Abstract
The per-capita medical expenditures of elderly persons aged 75 years and older (hereafter, ME75) in each prefecture of western Japan and the Hokkaido area are higher than those in each of the eastern prefectures. This geographical uneven Distribution among ME75 in Japan can thus be summarized as follows: Per-capita medical expenditures among ME75 in Japan are higher in western areas than eastern areas (hereafter, WJhigh_EJlow). However, this uneven distribution has only been visually identified using a quartile map of ME75 without statistics. Further, current statistical verifications of the causes (e.g., supply and demand for medical care) are insufficient. As such, this study statistically confirmed uneven distribution among ME75 in different areas of Japan and identified the causes. Here, several specific analyses were conducted, including Fisher's exact test (hereafter, FET), bivariate Moran's I (hereafter, bi_MoI), and a quantitative analysis via multivariate regional clustering (hereafter, multi_RC) to adjust for confounding factors. All such analyses were performed using Bellcurve for Excel 3.20. Finally, a spacial_Multiple Regression Analysis (hereafter, spacial_MRA) of the GeoDa system was conducted to confirm uneven distribution, Results clearly showed a distribution of ME75 among all 47 Japanese prefectures following WJhigh_EJlow typed through multi_RC. Further, the population ratio of long-term care beds and general beds were identified as the main contributing economic medical factors via multi_RC with ME75 by spacial_MRA. The high ME75 in western Japan can be considered supporting evidence that elderly persons have high access to hospitals as required by the community-based integrated care system. On the other hand, low ME75 in eastern Japan will be evaluated because it will be considered to yield the collapse of the Japan's medical care system due to rapid rising of medical care expenditures. Therefore, further comparative studies will be necessary to determine whether the West Japan system is superior or the East Japan system is superior.
Introduction
Uneven geographical distributions between different regions [1–3] are observed not only in regard to nutritional intake and disease, but also in per-capita medical expenditures for people aged 74 and younger as well as elderly persons aged 75 and older. In Japan, there are extreme examples of uneven distribution among the 47 prefectures [4–8]. uneven distribution among the 47 prefectures among ME75 has been referred to as “Western High and Eastern Low: ME75s of prefectures in western Japan and the Hokkaido area are higher than those in eastern Japan” (hereafter, WJhigh_EJlow). However, confirmations of uneven distribution among the 47 prefectures as WJhigh_EJlow have only been determined visually using a categorized map of Japan, and there has been no objective confirmation of uneven distribution among the 47 prefectures via regional clustering [9, 10]. In addition, statistical verification is not sufficient for detecting and determining the main causes of factors related to medical demands, supply, socioeconomic issues, and lifestyle. This study confirmed the existence of uneven distribution among the 47 prefectures among ME75 and statistically analyzed the causes.
Materials and Methods
1. Subjects
This study's subjects were the 47 Japanese prefectures, each ME75, and relevant indexes such as disease prevalence and hospital bed types as categorized by the Japanese Ministry of Health, Labour and Welfare (hereafter, MHLW).
2. Flow of Methods
Method 1: Creation of fishbone diagram
Among the nine targets of previous research [11–18] and since Healthy Japan 21 began in 2000 [19], there has been a national movement to prevent lifestyle-related diseases. With reference to information on different dietary habits and luxury goods, we created a causes-and-effect diagram (the fishbone diagram [20]), which is composed of indicators related to ME75s in all 47 prefectures.
Method 2: Calculation of basic statistics
We obtained the calculation basics (denominators, etc), means, and standard deviations of each indices constituting the fishbone diagram.
Method 3: Confirmation of regional clustering and related types of ME75
The type of uneven distribution among the 47 prefectures among ME75 was identified using Fisher's exact test (hereafter, FET) and mono_variate Moran's I (hereafter, mono_MoI), while FET was used to identify uneven distribution among the 47 prefectures among ME75 between western Japan/Hokkaido and eastern Japan (excluding Hokkaido). The tendency for WJhigh_EJlow was statistically confirmed via comparison prefecture frequency, including those in the top 50% rank of all 47 prefectures' ME75 between western Japan and Hokkaido (24 prefectures) and eastern Japan (23 prefectures). This was done by applying regional classifications from the Japan Meteorological Agency (e.g., western and eastern Japan.) . On the other hand, mono_MoI was performed to confirm mono regional clustering (hereafter, mono_RC) [21,22] using the GeoDa [23] system.
Method 4: Trend analysis using FET
WJhigh_EJlow trends or the opposite WJlow_EJhigh trends of each index constituting the fishbone diagram were verified using FET; these results were called trend1. Second, we obtained each binary Moran's I (hereinafter, bi_MoI) between respective indices and ME75; these results were called trend2.
Method 5: Analyze using Spacial_MRA
Spacial_MRA of the GeoDa system [23] was quantitatively analyzed to confirm multivariate regional clustering (hereafter, multi_RC) while adjusting for confounding factors [24, 25]. Spacial_MRA was performed with ME75 as the objective variable, while each index of the fishbone diagram were the explanatory variables; results were called trend3.
Method 6: Creation of binary LISA cluster map
The respective uneven distribution between each index and ME75 were classified into three types (type1–3) based on the significance of the results for trends1, 2, and 3. Type1 was the case in which the indexes for both trend1 and trend3 were significant, while type2 was the case in which both trend2 and trend3 were significant (trend1 was not significant). On the other hand, type3 was another index from type1 or type2. Characteristic cases from three types of binary LISA cluster map (hereinafter, bi_LISA map) [21, 22] were thus illustrated.
The data used in this study were not subject to national ethical review (i.e., the ethics guidelines established by the Ministry of Education, Culture, Sports, Science and Technology · the Ministry of Health, Labour and Welfare, 2014) [26]. This was because none of the data were personal and all were obtained from published sources.
Results
1. Results of Method 1
Figure 1 shows the fishbone diagram of ME75, which is composed of six main causes and 25 secondary factors. According to previous studies including three of nine targets of the Healthy Japan21 campaign [19] such as food, smoking and alcohol, the fishbone diagram for ME75, the fishbone diagram is characterized by six main causes and 25 secondary causes. The breakdown of the main factors consisted of the following: I. Eating habits, II. Luxury grocery items, III. Regional (industrial) characteristics, IV. Factors related to medical care demand, V. Factors related to facilities for long-term care needs, and VI. Factors related to health and medical supplies.
2. Results of Method 2
Table 1 shows the basic statistics of the fishbone diagram comprising the effects (ME75) and 25 sub-causes shown in Figure 1.
3. Results of Method 3
Figure 2 shows the quartile map of ME75 with the FET value and mono_MoI value in all 47 Japanese prefectures. The type of mono_RC was identified as WJhigh_EJlow with a highly significant FET (p < 0.0001) value and highly significant mono_MoI value (p < 0.0001).
4. Results of Method 4
Table 2 shows trend1 for 25 indicators. The breakdown of trend1 is as follows: Eight indicators showed the WJhigh_EJlow type (No.1, 2, 7, 10, 11, 17, 19, 20) and were significant, while six indicators (No.4, 5, 11, 13, 15, 25) showed WJlow_EJhigh. Similarly, trend2 revealed that 20 binary regional clustering (hereafter, bi_RC) out of 25 were significant (Table 2).
5. Results of Method 5
Table 2 also shows the results of spacial_MRA as trend3. Here, five variables (No. 21–25 out of the 25 explanatory variables) were removed from the model due to multiple collinearity [27]. The final model of spacial_MRA consisted of 20 indices. The multiple regression coefficient showed a high value and significance as R = 0.9622 (p < 0.001). The coefficients of four indices were significant and lined up in descending order of the absolute t-values of the multiple regression coefficients. Results were as follows: Number of hospital beds (long-term care type) / population was highly significant (p < 0.0001), while number of hospital beds (general type) / population was also significant (p = 0.0022). The third major disease mortality rate was highly significant (p = 0.0051) with a negative tendency for community accumulation, while the fourth specific health checkup rate was significant (p = 0.0243).
6. Results of Method 6 and overall results
The overall results of Methods 1 through 6 are shown below (a)–(e). Here, 10 cases of characteristic bi_LISA map [21, 22] among the 25 indices are illustrated in Figures 3-1 through 3-10.
1) A: Western Japan RC
(a) Type 1(High-High): significant multi_RCs with ME75 were identified in the following cases:
i. Number of hospital beds (long-term care type) / population (p < 0.0001)
ii. Number of hospital beds (general type) / population (p = 0.0022)
(b) Type2(High-High): significant bi_RCs with ME75 were identified in the following cases:
i. Number of hospital beds (mental disease type) / population (p < 0.0001)
ii. Long-term care facility (visit type) / number of elderly persons aged 75 and older (p < 0.0006)
iii. Long-term care facility (day-care type) / number of elderly persons aged 75 and older (p < 0.0001)
iv. Long-term care facility (residential care type) / number of elderly persons aged 75 and older (p < 0.0001)
v. Public nurse ratio (p = 0.0050)
vi. Tertiary industry employment rate (p = 0.0113)
2) B: Eastern Japan RC
(c) Type1 (High-Low): significant multi_RCs with ME75 were identified in the following cases:
i. Rate of specific medical checkup (p = 0.0243)
(d) Type2 (High-High): significant bi_RCs with ME75 were identified in the following cases:
i. Rate of smoking habit (female) (p = 0.0001)
ii. Average salt intake (male) (p = 0.0004)
iii. Average salt intake (female) (p < 0.0001)
iv. Secondary industry employment rate (p = 0.0020)
3) RC neither A nor B
(e) Type3(High-Low): significant multi_RCs with ME75 were identified in the following cases:
i. Four leading causes of death / population
Four leading causes of death / population showed specific uneven distribution belonging to neither W_high_vs_E_low nor W_low_vs_E_high.
Discussion
Kawanobe et al. [13] conducted a multiple regression analysis which showed that the number of beds (a supply factor) primarily explained the increase in medical care expenditures. This was especially clear in regard to medical care expenditures for the elderly.
Matsui [15] found that age composition was the main cause of regional differences in per-capita medical care expenditures (WJhigh_EJlow). However, the disparity between these regional differences will not change. This situation is most likely due to differences in patient visiting behaviors to hospitals / clinics, even when adjusting for the influence of age.
Based on the results of a factor analysis and causal modeling path analysis, Innami [14] concluded that main factor contributing to uneven distribution related to WJhigh_EJlow were as follows: (1) age, (2) household composition, (3) municipal economy, (4) individual economy, and (5) area density (contribution ratio of nearly 50%). However, these viewpoints were merely related to regional differences among municipalities, meaning the evaluations were not produced through regional clustering.
The types of uneven distribution shown on the color-coded map of Japan (e.g., WJhigh_EJlow) are generally thought to be relatively easy to visually identify. However, we attempted to capture uneven distribution not merely subjectively, but also both objectively and numerically via regional clustering using both Moran's I and LISA cluster map [21,22].
This was done because the methods used in previous studies [11–19] were not based on RC if strictly distinguished. Namely, previous studies analyzed factors influencing differences in per-capita medical care expenditures between prefectures or municipalities, not to identify WJhigh_EJlow or other types of RC.
For example, a correlation analysis or multiple regression analysis is generally applied to prefectural data that is sorted with prefecture codes (i.e., 1–47). However, the exact same result is obtained no matter how the recorded order is changed in this case. This means that information on uneven distribution is not used at all in the analysis. As such, this study introduced spacial_MRA [21,22] to adjust for confounding factors, meaning that uneven distribution among ME75 was quantified via regional clustering and related factors were identified.
The overall results of Methods 1–6 show that the combination of indicators for both trend1 and trend3 were the most accurate for identifying and explaining uneven distribution in regard to WJhigh_EJlow among ME75.
The three indicators that met this condition for Type1 were the number of hospital beds (long-term care type) / population, number of hospital beds (general type)/population, and rate of specific medical checkup. The first two factors showed positive coefficients, while the rate of specific medical checkup showed a negative coefficient.
Honda's [11] analysis of the causes behind increasing national medical care expenditures indicated that “strengthening health checkups based on health Japan21[19] etc. might have increased the number of medical examinations and medical expenses.” However, a negative result was found for trend3 in this study. It was thus considered that the specific health checkup factor produced both primary and secondary prevention effects, as originally intended.
Among the nine indicators classified as type2, trend1 and trend2 revealed that “long-term care facility (three types) / population of elderly persons aged 75 and older” and “number of hospital beds (mental disease type) / population” were highly significant. In particular, the bi_MoI (0.6242) for “number of hospital beds (mental disease type) / population” was higher than that (0.4642) of “number of hospital beds (long-term care type) / population” (Figures 3–6). However, the bi_LISA map shown in Figures 3–6 was distributed in the high-high, low-low, and high-low zones in both western and eastern Japan, while uneven distribution for “number of hospital beds (long-term care type) / population” was simpler (Figures 3-1).
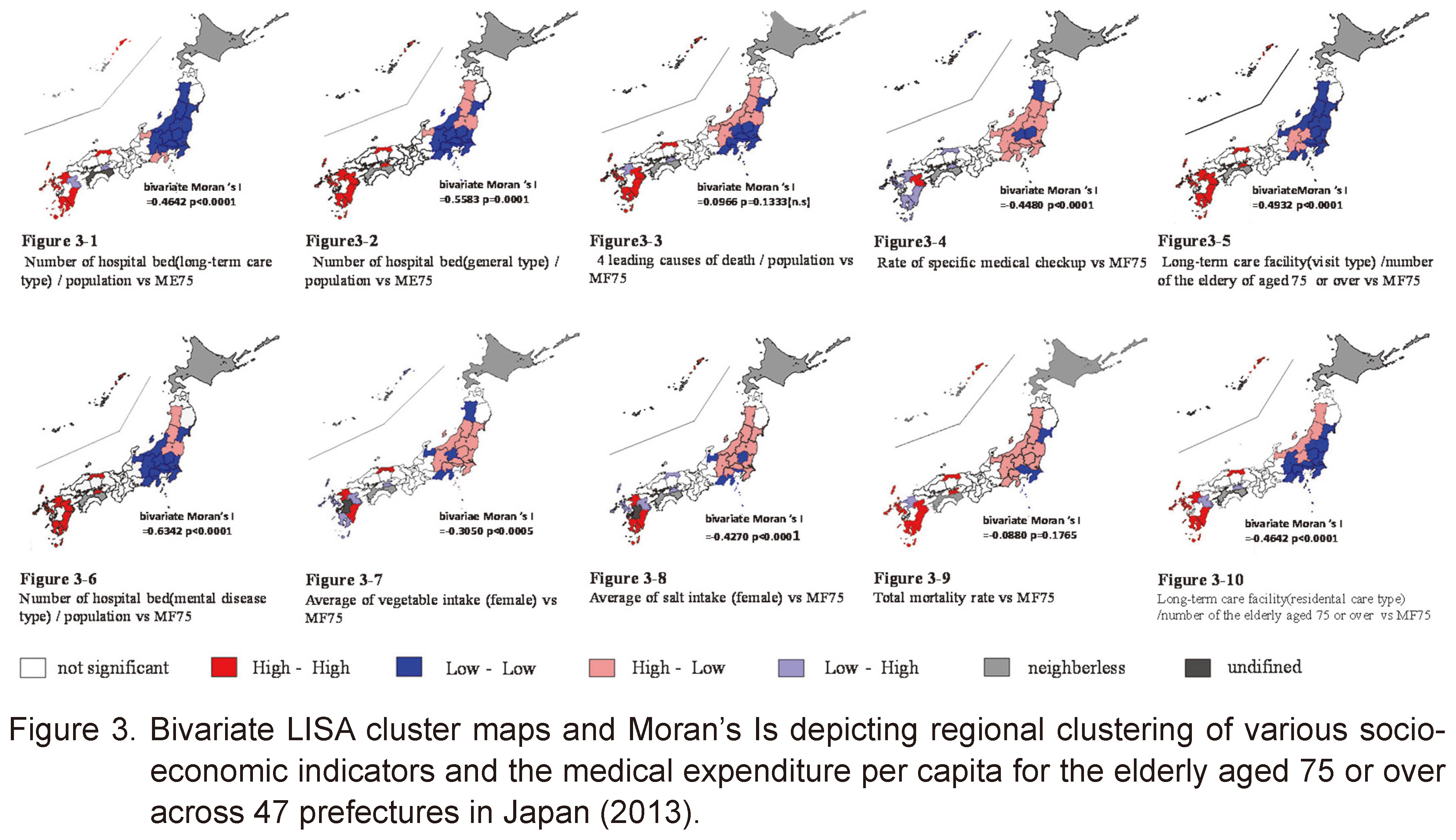
Number of the 6 indicators classified as type3, the four leading causes of death / population noted that the coefficient of spacial_MRA was significant and negative. The sum of the four leading causes of death / population was highly significant in trend3, though this was not the case for either trend1 or trend2. Namely, this index indicates highly significant uneven distribution that was neither WJhigh_EJlow nor the reverse pattern (Figures 3-3). From the Fisher's exact tests to evaluate uneven geographical distributions between the western Japan and then eastern Japan shown in Table 2, it can be seen that long-term care facility (residential care type: No.17) / population of elderly persons aged 75 and older vs. ME75 in western Japan, especially in Kyushu district long-term care facility (three types: No.7,10,17) / population of elderly persons aged 75 and older, number of hospital beds (long-term care type: No.1) / population, and number of hospital beds (general type: No.2) / population were of high rates in the western region. However, the results of spatial multiple regression analysis (objective variable: ME75 in Table 2 showed (highly) significant in only two variables related to types of hospital beds as long-term care type: No.1 and general type: No.2, whereas three types of long-term care facility (No.7,10,17) were not significant because long-term care expenditures were covered by not by health insurance system but the long-term care insurance system.
On the other hand, elderly suffered from severe illness in the intensive care home for the elderly are often admitted to hospitals with long-term care beds. It shows indirectly the cooperation between hospital and intensive care home is strong.
Honda [11] stated that “Japan's geriatric health care should provide as many medical services as possible for the long-term maintenance of healthy life expectancy, and then it is important to place the best possible level of medical care in Japan while taking into account the serious budget deficit”. This study's results showed that the amount of medical services available to the elderly were quite different between western Japan (including Hokkaido) and eastern Japan. Here, the main contributing supply factors were the number of long-term care beds and number of general beds. As a premise for interpreting this substantial instance of uneven distribution (i.e., the same issues presented by Honda [11]), it is necessary to determine how to consider and choose between the viewpoints and needs of medical quality, the economy, and policy.
Hiroi [28] cited the following four indicators as main contributing factors for increasing medical care expenditures: a) economic growth, b) accessibility to medical institutions, c) medical technology innovation, and d) aging. Of these, aging only applies to elderly persons aged 75 years and older. As such, this study did not consider the differences in aging rates among those over 75 years of age. However, the impacts were deemed small compared to medical care expenditures for persons up to 74 years of age. On the other hand, economic growth and medical technology innovation are considered effects that occur throughout the entire country, but they are also indicators that may have prefectural disparities. Finally, accessibility to medical institutions was a major factor that could not be introduced as a parameter at this time.
Conclusion
This study attempted to visually quantify uneven distribution among ME75 in Japanese prefectural units. Results showed clear RA typed WJhigh_Ejlow.
The ratios of long-term care beds and general beds were found to be the main medical economic factors influencing MF75. Further, high mortality rates and ME75 showed other types of RA as WJhigh_EJlow or WJlow_EJhigh. Future studies are needed to verify whether similar trends can be seen in secondary medical areas. For the elderly, the current RA of ME75 indicates that Japan's national medical care program can be summarized as “one country, two systems.” The biggest question is whether the high ME75 found in western Japan and Hokkaido is proof of the high accessibility required by the community-based integrated care system (CBICS) [29,30], which was proposed and attempted by MHLW. Specifically, authorities need to determine whether this should be extended to eastern Japan. On the other hand, Japan's aging society will become a more serious issues when coupled with innovations in medical technology in the near future. As such, it will eventually be necessary to regulate MF75 in order to maintain the current Japanese medical and welfare systems. In this regard, additional research is needed to determine the correct answer.
In addition, regarding the cooperation between Long-term care facilities and hospitals, in order to clarify the relationship of the qualitative provision system, it is necessary to analyze the causal relationship including the factors clarified in this study in the future.
Acknowledgments
The skeletal part of this study was conducted as part of a graduation study conducted during the 2019 fiscal year. We would like to thank the teachers working in the Department of Medical Informatics at Niigata University of Health and Welfare for their valuable guidance.
Conflicts of Interest
None of this study's authors have conflicts of interest or any financial ties to disclose.
References
- 1.WHO World Health Organization. Trace elements in human nutrition and health. Belgium: World Health Organization, 1996. 1-361.
- 2. Liggi M, Mais C, Demurtas M, et al. Uneven distribution of hepatic copper concentration and diagnostic value of double-sample biopsy in Wilson's disease. Scandinavian Journal of Gastroenterology. 2013; 48(12): 1452-1458.
- 3. Lee JS, Mogasale VV, Mogasale V, et al. Geographical distribution of typhoid risk factors in low- and middle-income countries. BMC Infect Dis. 2016; 16: 732. doi:10.1186/s12879-016-2074-1.
- 4. Matsui H. Iryuou Hiyou Kyusai Seisaku no Jissi to sono Kadai [Implementation of national medical expenses control measures and issues]. The Journal of Economic Policy Studies Kagawa University. 2009; 5: 125-145. (in Japanese)
- 5. Ishikawa M, Takahashi Y. Quantitative analysis of Japanese medical service level of each medical region. Journal of Japanese Association for Health Care Administrators. 2013; 71(1): 75-82. (in Japanese)
- 6. Ministry of Health, Labour and welfare. Analysis of regional differences in medical care expenditures (Medical care expenditure Map). Available from: https://www.mhlw.go. jp/stf/seisakunitsuite/bunya/kenkou_iryou/iryouhoken/database/iryomap/index.html (accessed October 25, 2019) (in Japanese)
- 7. Seki S, Kubo H, Yamada H, et al. Why does Japan's national insurance medical cost per capita geographically in the Japanese archipelago show high in the western half and in Hokkaido but low in the eastern half?. Niigata Journal of Health and Welfare. 2018; 18(1): 90 (in Japanese).
- 8. Fukuoka Prefecture. National Health Insurance medical expenses and national late elderly medical expenses.2018. Available from: http://www.pref.fukuoka.lg.jp/uploaded/life/310157_53254412_misc.pdf (accessed July 1, 2019) (in Japanese)
- 9. Takiguchi T, Yamamoto T, Aoyama H, et al. Spatial analyses of regional clustering of time-series trend of dft index among 3-year-old Japanese children in all 377 municipalities in Kanto area of Japan over a 10-year Period, 1998–2008. J Dent Hlth. 2012; 62(3): 296-304. (in Japanese)
- 10. Takiguchi T, Aoyama H, Fukai K, et al. Before-after (1998 and 2008) trend analyses on regional clustering of clinical dentist-to-population ratio in all 1,976 municipalities of Japan. Niigata Journal of Health and Welfare. 2012; 11: 78-93.
- 11. Honda Y. The analysis of the national medical expenses increase factor and the inspection of the medical expenses restraint policy. Policy science. 2016; 24(1): 15-31 (in Japanese).
- 12. Horii Y. Iryou-hi no Chiki Kakusa no Bunseki [Discussion on the analysis of regional disparities in medical expenses]. Iryo To Shakai. 1991; 1(1): 103-108. (in Japanese)
- 13. Kawanobe H, Ganryu Y. A quantitative analysis of the difference of medical treatment expenses between 47 prefectures in Japan. Public Choice Studies. 1999; 33: 29-44.
- 14. Innami I. Iryou-hi no Kettei Kouzou to Chiiki Kakusa [The structural determinations of Japanese health care expenditures and the explanation for its regional gap]. Iryo To Shakai. 1997, 7(3): 53-82. (in Japanese)
- 15. Matui H. Control of the national medical care expenditures measures and problems to be solved. The Journal of Economic Policy Studies, Kagawa University. 2009; 5: 125-145. (in Japanese)
- 16.Ministry of Health, Labour and Welfare 2013. Survey of medical facilities (dynamics) and the overview of hospital reports. Available from: https://www.mhlw.go.jp/toukei/saikin/hw/iryosd/13/dl/gaikyo.pdf (accessed October 20, 2019) (in Japanese)
- 17. Maeda Y. Kokumin Kenkou Hoken Iryou Map no Bunseki – naze Yamaguchi Ken Hitori Atari no Iryou-hi ha Ichii ni naru noka, naze Kagoshima Ken no Iryou-hi ha Koutou shite iru noka – [An analysis on the map of national medical care expenditures in Japan]. JMARI Working Paper. 2000; 39. (in Japanese)
- 18. Maeda Y. Iryou no Juyou to Kyoukyu ni tsuite [Demand and supply of medical care in Japan]. JMARI Working Paper. 2019; 429. (in Japanese)
- 19. Sakurai H. Healthy Japan 21. JMAJ. 2003; 46(2): 47-49.
- 20. Ilie G, Ciocoiu CN. Application of fishbone diagram to determine the risk of an event with multiple causes. Management research and practice. 2010; 2(1): 1-20.
- 21. Takiguchi T. A review of oral epidemiological statistics – Part VII: The bases of Spatial (Geographical) Epidemiology 1st flow-up review –. Health Science and Health Care. 2009; 9(1): 19-32. (in Japanese)
- 22. Takiguchi T. A review of oral epidemiological statistics – Part VIII: The bases of Spatial (Geographical) Epidemiology 2nd follow-up review –. Health Science and Health Care. 2010; 9(1): 4-19. (in Japanese)
- 23.GeoDa. An Introduction to Spatial Data Analysis. Available from: https://geodacenter. github.io (accessed April 15, 2019)
- 24.Berlin school of public health. Strategies to adjust for confounding: a friendly introduction, 2019. Available from: https://mef.unizg.hr/wp-content/uploads/2019/05/Strategies-for-Confounding-Adjustment.pdf (accessed November 9, 2019)
- 25. Takiguchi T. Kouraku Insi –Kekka wo Yugameru Haikei Inshi– [Confounding factors-background factors that distort results]. Dental Outlook. 2010; 116(6): 1152-1153. (in Japanese)
- 26.Ministry of Education, Culture, Sports, Science and Technology, Ministry of Health, Labor and Welfare. Ethical Guidelines for Medical Research for Humans. Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hokabunya/kenkyujigyou/i-kenkyu/index.html (accessed September 10, 2019) (in Japanese)
- 27.Statistic Solutions. Multicollinearity. Available from: https://www.statisticssolutions.com/multicollinearity/ (accessed November 9, 2019)
- 28. Hiroi Y. Increases of health care expenditures and economic growth – access, technological, change and aging –. Japanese Journal of Health Economics and Policy. 1994; 1: 69-82.
- 29. Masui H, Otaga M, Moriyama Y, et al. Current issues in long-term care policy and research: Toward the promotion of evidence-based policy. J Natl Inst Public Health. 2019; 68: 34-44.
- 30.Ministry of Health, Labour and Welfare; 2017. The community-based integrated care system. Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/kaigo_koureisha/chiiki-houkatsu/ (accessed August, 1, 2019) (in Japanese)




