Abstract
Bow Hunter’s syndrome is an unusual symptomatic vertebrobasilar insufficiency resulting from intermittent mechanical compression of the vertebral artery, and is rarely a trigger for cerebral infarction following thrombus formation on the damaged endothelial vessels (Bow Hunter’s stroke). The authors present an extremely rare case of a 45-year-old man showing Bow Hunter’s stroke due to congenital vertebral artery fenestration stretching and sliding between C1 and C2 after head rotation to the right. Congenital vertebral artery anomaly rarely causes cerebral infarction, but could cause embolic strokes by mechanical stretching without bony abnormalities.
Introduction
Bow hunter’s syndrome is defined as symptomatic, vertebrobasilar insufficiency caused by mechanical occlusion of the vertebral artery (VA) at the atlanto-axial level during head rotation, and was coined by Sorensen in 1978.1) It is generally associated with hemodynamic changes, often leading to vertigo and faintness.2) This condition sometimes causes artery-to-artery embolism due to endothelial damage by osseous process or thick fibrous band surrounding the VA at occipital/C1 or C1/C2, which is called Bow hunter’s stroke.3–10) We herein present an extremely rare case showing Bow hunter’s stroke due to stretching and sliding of the VA fenestration between C1 and C2, and discuss its clinical implications with a literature review. To our knowledge, this is the first report of Bow hunter’s stroke associated with stretching and sliding of a congenital VA fenestration without bony abnormalities.
Case Presentation
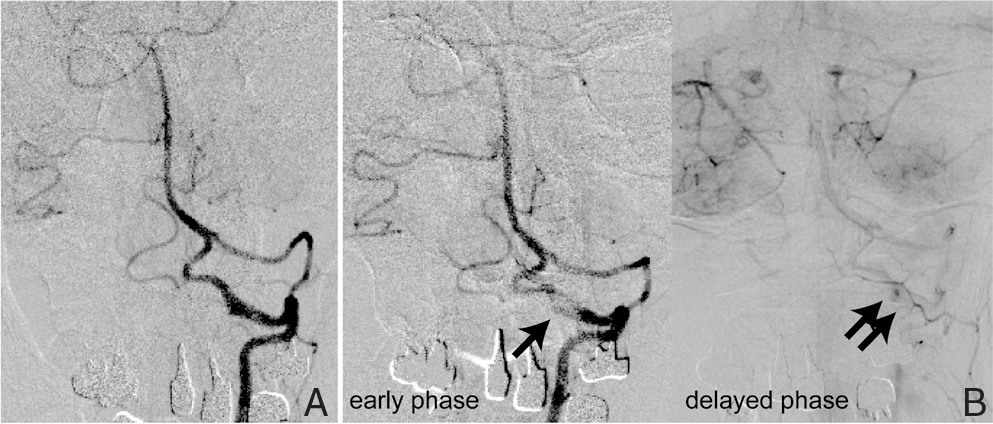
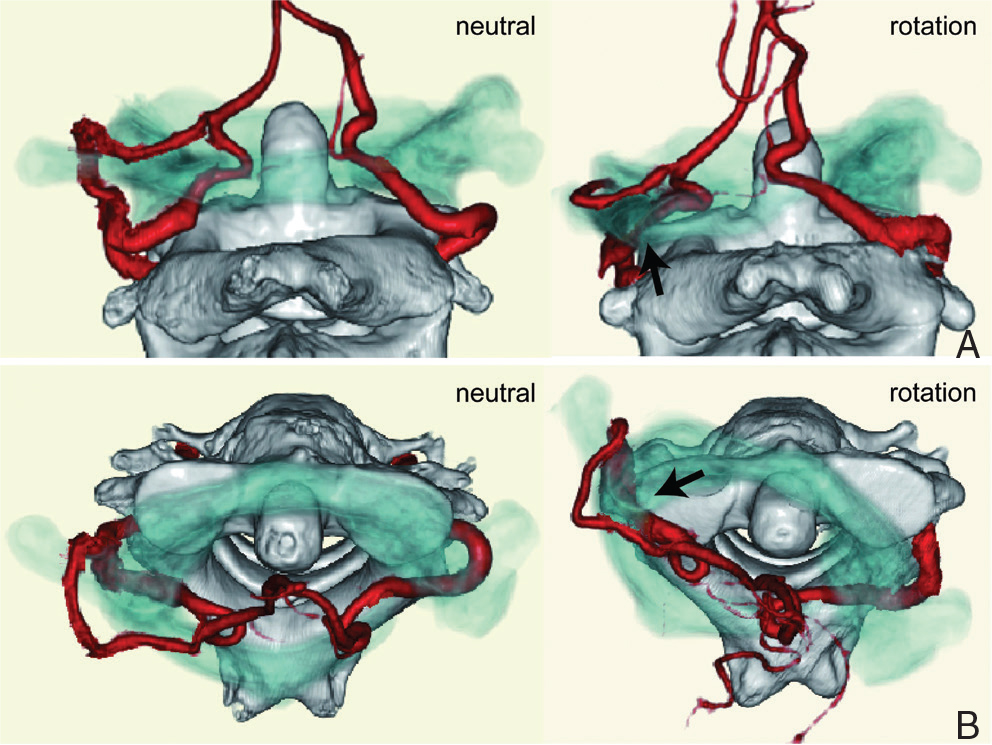
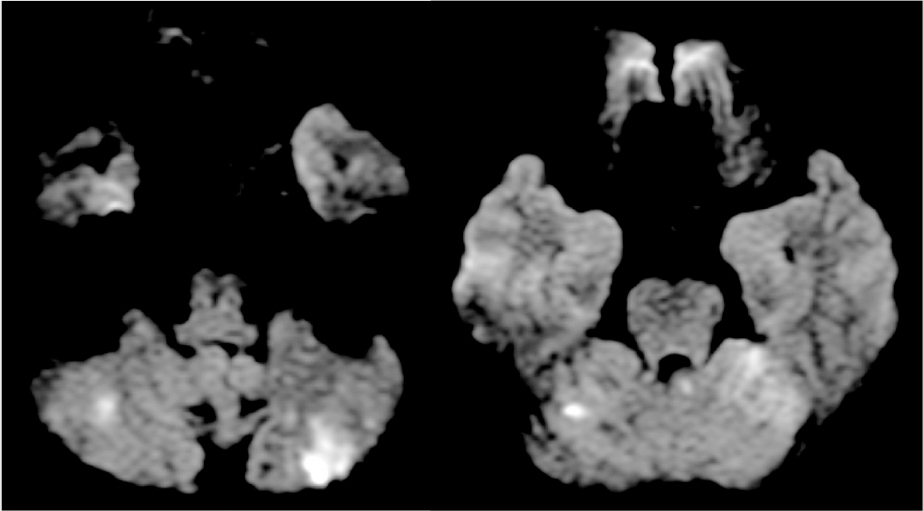
A 45-year-old man complained of repeated vertigo associated with head rotation to the right for 2 years. Magnetic resonance imaging (MRI) previously revealed multiple cerebellar infarctions, and the patient was transferred to our institute for further examination and treatment since the etiology of stroke was not clear. On admission, his physical and neurological examination showed no abnormalities. MRI showed multiple acute infarctions in the bilateral cerebellar hemispheres (Fig. 1). Magnetic resonance angiography and computed tomography angiography (CTA) showed no apparent stenosis or vessel occlusion in the posterior circulation, and only showed congenital anomalies including VA fenestration on the left side and the persistent first inter-segmental artery (FIA) on the right side. We further performed dynamic rotational angiography to assess the possibility of Bow hunter’s stroke. Interestingly, digital subtraction angiography (DSA) showed segmental elongation of the lower limb of the left VA fenestration (Fig. 2A), with a focal defect of the contrast media in the early phase and delayed pooling of the contrast media after head rotation to the right (Fig. 2B). Moreover, CTA clearly showed marked stretching and sliding of the left VA fenestration, and the lower limb was compressed between the C1 transverse process and C2 lateral mass in head rotation to the right (Fig. 3). We concluded that rotational stretching and sliding of the left VA fenestration contributed to this multiple cerebellar infarction, with endothelial damage and mural thrombus formation in the lower limb. After 38 days from last stroke, the patient underwent C1/C2 posterior fusion using C1/C2 transarticular screws and bone graft for prevention of further stroke. Postoperative course was uneventful and there was no longer compression of the inferior limb of the VA between C1 and C2 during head rotation after the surgery (Fig. 4). No symptoms or recurrent stroke have been observed in the patient to date, 24 months after the surgery.
Discussion
I. Epidemiology of VA fenestration
According to a previous report, congenital anomaly of VA at the C1/C2 level has three types: VA fenestration, persistent FIA, and posterior inferior cerebellar artery of C1/C2 origin.11) These congenital VA anomalies were found in 2.3–5.4% of patients.11–13) Extracranial VA fenestration is a well-known variation and most frequently seen at a C1/C2 level. This VA fenestration contains two limbs, an upper limb running between occipital bone and C1, and a lower limb running between C1 and C2, which was observed in 0.5–0.9% of patients.12,13) This is a very rare case showing both unilateral VA fenestration and contralateral persistent FIA, which is reported in 0.1% of patients.12) These VA anomalies are mostly found incidentally, especially in the examination of cervical spinal disorder.12–15) These VA anomalies are usually asymptomatic,13) although some authors have reported an associated aneurysm and subarachnoid hemorrhage.15–17)
II. Etiologies of stroke
We provided details of eight case reports showing Bow hunter’s stroke (Table 1).3–10) Interestingly, Bow hunter’s stroke occurred at a relatively younger age (mean 24.4 ± 7.2 years old), indicating that aging-related vessel change or bony change does not always contributed to Bow hunter’s stroke, contrary to expectations. Moreover, all the cases had associated bony abnormalities including congenital anomaly. In all the cases, the mechanism for Bow hunter’s stroke is reported as a compression or occlusion of the VA due to osseous process in head rotation. Interestingly, this case has some unique characteristics, which have not been reported so far. First, the patient had no existing bony abnormalities compressing the VA. Second, the patient had a congenital vessel anomaly affecting the Bow hunter’s stroke. Some reports showed mobile mural thrombus in the damaged vessel due to repeated VA compression by head rotation.7,10) This case also supports the mechanism of Bow hunter’s stroke as mural thrombus. MRI showed multiple infarcts in the area of the posterior circulation indicating embolic stroke. Further, DSA showed pooling of the contrast media in lower limb indicating endothelial damage. Stroke occurred at a middle age in this case and cervical spine radiographs showed no atlanto-axial instability or cervical spondylosis (Fig. 5).

Table 1
Reported cases of Bow hunter’s stroke and related mechanism
| Author (year) |
Age, sex |
Location |
Associated bony abnormality |
Associated vessel abnormality |
Mechanism |
Treatment |
| Shimizu et al. (1988)9) |
37, M |
Occipital-C1 |
Thickened membrane |
None |
Compression and occlusion of VA |
Surgical decompression |
| Tominaga et al. (2002)10) |
34, M |
Occipital-C1 |
Osseous process |
None |
Compression and occlusion of VA |
Surgical decompression |
| Lu et al. (2009)6) |
12, M |
Occipital-C1 |
Osseous process |
None |
Compression and occlusion of VA |
Surgical decompression |
| Greiner et al. (2010)5) |
15, M |
Occipital-C1 |
Osseous process |
None |
Compression of VA |
Surgical decompression |
| Saito et al. (2010)7) |
7, M |
C1-C2 |
Atlantoaxial subluxation |
None |
Compression of VA |
C1-C2 fusion |
| Sakamoto et al. (2011)8) |
16, M |
Occipital-C1 |
Occipitalization of atlas |
None |
Compression of VA |
Endovascular VA occlusion |
| Andereggen et al. (2012)3) |
66, M |
C5-C6 |
Osseous process |
None |
Compression of VA |
Surgical decompression |
| Cornelius et al. (2012)4) |
8, M |
C1-C2 |
C1-C2 bony malformation |
None |
Compression and occlusion of VA |
Surgical decompression |
| Present case |
45, M |
C1-C2 |
None |
VA fenestration |
Stretching and sliding of VA |
C1-C2 fusion |
The rotational movement in lower cervical vertebrae is limited due to degenerative changes caused by aging. By this limitation, excessive rotation in atlanto-axial joint is forced and lead to the stress of surrounding structure including ligaments.18) In our case, excessive rotation stretched VA, and this VA was compressed between C1 posterior arch and C2 lateral mass because of narrowing the space caused by excessive rotation. Repeated compression also causes sclerotic changes of VA.10) This stretching and compression damaged the intima of the sclerotic VA.
Regarding treatment strategies for Bow hunter’s stroke, surgical decompression such as C1/C2 fusion or endovascular VA occlusion was reported.3–10) In the present study, we performed C1/C2 fusion and the postoperative course was uneventful. Endovascular occlusion of the lower limb of VA is less invasive and could be a favorable option, but remains unclear whether an occluded vessel with coils remains stable against remaining repeated compression. Further accumulation of new cases is required to discuss the treatment option.
Conclusion
To our knowledge, this is the first report of Bow hunter’s stroke associated with stretching and sliding of the congenital VA fenestration between C1 and C2. This case indicates that patients with VA fenestration have a risk of cerebral infarction due to stretching and sliding into bony structures.
Conflicts of Interest Disclosure
None.
References
- 1) Sorensen BF: Bow hunter’s stroke. Neurosurgery 2: 259–261, 1978
- 2) Choi KD, Choi JH, Kim JS, Kim HJ, Kim MJ, Lee TH, Lee H, Moon IS, Oh HJ, Kim JI: Rotational vertebral artery occlusion: mechanisms and long-term outcome. Stroke 44: 1817–1824, 2013
- 3) Andereggen L, Arnold M, Andres RH, Raabe A, Reinert M, Gralla J: Bow hunter’s stroke due to prominent degenerative spinal disorder. Clin Neuroradiol 2: 355–358, 2012
- 4) Cornelius JF, George B, N’dri Oka D, Spiriev T, Steiger HJ, Hänggi D: Bow-hunter’s syndrome caused by dynamic vertebral artery stenosis at the cranio-cervical junction—a management algorithm based on a systematic review and a clinical series. Neurosurg Rev 35: 127–135, 2012
- 5) Greiner HM, Abruzzo TA, Kabbouche M, Leach JL, Zuccarello M: Rotational vertebral artery occlusion in a child with multiple strokes: A case-based update. Child’s Nervo Syst 26: 1669–1674, 2010
- 6) Lu DC, Gupta N, Mummaneni PV: Minimally invasive decompression of a suboccipital osseous prominence causing rotational vertebral artery occlusion. Case report. J Neurosurg Pediatr 4: 191–195, 2009
- 7) Saito K, Hirano M, Taoka T, Nakagawa H, Kitauchi T, Tanizawa E, Yoshida K, Sakurai Y, Tamura K, Nakase H, Yoshioka A, Sakaki T, Kichikawa K, Ueno S: Artery-to-artery embolism with a mobile mural thrombus due to rotational vertebral artery occlusion. J Neuroimaging 20: 284–286, 2010
- 8) Sakamoto Y, Kimura K, Iguchi Y, Iwanaga T, Toi H, Matsubara S, Uno M: An embolic bow hunter’s stroke associated with anomaly of cervical spine. Neurology 77: 1403–1404, 2011
- 9) Shimizu T, Waga S, Kojima T, Niwa S: Decompression of the vertebral artery for bow-hunter’s stroke. Case report. J Neurosurg 69: 127–131, 1988
- 10) Tominaga T, Takahashi T, Shimizu H, Yoshimoto T: Rotational vertebral artery occlusion from occipital bone anomaly: A rare cause of embolic stroke. Case report. J Neurosurg 97: 1456–1459, 2002
- 11) Tokuda K, Miyasaka K, Abe H, Abe S, Takei H, Sugimoto S, Tsuru M: Anomalous atlantoaxial portions of vertebral and posterior inferior cerebellar arteries. Neuroradiology 27: 410–413, 1985
- 12) Hong JT, Lee SW, Son BC, Sung JH, Yang SH, Kim IS, Park CK: Analysis of anatomical variations of bone and vascular structures around the posterior atlantal arch using three-dimensional computed tomography angiography. J Neurosurg Spine 8: 230–236. 2008
- 13) Uchino A, Saito N, Watadani T, Okada Y, Kozawa E, Nishi N, Mizukoshi W, Inoue K, Nakajima R, Takahashi M: Vertebral artery variations at the C1-2 level diagnosed by magnetic resonance angiography. Neuroradiology 54: 19–23, 2012
- 14) Lee SH, Kim ES, Eoh W: Posterior C1-2 fusion using a polyaxial screw/rod system for os odontoideum with bilateral persistence of the first intersegmental artery. J Neurosurg Spine 14: 10–13, 2011
- 15) Meila D, Tysiac M, Petersen M, Theisen O, Wetter A, Mangold A, Schlunz-Hendann M, Papke K, Brassel F, Berenstein A: Origin and course of the extracranial vertebral artery: CTA findings and embryologic considerations. Clin Neuroradiol 22: 327–333, 2012
- 16) Polguj M, Podgórski M, Jedrzejewski K, Topol M, Majos A: Fenestration and duplication of the vertebral artery: the anatomical and clinical points of view. Clin Anat 26: 933–943, 2013
- 17) Morita T, Takazawa H, Narisawa A, Kawaguchi T, Sasaki T, Nishijima M: [Operated case of a ruptured aneurysm arising from fenestration of the vertebral artery]. No Shinkei Geka 40: 221–227, 2012 (Japanese)
- 18) Greenberg AD: Atlanto-axial dislocations. Brain 91: 655–684, 1968