-time reverse
transcriptase–polymerase chain reaction (RT-qPCR).10 To date, different genes within the virus have been used as targets,
including the envelope (E), spike (S), nucleocapsid (N), and open reading frame (ORF)1ab
genes, with the N gene being the most prevalently used.3 Antigen testing is another approach that detects the presence of
SARS-CoV-2 viral antigens. The most commonly used antigens in SARS-CoV-2 antigen tests are
the N and S proteins.3 Although antigen
tests have the benefit of a quick turnaround time (less than 30 min), their sensitivity is
significantly lower than that of RT-qPCR.11,12 In this
context, RT-qPCR techniques have higher sensitivity and specificity than antigen tests do
and, therefore, can minimize the risk of misidentifying patients having the potential to
transmit the virus.13,14,15
While direct viral detection tests can identify acutely infected patients, antibody tests
can be positive during the acute infection and after the resolution of the infection.
Samples for antibody tests are typically collected from the blood. Antibody tests for
SARS-CoV-2 infection are useful tools for surveillance and epidemiologic studies. Recently,
the U.S. Food and Drug Administration (FDA) authorized the first test to detect neutralizing
antibodies that have been shown to decrease in vitro SARS-CoV-2
infection.16 Since COVID-19 is an
emerging infectious disease, it remains to be elucidated whether detecting neutralizing
antibodies in an infected person is associated with protective immunity against this
virus.
Potential Advantage of Saliva Samples for Widespread RT-qPCR Testing
For diagnostic RT-qPCR testing of SARS-CoV-2, samples are obtained from the respiratory
system, such as the nasopharynx, oral cavity, or saliva.10 Although nasopharyngeal swab samples have been most frequently used for
RT-qPCR testing, such samples require collection by trained medical staff, pose infection
risks, and utilize both personnel and personal protective equipment (PPE).17 In contrast, saliva samples can be collected
by non-experts and even allow for self-collection. Several studies have compared matched
nasopharyngeal swabs and saliva samples obtained from patients with PCR-confirmed or
clinically suspected SARS-CoV-2 infection. There was a high concordance observed between the
RT-qPCR cycle threshold (Ct) values of matched nasopharyngeal and saliva samples obtained
early (within 9 days from symptom onset) in the course of the disease.18,19,20,21
Uwamino et al. also assessed the stability of saliva samples and demonstrated that RT-qPCR
Ct values were not affected even after storage at room temperature for more than 7
days.18 Interestingly, the copy number
of SARS-CoV-2 RNA was higher in saliva than that in nasopharyngeal swabs from hospitalized
COVID-19 patients.22 Because SARS-CoV-2
can be detected in the saliva of asymptomatic individuals,20,22 saliva has been proposed as a non-invasive alternative to nasopharyngeal
swabs to facilitate large-scale RT-qPCR screening without posing a risk to healthcare
workers.
Debate Over the Cut-off of RT-PCR for the Diagnosis of COVID-19
In principle, a PCR result is considered “positive” when the Ct value is less than
40.10 However, there has been debate
over the optimal cutoff for the diagnosis of COVID-19 because suggested thresholds vary
between countries and experts.23 For
example, some groups used a cut-off Ct value <38 for the diagnosis of
SARS-CoV-2,22,24 whereas other groups used a lower cut-off
value.25 It is important to note that
Ct value cutoffs are established by manufacturers through evaluation of known positive and
negative samples; consequently, not all RT-qPCR tests use the same Ct cutoff value.
Multiple studies have indicated that RT-qPCR can detect non-viable viral RNA fragments and
viral copy numbers that are lower than those observed during infection.26,27 Using a cut-off Ct value <40 might misidentify individuals
who are not infectious and lead to unnecessary isolation. To maintain social and economic
activities while preventing the spread of infection, it is crucial to have guidelines that
are reasonable and realistic.
Several groups have examined the correlation between RT-qPCR Ct values and
infectivity,26,28,29,30,31
suggesting that much lower Ct values could be used for practical quarantine control methods.
For example, a group from France performed serial RT-qPCR testing and compared Ct values
with infectivity in a cell culture model using nasopharyngeal samples from 155
RT-qPCR-confirmed COVID-19 patients.26 The
authors demonstrated that the success rate of viral culture decreased progressively as Ct
values increased. They also observed that the virus was not isolated from samples collected
later in the course of disease (8 days after symptom onset), whereas viral RNA was still
detected by RT-qPCR. They concluded that patients with Ct values of at least 34 no longer
pose a threat of viral transmission.26
Another study from Canada that examined the correlation between RT-qPCR Ct values and virus
isolation in cell culture showed that infectivity (as defined by growth in cell culture) is
dependent on both Ct values (less than 24) and the stage of the disease (less than 8 days
from symptom onset).28 A strong
relationship between Ct values and virus isolation has also been reported by a study group
in the U.K. The authors showed that there was no statistically significant difference in Ct
values between those with asymptomatic, mild–moderate, and severe symptoms, and that samples
from asymptomatic and symptomatic patients exhibited similar virus isolation results, based
on the Ct values and time points in their disease course.29 Another study from the U.S. showed that virus growth in cell
culture was highly efficient in samples with Ct values of 10–20 (76.7% positive isolation
rate), and dropped to 24.1% for Ct values of 20–30 and to 2.9% for Ct values of 30–40. There
was one outlier case of positive viral culture in a sample with a Ct value above 30 (Ct
=32.1), but the rest of the 47 culture-positive samples had Ct values lower than 30, with a
mean Ct value of 18.8.31 Further,
Yamayoshi et al. reported that no virus isolation was observed in samples with Ct values
higher than 30.14
Although there are variabilities of Ct value thresholds for viral infectivity in cell
culture models, with Ct values of 34, 30, and 24 being indicated, the common takeaway
interpretation from these studies is that the viral load at the end of the RT-qPCR cycle
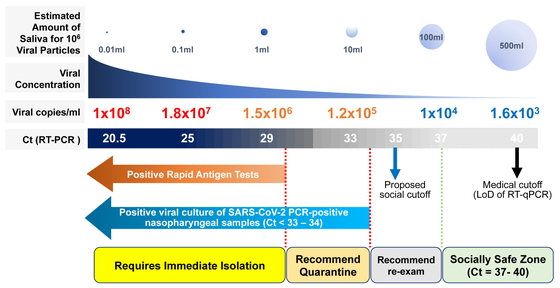
(>34 Ct) may not reflect virus replication capacity. When we applied the formula
(10^((Ct–43.023)/–3.718))*75*(1000/300) as previously described,22 a Ct value of 34 indicates 1 × 106 viral particles
in 10 mL of nasopharyngeal or saliva samples (Fig.
2). Given that normal social activity does not involve exchanging such amounts of
saliva or nasal discharge, the risk of transmission is very low. However, the amount of
virus needed for person-to-person transmission of SARS-CoV-2 is still unknown.
Recommendation on risk stratification
From the findings above, we propose using the RT-qPCR Ct values to stratify the risk of
viral transmission as follows (Fig. 2):
– Patients with Ct values <30 are considered highly infectious, requiring immediate
isolation and contact tracing. The tested individual should be reported to the local
health center and should seek advice on medical treatment.
– Patients with Ct values between 30 and 34 are considered moderately infectious. The
tested individual should refrain from social gatherings and quarantine themselves.
– Patients with Ct values between 34 and 37 are considered as belonging to a “gray zone,”
allowing the tested individual to continue social activity but with adequate standard
precautions33 (such as hand hygiene,
PPE, respiratory etiquette, cleaning, and disinfection), physical distancing, and contact
tracing. As implied by the word “gray,” individuals are recommended to have a follow-up
test within the next few days and to closely monitor themselves for symptoms. We propose
the new concept of a “social cut-off” at a Ct value <35, based on studies showing the
correlation between Ct values and viral culture recovery rate.26,29,31
– Patients with Ct values >37 are considered non-infectious, allowing the tested
individual to continue social activity with standard precautions.33 One must keep in mind that a Ct >37 (a
“negative test”) does not completely rule out the presence of the virus, because there is
a risk of early infection with low viral load. Decisions on social activity levels for a
tested individual should be based not only on the Ct values but also on the combination of
clinical observation and patient history, including recent exposure. It would be safer to
follow up these individuals, especially those in high-risk environments such as hospitals,
nursing homes, and schools to prevent unaddressed cluster outbreaks.
Rapid qualitative antigen testing has been widely implemented because it is easy, quick,
and inexpensive. In general, rapid antigen tests detect patients whose RT-qPCR Ct values
are below 30.13,14,34 When RT-qPCR is not easily accessible, rapid antigen testing
should be considered. Individuals with a positive antigen test result must be advised to
immediately isolate themselves and should be provided with medical care if they develop
any symptoms.
Limitations of diagnosing COVID-19 using RT-qPCR
The RT-qPCR method has several limitations. First, a test may return a false-negative
result,35 as experienced with other
test modalities. To ensure both a safe and active society during a pandemic, it would be
ideal to follow up individuals who were exposed to the virus or have suspicious symptoms
and to encourage routine testing rather than snapshot, one-time testing. Second, different
probes and primer targets result in different amplification efficiencies and Ct
values.36,37 It is known that PCR amplification
efficiencies critically influence the Ct values; for example, the number of viral genome
copies estimated by a Ct value of 37 in PCR with an amplification efficiency of 100% is
equal to that estimated by a Ct value of about 40 in PCR with an amplification efficiency
of 90%. Each local laboratory in charge of diagnostic RT-qPCR testing should be aware of
these differences when optimizing standard operating procedures and of the importance of
regular laboratory quality checks and controls. Third, RT-qPCR can result in
cross-contamination, sample carry-over, and false-positive results.38,39 Steps for monitoring and reducing contamination have been
proposed.39 Regular quality
measurements are essential when using RT-qPCR results for risk stratification. Fourth,
mutations in the viral genome may compromise the sensitivity of RT-qPCR testing to detect
SARS-CoV-2, as has been demonstrated in some reports.40,41
Consequently, it is critical to monitor the genetic evolution of this virus for the
emergence of mutations that might negatively affect the accuracy of RT-qPCR-based
diagnosis and to use more than two regions as targets to avoid false-negative results.
Comparing the sensitivity and specificity of several commercially available PCR kits for
detecting variants prevalent in each region will also minimize the risk of false-negative
results. Finally, a new variant identified in the U.K. that is spreading across several
other countries has renewed worldwide concern because it has been revealed to be more
virulent than previous circulating viruses.42,43 If this
lineage (known as B.1.1.7 and characterized by a range of 14 non-synonymous mutations and
3 deletions) becomes the dominant strain in the region, the social cut-off proposed here
may have to be adjusted.
Sample Pooling for SARS-CoV-2 RT-qPCR
The effectiveness of sample pooling for RT-qPCR has been validated for other infectious
diseases, including syphilis, malaria, HIV, and influenza.44,45 With the rising demand for large-scale testing for SARS-CoV-2, especially
for screening purposes, pooled-sample testing offers a promising strategy to enable
large-scale screening and save supplies, time, and human resources.45 Sample pooling is performed by mixing
different samples and performing the test on this “pool” as if it were a single sample. If
the result is negative, each sample in the pool is considered negative and no further
individual testing is required. If the pool tests positive, then individual testing is
required. Therefore, pooled sample testing can increase the testing capacity.45 Multiple groups have evaluated the
effectiveness and accuracy of sample pooling strategies for detecting SARS-CoV-2. When
considering the sensitivity and specificity of the test results, the optimal pool size (the
number of samples in a pool) varies depending on the prevalence or positivity rate in the
community. For example, a pool size of around 30 has been shown to be effective in
low-prevalence areas.44 The dilution of
samples in pooled testing results in increased Ct values for each viral target
gene.46,47 For instance, pooling at a dilution of 1:10
led to a median loss of Ct values of 2.87 for the E gene, 3.36 for the RNA-dependent RNA
polymerase gene, and 2.99 for the N gene.47 When conducting sample pooling, one must keep in mind that borderline
positive samples may escape detection and return false-negative results. To adjust for this,
a possible solution may be to add a few cycles to the threshold to minimize the chances of
missing otherwise positive cases. The studies mentioned above assessed pooled sample testing
using nasopharyngeal swab samples. Other studies have demonstrated the usefulness of pooled
sample testing for evaluating saliva samples.48,49,50 Because
the demand for screening large numbers of people is increasing, we have started comparing
the sensitivities of pooled-sample testing and individual testing at Keio University. The
results of the pooled-sample testing are beyond the scope of this paper, and the results we
describe in the following section were obtained from individual RT-qPCR testing.
Keio University Cases
Keio University School of Medicine has been supporting Keio University Hospital by
undertaking non-urgent COVID-19 screening testing, i.e., testing healthy and asymptomatic
individuals who attended medical check-ups. This preserved the hospital’s capacity to test
symptomatic patients and suspected individuals, to follow up patients already diagnosed, and
to screen patients scheduled for treatment at the hospital. To achieve this, the
Collaborative Research Resources, located within the medical school building, was registered
by the Shinjuku City Public Health Center as an external clinical laboratory (ECL) to be an
auxiliary COVID-19 PCR testing site in Tokyo in early May 2020. The ECL began to function in
late August. At the end of December 2020, we had tested 2342 samples by RT-qPCR. Briefly,
participants collected their own saliva samples at home in sterile cups and brought them
within 1–2 days to the Center for Preventive Medicine at Keio University Hospital. After
thermal inactivation of the virus and RNA extraction, RT-qPCR was performed according to the
manufacturer’s instructions using the QuantStudio 5 Real-Time PCR system (Thermo Scientific,
Waltham, MA, USA) and the SARS-CoV-2 Direct Detection RT-qPCR Kit (TaKaRa Bio, Shiga,
Japan), which contains a primer/probe mix for the U.S. CDC 2019-nCoV_N1 and 2019-nCoV_N2
strains.51 We determined that samples
with Ct values <40 with either primer were positive for SARS-CoV-2 infection. All
procedures followed were in accordance with the ethical standards of the responsible
committee at which this study was conducted (IRB approval number 20200063) and with the
Helsinki Declaration of 1964 and later versions. Written informed consent was obtained from
all patients and healthy individuals prior to data collection.
We had no positive cases in August, September, or October among the healthy and
asymptomatic individuals who visited the Center for Preventive Medicine. During the third
wave in Tokyo, we reported three asymptomatic cases in November. However, no positive cases
were reported in December. The number of RT-qPCR tests performed on individuals visiting for
medical check-ups at the Center for Preventive Medicine and the clinical characteristics of
the three RT-qPCR-positive cases are shown in Tables
1 and 2.
Table 1.
SARS-CoV-2 RT-qPCR tests performed on individuals visiting for medical check-ups at
the Center for Preventive Medicine in 2020
| Month |
PCR tests |
Positive Cases |
| August |
162 |
0 |
| September |
526 |
0 |
| October |
617 |
0 |
| November |
542 |
3 |
| December |
495 |
0 |
aPCR screening started on August 24, which explains the smaller number of
samples tested in August compared with that in other months.
Table 2.
Clinical characteristics of three RT-qPCR-positive cases confirmed at the Center
for Preventive Medicine
| Case |
Age (years) |
Sex |
Ct value of RT-qPCR |
Prior exposure |
| Case 1 |
49 |
Male |
29.0 |
7 days before |
| Case 2 |
54 |
Male |
34.8 |
Unknown |
| Case 3 |
45 |
Female |
26.3 |
Unknown |
Ct, cycle threshold.
Dental treatment can be high risk in terms of possible transmission of the virus because
patients and healthcare providers are in close proximity and procedures can generate
aerosols from patient saliva that may be mixed with blood. Aerosols can directly splash into
the dentist/hygienist’s eyes or contaminate surfaces in the clinic.52 As a part of risk management efforts to
provide a safe environment for dental care at Keio University Hospital, the ECL has been
screening outpatients at the Department of Dentistry and Oral Surgery at Keio University
Hospital who are scheduled to undergo treatment. From August to December, we tested 208
patients, and none had positive results.
Conclusions
The COVID-19 pandemic has affected countries worldwide and continues to have serious
effects on public health and the economy. Rapid and accurate detection of infection is key
to preventing transmission. Herein, we discussed the characteristics of the test modalities
currently used to detect SARS-CoV-2. RT-qPCR is a highly sensitive and useful method for
detecting ongoing infections, although it has limitations. Saliva samples are a good
alternative to nasopharyngeal swabs, offering similar sensitivity and sample stability and
saving human resources and PPE. Pooled-sample testing has proven effective in detecting
SARS-CoV-2 infection in a large-scale setup, although we must keep in mind that borderline
positive samples may escape detection in pools. We propose the new concept of “social
cut-off” Ct values and risk stratification based on studies evaluating the correlation
between Ct values and infectivity as a guide to safe levels of social activity with less
stringent restrictions. Balanced ways of supporting public health and social and economic
activities must be explored using a science-based approach.
Author Contributions
H.N. conceived the study, and J.O. and H.T. wrote, revised, and edited the manuscript. M.S.
and R.T. conducted RT-qPCR testing. S.M. and T.N. collected the samples from outpatients at
the Department of Dentistry and Oral Surgery. H.T. collected samples from healthy and
asymptomatic individuals who visited the Center for Preventive Medicine for medical
check-ups. H.S. and K.M. provided resources for conducting RT-qPCR screening tests at the
ECL facility. All authors have read and approved the manuscript.
Acknowledgments
The authors would like to thank Ms. Kaori Mochida, Ms. Emmy Yanagida, Mr. Hiroshi Yamada,
Mr. Hiroumi Kurogi, and Ms. Matsumi Hirose for their technical assistance; Dr. Scott E.
Woodman (Houston, TX, USA) for proofreading our manuscript; and Dr. A. Gordon Robertson
(Courtenay, BC, Canada) for his helpful advice on data visualization and valuable manuscript
discussions. The Keio Donner Project was launched in early 2020 to promote research to
clarify the mechanism of COVID-19 disease, increase diagnostic test capacity, and develop
effective therapeutic options. The name “Donner” is derived from the late Professor S.
Kitasato, the founder of the Keio University School of Medicine. Special thanks to Masatoshi
Wakui, MD, PhD; Yoshifumi Uwamino, MD, PhD; Toshinobu Kurafuji; Masayo Noguchi; Akemi Ohno;
Hiromitsu Yokota, PhD; Haruhito Kikuchi; MD; PhD, Naoki Hasegawa, MD, PhD; Mitsuru Murata,
MD, PhD; Yuko Kitagawa, MD, PhD; and Masayuki Amagai, MD, PhD for their contribution to the
Keio Donner Project. This work was partially supported by the Keio University Global
Research Institute (KGRI) Research Projects for New Coronavirus Crisis: Implementation of a
Keio Model to Optimize SARS-CoV-2 PCR Tests through Systems Approach (PI: Koichi Matsuo);
the Japan Agency for Medical Research and Development (AMED) (PI: Hiroshi Nishihara, Grant
Number 20he1422004j0001); and the Ministry of Education, Culture, Sports, Science and
Technology of Japan (MEXT) for utilization of the university’s PCR equipment. The funding
agencies had no role in the study design; in the collection, analysis, or interpretation of
data; in the writing of the report; or in the decision to submit the article for
publication.
Conflicts of Interest
The authors have declared that no conflict of interest exists.
References
- 1. World Health Organization: Coronavirus disease
(COVID-19) pandemic. Draft landscape of COVID-19 candidate vaccines. Available online:
https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines
(accessed on 12 January 2021).
- 2. Worldometer. Covid-19 Coronavirus Pandemic.
Available online: https://www.worldometers.info/coronavirus/ (accessed on 12 January
2021).
- 3. Nguyen NN, McCarthy C, Lantigua D, Camci-Unal G:
Development of diagnostic tests for detection of SARS-CoV-2. Diagnostics (Basel) 2020; 10:
905. PMID:33167445, DOI:10.3390/diagnostics10110905
- 4. Peng W, Berry EM: Coping with the challenges of
COVID-19 using the sociotype framework: a rehearsal for the next pandemic. Rambam
Maimonides Med J 2020. PMID:33215987
- 5. El Keshky ME, Basyouni SS, Al Sabban AM: Getting
through COVID-19: the pandemic’s impact on the psychology of sustainability, quality of
life, and the global economy − a systematic review. Front Psychol 2020; 11: 585897.
PMID:33281683, DOI:10.3389/fpsyg.2020.585897
- 6. Ministry of Health, Labour and Welfare of Japan:
Novel Coronavirus (COVID-19). Available online:
https://www.mhlw.go.jp/stf/covid-19/open-data_english.html (accessed on 12 January
2021).
- 7. Tsuboi M, Hachiya M, Noda S, Iso H, Umeda T:
Epidemiology and quarantine measures during COVID-19 outbreak on the cruise ship Diamond
Princess docked at Yokohama, Japan in 2020: a descriptive analysis. Glob Health Med 2020;
2: 102–106. PMID:33330785, DOI:10.35772/ghm.2020.01037
- 8. The Tokyo Metropolitan Government: Updates on
COVID-19 in Tokyo. Available online: https://stopcovid19.metro.tokyo.lg.jp/en (accessed on
12 January 2021).
- 9. Sheikhzadeh E, Eissa S, Ismail A, Zourob M:
Diagnostic techniques for COVID-19 and new developments. Talanta 2020; 220: 121392.
PMID:32928412, DOI:10.1016/j.talanta.2020.121392
- 10. Sethuraman N, Jeremiah SS, Ryo A: Interpreting
diagnostic tests for SARS-CoV-2. JAMA 2020; 323: 2249–2251. PMID:32374370,
DOI:10.1001/jama.2020.8259
- 11. Scohy A, Anantharajah A, Bodéus M, Kabamba-Mukadi
B, Verroken A, Rodriguez-Villalobos H: Low performance of rapid antigen detection test as
frontline testing for COVID-19 diagnosis. J Clin Virol 2020; 129: 104455. PMID:32485618,
DOI:10.1016/j.jcv.2020.104455
- 12. Nagura-Ikeda M, Imai K, Tabata S, Miyoshi K,
Murahara N, Mizuno T, Horiuchi M, Kato K, Imoto Y, Iwata M, Mimura S, Ito T, Tamura K,
Kato Y: Clinical evaluation of self-collected saliva by quantitative reverse
transcription-PCR (RT-qPCR), direct RT-qPCR, reverse transcription-loop-mediated
isothermal amplification, and a rapid antigen test to diagnose COVID-19. J Clin Microbiol
2020; 58: e01438-20. PMID:32636214, DOI:10.1128/JCM.01438-20
- 13. Krüttgen A, Cornelissen CG, Dreher M, Hornef MW,
Imöhl M, Kleines M: Comparison of the SARS-CoV-2 Rapid Antigen Test to the real star
Sars-CoV-2 RT PCR kit. J Virol Methods 2021; 288: 114024. PMID:33227341,
DOI:10.1016/j.jviromet.2020.114024
- 14. Yamayoshi S, Sakai-Tagawa Y, Koga M, Akasaka O,
Nakachi I, Koh H, Maeda K, Adachi E, Saito M, Nagai H, Ikeuchi K, Ogura T, Baba R, Fujita
K, Fukui T, Ito F, Hattori S, Yamamoto K, Nakamoto T, Furusawa Y, Yasuhara A, Ujie M,
Yamada S, Ito M, Mitsuya H, Omagari N, Yotsuyanagi H, Iwatsuki-Horimoto K, Imai M, Kawaoka
Y: Comparison of rapid antigen tests for COVID-19. Viruses 2020; 12: 1420. PMID:33322035,
DOI:10.3390/v12121420
- 15. Mak GC, Lau SS, Wong KK, Chow NL, Lau CS, Lam ET,
Chan RC, Tsang DN: Evaluation of rapid antigen detection kit from the WHO Emergency Use
List for detecting SARS-CoV-2. J Clin Virol 2021; 134: 104712. PMID:33338894,
DOI:10.1016/j.jcv.2020.104712
- 16. US Food and Drug Administration (FDA):
Coronavirus (COVID-19) Update: FDA authorizes first test that detects neutralizing
antibodies from recent or prior SARS-CoV-2 infection. Available online:
https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-test-detects-neutralizing-antibodies-recent-or
(accessed on 20 December 2020).
- 17. Qian Y, Zeng T, Wang H, Xu M, Chen J, Hu N, Chen
D, Liu Y: Safety management of nasopharyngeal specimen collection from suspected cases of
coronavirus disease 2019. Int J Nurs Sci 2020; 7: 153–156. PMID:32292635,
DOI:10.1016/j.ijnss.2020.03.012
- 18. Uwamino Y, Nagata M, Aoki W, Fujimori Y, Nakagawa
T, Yokota H, Sakai-Tagawa Y, Iwatsuki-Horimoto K, Shiraki T, Uchida S, Uno S, Kabata H,
Ikemura S, Kamata H, Ishii M, Fukunaga K, Kawaoka Y, Hasegawa N, Murata M: Accuracy and
stability of saliva as a sample for reverse transcription PCR detection of SARS-CoV-2. J
Clin Pathol 2021; 74: 67–68. PMID:32928941,
DOI:10.1136/jclinpath-2020-206972
- 19. Iwasaki S, Fujisawa S, Nakakubo S, Kamada K,
Yamashita Y, Fukumoto T, Sato K, Oguri S, Taki K, Senjo H, Sugita J, Hayasaka K, Konno S,
Nishida M, Teshima T: Comparison of SARS-CoV-2 detection in nasopharyngeal swab and
saliva. J Infect 2020; 81: e145–e147. PMID:32504740,
DOI:10.1016/j.jinf.2020.05.071
- 20. Medeiros da Silva RC, Nogueira Marinho LC, de
Araújo Silva DN, Costa de Lima K, Pirih FQ, Luz de Aquino Martins AR: Saliva as a possible
tool for the SARS-CoV-2 detection: a review. Travel Med Infect Dis 2020; 38: 101920.
PMID:33220456, DOI:10.1016/j.tmaid.2020.101920
- 21. Sakanashi D, Asai N, Nakamura A, Miyazaki N,
Kawamoto Y, Ohno T, Yamada A, Koita I, Suematsu H, Hagihara M, Shiota A, Kurumiya A,
Sakata M, Kato S, Muramatsu Y, Koizumi Y, Kishino T, Ohashi W, Yamagishi Y, Mikamo H:
Comparative evaluation of nasopharyngeal swab and saliva specimens for the molecular
detection of SARS-CoV-2 RNA in Japanese patients with COVID-19. J Infect Chemother 2021;
27: 126–129. PMID:33060046, DOI:10.1016/j.jiac.2020.09.027
- 22. Wyllie AL, Fournier J, Casanovas-Massana A,
Campbell M, Tokuyama M, Vijayakumar P, Warren JL, Geng B, Muenker MC, Moore AJ, Vogels CB,
Petrone ME, Ott IM, Lu P, Venkataraman A, Lu-Culligan A, Klein J, Earnest R, Simonov M,
Datta R, Handoko R, Naushad N, Sewanan LR, Valdez J, White EB, Lapidus S, Kalinich CC,
Jiang X, Kim DJ, Kudo E, Linehan M, Mao T, Moriyama M, Oh JE, Park A, Silva J, Song E,
Takahashi T, Taura M, Weizman OE, Wong P, Yang Y, Bermejo S, Odio CD, Omer SB, Dela Cruz
CS, Farhadian S, Martinello RA, Iwasaki A, Grubaugh ND, Ko AI: Saliva or nasopharyngeal
swab specimens for detection of SARS-CoV-2. N Engl J Med 2020; 383: 1283–1286.
PMID:32857487, DOI:10.1056/NEJMc2016359
- 23. Sule WF, Oluwayelu DO: Real-time RT-PCR for
COVID-19 diagnosis: challenges and prospects. Pan Afr Med J 2020; 35(Suppl 2): 121.
PMID:33282076, DOI:10.11604/pamj.supp.2020.35.2.24258
- 24. Zheng S, Fan J, Yu F, Feng B, Lou B, Zou Q, Xie
G, Lin S, Wang R, Yang X, Chen W, Wang Q, Zhang D, Liu Y, Gong R, Ma Z, Lu S, Xiao Y, Gu
Y, Zhang J, Yao H, Xu K, Lu X, Wei G, Zhou J, Fang Q, Cai H, Qiu Y, Sheng J, Chen Y, Liang
T: Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in
Zhejiang province, China, January-March 2020: retrospective cohort study. BMJ 2020; 369:
m1443. PMID:32317267, DOI:10.1136/bmj.m1443
- 25. Arnaout R, Lee RA, Lee GR, Callahan C, Yen CF,
Smith KP, Arora R, Kirby JE: SARS-CoV-2 testing: the limit of detection matters. bioRχiv
2020. doi:.DOI:10.1101/2020.06.02.131144
- 26. La Scola B, Le Bideau M, Andreani J, Hoang VT,
Grimaldier C, Colson P, Gautret P, Raoult D: Viral RNA load as determined by cell culture
as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards.
Eur J Clin Microbiol Infect Dis 2020; 39: 1059–1061. PMID:32342252,
DOI:10.1007/s10096-020-03913-9
- 27. He X, Lau EH, Wu P, Deng X, Wang J, Hao X, Lau
YC, Wong JY, Guan Y, Tan X, Mo X, Chen Y, Liao B, Chen W, Hu F, Zhang Q, Zhong M, Wu Y,
Zhao L, Zhang F, Cowling BJ, Li F, Leung GM: Temporal dynamics in viral shedding and
transmissibility of COVID-19. Nat Med 2020; 26: 672–675. PMID:32296168,
DOI:10.1038/s41591-020-0869-5
- 28. Bullard J, Dust K, Funk D, Strong JE, Alexander
D, Garnett L, Boodman C, Bello A, Hedley A, Schiffman Z, Doan K, Bastien N, Li Y, Van
Caeseele PG, Poliquin G: Predicting infectious SARS-CoV-2 from diagnostic samples. Clin
Infect Dis 2020; ciaa638. PMID:32442256
- 29. Singanayagam A, Patel M, Charlett A, Lopez Bernal
J, Saliba V, Ellis J, Ladhani S, Zambon M, Gopal R: Duration of infectiousness and
correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to
May 2020. Euro Surveill 2020; 25: 2001483. PMID:32794447,
DOI:10.2807/1560-7917.ES.2020.25.32.2001483
- 30. Walsh KA, Jordan K, Clyne B, Rohde D, Drummond L,
Byrne P, Ahern S, Carty PG, O’Brien KK, O’Murchu E, O’Neill M, Smith SM, Ryan M,
Harrington P: SARS-CoV-2 detection, viral load and infectivity over the course of an
infection. J Infect 2020; 81: 357–371. PMID:32615199,
DOI:10.1016/j.jinf.2020.06.067
- 31.Gniazdowski V, Morris CP, Wohl S, Mehoke T,
Ramakrishnan S, Thielen P, Powell H, Smith B, Armstrong DT, Herrera M, Reifsnyder C,
Sevdali M, Carroll KC, Pekosz A, Mostafa HH: Repeat COVID-19 molecular testing:
correlation of SARS-CoV-2 culture with molecular assays and cycle thresholds. Clin Infect
Dis 2020; 27 : ciaa1616. https://doi.org/10.1093/cid/ciaa1616
- 32. Wang X, Yao H, Xu X, Zhang P, Zhang M, Shao J,
Xiao Y, Wang H: Limits of detection of 6 approved RT-PCR kits for the novel
SARS-coronavirus-2 (SARS-CoV-2). Clin Chem 2020; 66: 977–979. PMID:32282874,
DOI:10.1093/clinchem/hvaa099
- 33. Siegel JD, Rhinehart E, Jackson M, Chiarello L,
Health Care Infection Control Practices Advisory Committee: 2007 Guideline for isolation
precautions: preventing transmission of infectious agents in health care settings. Am J
Infect Control 2007; 35(Suppl 2): S65–S164. PMID:18068815,
DOI:10.1016/j.ajic.2007.10.007
- 34. Lanser L, Bellmann-Weiler R, Öttl KW, Huber L,
Griesmacher A, Theurl I, Weiss G: Evaluating the clinical utility and sensitivity of
SARS-CoV-2 antigen testing in relation to RT-PCR Ct values. Infection 2020; 13: 1–3.
PMID:33185807
- 35. Arevalo-Rodriguez I, Buitrago-Garcia D,
Simancas-Racines D, Zambrano-Achig P, Del Campo R, Ciapponi A, Sued O, Martinez-García L,
Rutjes AW, Low N, Bossuyt PM, Perez-Molina JA, Zamora J: False-negative results of initial
RT-PCR assays for COVID-19: a systematic review. PLoS One 2020; 15: e0242958.
PMID:33301459, DOI:10.1371/journal.pone.0242958
- 36. Vogels CB, Brito AF, Wyllie AL, Fauver JR, Ott
IM, Kalinich CC, Petrone ME, Casanovas-Massana A, Muenker CM, Moore AJ, Klein J, Lu P,
Lu-Culligan A, Jiang X, Kim DJ, Kudo E, Mao T, Moriyama M, Oh JE, Park A, Silva J, Song E,
Takahashi T, Taura M, Tokuyama M, Venkataraman A, Weizman OE, Wong P, Yang Y, Cheemarla
NR, White EB, Lapidus S, Earnest R, Geng B, Vijayakumar P, Odio C, Fournier J, Bermejo S,
Farhadian S, Dela Cruz CS, Iwasaki A, Ko AI, Landry ML, Foxman EF, Grubaugh ND: Analytical
sensitivity and efficiency comparisons of SARS-CoV-2 RT-qPCR primer–probe sets. Nat
Microbiol 2020; 5: 1299–1305. PMID:32651556,
DOI:10.1038/s41564-020-0761-6
- 37. Zhou Y, Pei F, Ji M, Wang L, Zhao H, Li H, Yang
W, Wang Q, Zhao Q, Wang Y: Sensitivity evaluation of 2019 novel coronavirus (SARS-CoV-2)
RT-PCR detection kits and strategy to reduce false negative. PLoS One 2020; 15: e0241469.
PMID:33206690, DOI:10.1371/journal.pone.0241469
- 38. Wernike K, Keller M, Conraths FJ, Mettenleiter
TC, Groschup MH, Beer M: Pitfalls in SARS‐CoV‐2 PCR diagnostics. Transbound Emerg Dis
2020; tbed.13684. PMID:32536002, DOI:10.1111/tbed.13684
- 39. Huggett JF, Benes V, Bustin SA, Garson JA, Harris
K, Kammel M, Kubista M, McHugh TD, Moran-Gilad J, Nolan T, Pfaffl MW, Salit M, Shipley G,
Vallone PM, Vandesompele J, Wittwer C, Zeichhardt H: Cautionary note on contamination of
reagents used for molecular detection of SARS-CoV-2. Clin Chem 2020; 66: 1369–1372.
PMID:32894756, DOI:10.1093/clinchem/hvaa214
- 40. Artesi M, Bontems S, Göbbels P, Franckh M, Maes
P, Boreux R, Meex C, Melin P, Hayette MP, Bours V, Durkin K: A recurrent mutation at
position 26340 of SARS-CoV-2 is associated with failure of the E gene quantitative reverse
transcription-PCR utilized in a commercial dual-target diagnostic assay. J Clin Microbiol
2020; 58: e01598-20. PMID:32690547, DOI:10.1128/JCM.01598-20
- 41. Ziegler K, Steininger P, Ziegler R, Steinmann J,
Korn K, Ensser A: SARS-CoV-2 samples may escape detection because of a single point
mutation in the N gene. Euro Surveill 2020; 25: 2001650. PMID:33006300,
DOI:10.2807/1560-7917.ES.2020.25.39.2001650
- 42. World Health Organization: SARS-CoV-2
variant—United Kingdom. 21 Dec 2020. Available online:
https://www.who.int/csr/don/21-december-2020-sars-cov2-variant-united-kingdom/en (accessed
on 29 December 2020).
- 43. Mahase E: Covid-19: What have we learnt about the
new variant in the UK? BMJ 2020; 371: m4944. PMID:33361120,
DOI:10.1136/bmj.m4944
- 44. Deka S, Kalita D: Effectiveness of sample pooling
strategies for SARS-CoV-2 mass screening by RT-PCR: a scoping review. J Lab Physicians
2020; 12: 212–218. PMID:33268939, DOI:10.1055/s-0040-1721159
- 45. Lagopati N, Tsioli P, Mourkioti I, Polyzou A,
Papaspyropoulos A, Zafiropoulos A, Evangelou K, Sourvinos G, Gorgoulis VG: Sample pooling
strategies for SARS-CoV-2 detection. J Virol Methods 2021; 289: 114044. PMID:33316285,
DOI:10.1016/j.jviromet.2020.114044
- 46. Lohse S, Pfuhl T, Berkó-Göttel B, Rissland J,
Geißler T, Gärtner B, Becker SL, Schneitler S, Smola S: Pooling of samples for testing for
SARS-CoV-2 in asymptomatic people. Lancet Infect Dis 2020; 20: 1231–1232. PMID:32530425,
DOI:10.1016/S1473-3099(20)30362-5
- 47.de Salazar A, Aguilera A, Trastoy R, Fuentes
A, Alados JC, Causse M, Galan JC, Moreno A, Trigo M, Perez-Ruiz M, Roldan C, Pena MJ,
Bernal S, Serrano-Conde E, Barbeito G, Torres E, Riazzo C, Cortes-Cuevas JL, Chueca N,
Coira A, Sanchez-Calvo J M, Marfil E, Becerra F, Gude MJ, Pallares A, Perez Del Molino ML,
Garcia F: Sample pooling for SARS-CoV-2 RT-PCR screening. Clin Microbiol Infect 2020; 26 :
1687. e1-1687 e.5. doi:.DOI:10.1016/j.cmi.2020.09.008
- 48. Barat B, Das S, De Giorgi V, Henderson DK, Kopka
S, Lau AF, Miller T, Moriarty T, Palmore TN, Sawney S, Spalding C, Tanjutco P, Wortmann G,
Zelazny AM, Frank KM: Pooled saliva specimens for SARS-CoV-2 testing. J Clin Microbiol
2020; JCM.02486-20. PMID:33262219, DOI:10.1128/JCM.02486-20
- 49. Pasomsub E, Watcharananan SP, Watthanachockchai
T, Rakmanee K, Tassaneetrithep B, Kiertiburanakul S, Phuphuakrat A: Saliva sample pooling
for the detection of SARS-CoV-2. J Med Virol 2021; 93: 1506–1511. PMID:32841429,
DOI:10.1002/jmv.26460
- 50. Watkins AE, Fenichel EP, Weinberger DM, Vogels
CB, Brackney DE, Casanovas-Massana A, Campbell M, Fournier J, Bermejo S, Datta R, Dela
Cruz CS, Farhadian SF, Iwasaki A, Ko AI, Grubaugh ND, Wyllie AL: Pooling saliva to
increase SARS-CoV-2 testing capacity. medRxiv 2020.
doi:.DOI:10.1101/2020.09.02.20183830
- 51. CDC: A CDC 2019-novel coronavirus (2019-nCoV)
real-time RT-PCR diagnostic panel. Available online:
https://www.fda.gov/media/134922/download (accessed on 27 December 2020).
- 52. Turkistani K, Turkistani K: Dental risks and
precautions during COVID-19 pandemic: a systematic review. J Int Soc Prev Community Dent
2020; 10: 540–548. PMID:33282761, DOI:10.4103/jispcd.JISPCD_295_20