Abstract
Basilar artery dissection (BAD) presenting with subarachnoid hemorrhage (SAH) is life-threatening, but its treatment has not been established yet. We treated two patients with ruptured BAD. They were 40-year-old and 41-year-old women. Both of them were treated conservatively during the acute stage. In one patient, radiological abnormality of BAD improved spontaneously. In another patient, reconstructive endovascular treatment (stent with coiling) was required in the chronic stage because the lesion deteriorated morphologically. Neither of them suffered from rebleeding and both had favorable outcome. We reported two patients with ruptured BAD treated conservatively during the acute stage and their outcomes were favorable. We reviewed the literature of BAD presenting with SAH and discussed the management for these lesions.
Introduction
Basilar artery dissections (BADs) are rare lesions and little is known about its natural history. The clinical presentations of BADs are subarachnoid hemorrhage (SAH), brain ischemia, and brainstem compression. Ruptured BADs presenting with SAH seemed to have higher mortality rate than unruptured ones.1–7) Rebleeding of ruptured BAD leads to poor outcome, and preventive treatment for rebleeding should be performed in the same manner for other intracranial arterial dissections such as vertebral artery dissections (VADs). Although treatment for ruptured VAD is established, treatment for ruptured BAD has not been established. Surgical trapping or endovascular intraluminal occlusion with coiling in the acute stage is the standard therapy for ruptured VAD, but these treatments cannot be applied to ruptured BAD due to inevitable ischemic complications. The other surgical or endovascular therapies for ruptured BAD during the acute stage are hazardous and do not always prevent rebleeding completely.
We report two patients with ruptured BAD. One patient underwent conservative treatment during the acute stage, and the lesion improved spontaneously. Another one was treated conservatively during the acute stage, but reconstructive endovascular treatment (RET), i.e., stent assisted coiling, was required in the chronic stage because the lesion deteriorated morphologically. We review the literature of BAD presenting with SAH and discuss the management for these lesions.
Case Reports
I. Case 1
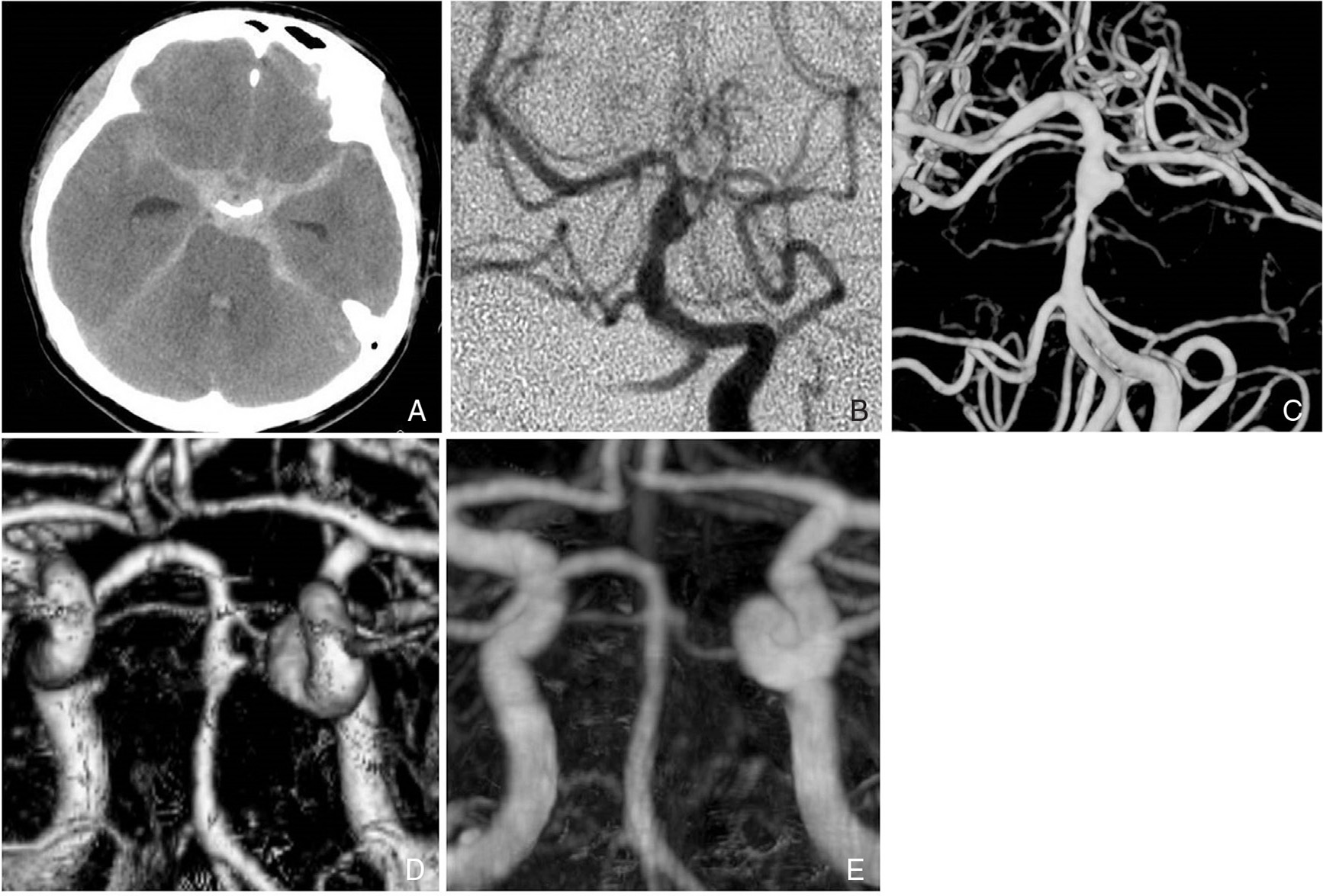
This 40-year-old woman was admitted to another hospital for consciousness disturbance following severe headache and vomiting. On admission, Glasgow Coma Scale (GCS) was 13 and no apparent hemiparesis was observed. Brain computed tomography (CT) showed diffuse SAH mainly in the basal and prepontine cisterns with mild ventricular dilatation (Fig. 1A). Cerebral angiography revealed moderate dilatation of the distal portion of the basilar artery (BA) (Fig. 1B). Under the diagnosis of ruptured BAD, she was treated conservatively with propofol (AstraZeneca, London, England) administration and blood pressure control. She was transferred to our hospital on Day 2 and the same conservative treatment was continued until Day 14. Rebleeding or symptomatic vasospasm did not develop. She had no apparent neurological deficit on Day 20. Three dimensional computed tomography angiography (3DCTA) on Day 20 showed enlarged dilatation of the lesion (Fig. 1C). Although we planned endovascular treatment, 3DCTA on Day 30 revealed improvement of the dilatation (Fig. 1D). The scheduled endovascular treatment was cancelled. She was discharged without any neurological deficit on Day 40. 3DCTA on Day 100 demonstrated normalization of the lesion (Fig. 1E). 3DCTA at 2 years also showed normal BA, and she was working at the previous office.
This 41-year-old woman was admitted to another hospital with restless confusion following severe headache and vomiting. On admission, GCS was 12 and no apparent hemiparesis was observed. CT showed diffuse SAH mainly in the basal and prepontine cisterns with marked ventricular dilatation (Fig. 2A). 3DCTA revealed moderate dilatation of the mid portion of the BA (Fig. 2B). Under the diagnosis of ruptured BAD with acute hydrocephalus, ventricular drainage was performed on the first day. She was treated conservatively with propofol administration and blood pressure control until Day 14. She suffered from no rebleeding or symptomatic vasospasm. 3DCTA on Day 20 showed aneurysmal dilatation of the lesion (Fig. 2C). She was transferred to our hospital on Day 25 for further treatment. On admission to our hospital, she had no apparent neurological deficit. Vertebral angiography also showed the aneurysmal dilatation of the mid portion of the BA (Fig. 2D). Dual antiplatelet premedication (aspirin and clopidogrel) was started on Day 30. Stent assisted coil embolization using Enterprise Vascular Reconstruction Device (VRD) (Johnson & Johnson, Miami, Florida, USA) was performed. Excelsior SL-10 (Stryker, Kalamazoo, Michigan, USA) was first introduced to the aneurysmal dilatation in the mid-BA. Then, Enterprise VRD 4.5 mm × 22 mm was deployed from P1 portion of the left posterior cerebral artery to the lower BA. Then, three coils (Orbit GALAXY, Johnson & Johnson, Miami, Florida, USA and Target 360 ULTRA, Stryker, Kalamazoo, Michigan, USA) were deposited in the lesion (Fig. 2E). Postoperative diffusion-weighted imaging showed small fresh infarction in the right pons and the left cerebellar hemisphere, but she had no neurological symptom. Postoperative course was uneventful and she was discharged without any neurological deficit on Day 60. Dual antiplatelet medication was continued for 6 months, and single antiplatelet medication (clopidogrel) was continued for another 6 months. Cerebral angiography at 1 year showed stable occlusion of the lesion compared to the outcome of the previous endovascular treatment (Fig. 2F), and she currently spends a normal life.

Discussion
Although BAD presenting with SAH is life-threatening, the treatment for these lesions has not been established. Rebleeding of ruptured BAD leads to poor outcome, thus preventive treatment for rebleeding is ideally performed during the acute stage. There are some options for ruptured BAD: conservative therapy, surgical therapy, endovascular therapy, and their combinations.
Including our two cases, 68 BADs presenting with SAH have been reported.1–28) Morphologically, there were 44 dilated lesions, 12 pearl-and-string lesions, 9 stenotic lesions, and 3 completely occluded lesions. In the latter two groups of steno-occlusive lesions (9 stenotic lesions and 3 complete occluded lesions), 10 were treated conservatively and 2 were treated with single stent replacement during the acute stage. None of the patients with steno-occlusive lesions suffered rebleeding. Excluding these 12 stenoocclusive lesions, the remaining 56 ruptured BADs (44 dilated lesions and 12 pearl-and-string lesions) including our 2 cases were further reviewed (Table 1). Two patients (5%) died soon after admission. In 33 patients (59%) of 56 ruptured BADs, surgical or endovascular therapy was performed in the acute stage. Four had surgical wrapping of the lesion, 4 had endovascular flow reversal therapy, 8 had endovascular coiling, and 17 had RET with stentings with or without coiling. Two of 33 patients (6%) with acute surgical or endovascular treatment presented with rebleeding (one with surgical treatment and the other with endovascular flow reversal therapy). Surgically treated patients had poor outcome [GOS: good recovery (GR) 50% (2/4)] and patients with endovascular flow reversal therapy had poor outcome [GOS: GR 50% (2/4)], whereas patients treated with RET had favorable outcome [GOS: GR 88% (15/17)]. The patients with endovascular coiling had good outcome [GOS: GR 75% (6/8)], but recanalization was observed in 2 patients (25%). In 21 patients (38%) of 56 ruptured BADs, conservative therapy was performed during the acute stage. Five of these 21 patients suffered rebleeding, and rebleeding rate of ruptured BAD treated conservatively was 24% (5/21). As for the rebleeding rate, there were no significant differences between dilated lesions and pearl-and-string lesions [dilated lesions: 23% (3/13), pearl-and-string lesions: 25% (2/8), Fisher exact test: P = 0.738]. In 21 conservatively treated patients, 7 had surgical or endovascular treatment in the chronic stage because the lesions deteriorated morphologically and 9 had no further treatment because of stable or improved lesions. As for the clinical outcome of 56 ruptured BADs, 39 patients (70%) were ranked as GR, 3 (5%) as mild disability, 4 (7%) as severe disability, and 9 (16%) as death.
Table 1
Review of the 56 ruptured basilar artery dissections including our two cases
| Baseline characteristics |
| General |
Mean age (years old) |
48.2 (17–78) |
| Woman |
34/56 (63%) |
| H&K grade |
1 |
6 (11%) |
| 2 |
21 (38%) |
| 3 |
11 (20%) |
| 4 |
7 (13%) |
| 5 |
6 (11%) |
| n.s. |
5 (9%) |
| Radiological finding |
Dilatation |
44 (79%) |
| Pearl-and-string |
12 (21%) |
| *Stenotic lesions and complete occluded lesions are excluded in this review. |
| Treatment |
| Acute stage |
None |
2 (5%) |
| Conservative therapy |
21 (38%) |
| Surgical wrapping |
4 (7%) |
| Endovascular flow reverse therapy |
4 (7%) |
| Endovascular coiling |
8 (14%) |
| RET with stents with or without coiling |
17 (30%) |
| Chronic stage |
Surgical flow reverse therapy |
4 (7%) |
| Surgical clipping |
1 (2%) |
| Endovascular coiling |
1 (2%) |
| RET with stents with or without coiling |
1 (2%) |
| Results |
| Rebleeding |
Conservative treatment |
|
| (dilated lesions) |
3/13 (23%) |
| (pearl-and-string lesions) |
2/8 (25%) |
| (total) |
5/21 (24%) |
| Acute surgical or endovascular treatment |
2/33 (6%) |
| GOS |
Good recovery |
39 (70%) |
| Mild disability |
3 (5%) |
| Severe disability |
4 (7%) |
| Vegetative state |
0 (0%) |
| Death |
9 (16%) |
| n.s. |
1 (2%) |
GOS: Glasgow Outcome Scale, H&K: Hunt & Kosnik, n.s.: not specified, RET: reconstructive endovascular treatment, SAH: subarachnoid hemorrhage, VRD: vascular reconstruction device.
The appropriate treatment of ruptured BAD depends on the anatomy of the lesion, and conservative therapy might be suitable for the steno-occlusive lesions. Treatment of the dilated lesions and the pearl-and-string lesions is controversial. According to our review, rebleeding rate of the dilated lesions and the pearl-and-string lesions treated conservatively was relatively high (24%). And the patients with acute surgical therapy had poor outcome, whereas the patients treated with acute RET had favorable outcome. Kim, et al. reported usefulness of acute RET with stenting with or without coiling.3) In their report, 6 of 7 patients with acute endovascular treatment recovered with complete or near-complete healing of the dissection on follow-up angiography. Jiang C, et al reported 18 ruptured BADs treated with acute endovascular therapy.2) In their report, coiling-only therapy without stenting was performed in 8 cases and RET with stenting with or without coiling was performed in 10 cases. Stented cases had better outcome than coiling-only cases and the coiling-only patients had a significantly higher recurrence rate than the patients with stent-assisted treatment. On the other hand, it remains unclear whether treatment should be performed in the chronic stage, when the lesions treated conservatively during the acute stage deteriorated morphologically. According to our review, all such cases underwent treatments in the chronic stage, and both surgically and endovascularly treated patients had good outcome.
Progress of endovascular treatment is ever-improving, and acute endovascular treatment for ruptured BAD becomes safer and more reliable recently. RET with stenting with or without coiling enables treatment of the lesions and preserve blood flow through the parent vessel and is suitable for dilated or pearl-and-string BAD presenting with SAH.
Although acute RET for ruptured BAD should be performed with great care to avoid ischemic complication, RET in the acute stage may be considered as a treatment option for ruptured BADs with high rebleeding risk, such as dilated lesions with bleb or pearl-and-string lesions.2,3)
References
- 1) Hosoda K, Fujita S, Kawaguchi T, Shose Y, Yonezawa K, Shirakuni T, Hamasaki M: Spontaneous dissecting aneurysms of the basilar artery presenting with a subarachnoid hemorrhage. Report of two cases. J Neurosurg 75: 628–633, 1991
- 2) Jiang C, Li Q, Liu JM, Huang QH: Endovascular treatment for the basilar artery dissection. Cardiovasc Intervent Radiol 37: 646–656, 2014
- 3) Kim BM, Suh SH, Park SI, Shin YS, Chung EC, Lee MH, Kim EJ, Koh JS, Kang HS, Roh HG, Won YS, Chung PW, Kim YB, Suh BC: Management and clinical outcome of acute basilar artery dissection. AJNR Am J Neuroradiol 29: 1937–1941, 2008
- 4) Masson C, Krespy Y, Masson M, Colombani JM: Magnetic resonance imaging in basilar artery dissection. Stroke 24: 1264–1266, 1993
- 5) O’Shaughnessy BA, Getch CC, Bendok BR, Batjer HH: Late morphological progression of a dissecting basilar artery aneurysm after staged bilateral vertebral artery occlusion: case report. Surg Neurol 63: 236–243; discussion 243, 2005
- 6) Ruecker M, Furtner M, Knoflach M, Werner P, Gotwald T, Chemelli A, Zangerle A, Prantl B, Matosević B, Schmidauer C, Schmutzhard E, Willeit J, Kiechl S: Basilar artery dissection: series of 12 consecutive cases and review of the literature. Cerebrovasc Dis 30: 267–276, 2010
- 7) Takagi M, Hirata K, Fujitsu K, Yamamoto I: Unusual angiographic changes in a dissecting aneurysm of the basilar artery: case report. Neurosurgery 34: 356–358; discussion 358, 1994
- 8) Adams HP, Aschenbrener CA, Kassell NF, Ansbacher L, Cornell SH: Intracranial hemorrhage produced by spontaneous dissecting intracranial aneurysm. Arch Neurol 39: 773–776, 1982
- 9) Ali MJ, Bendok BR, Tella MN, Chandler JP, Getch CC, Batjer HH: Arterial reconstruction by direct surgical clipping of a basilar artery dissecting aneurysm after failed vertebral artery occlusion: technical case report and literature review. Neurosurgery 52: 1475–1480; discussion 1480–1481, 2003
- 10) Amin-Hanjani S, Ogilvy CS, Buonanno FS, Choi IS, Metz LN: Treatment of dissecting basilar artery aneurysm by flow reversal. Acta Neurochir (Wien) 139: 44–51, 1997
- 11) Berger MS, Wilson CB: Intracranial dissecting aneurysms of the posterior circulation. Report of six cases and review of the literature. J Neurosurg 61: 882–894, 1984
- 12) Farrell MA, Gilbert JJ, Kaufmann JC: Fatal intracranial arterial dissection: clinical pathological correlation. J Neurol Neurosurg Psychiatr 48: 111–121, 1985
- 13) Friedman AH, Drake CG: Subarachnoid hemorrhage from intracranial dissecting aneurysm. J Neurosurg 60: 325–334, 1984
- 14) Hashimoto M, Johkura K, Ichikawa T, Kojima A, Nishimura S, Shinonaga M: Conservative treatment of ruptured vertebrobasilar dissecting aneurysm. Neurol Sci 29: 241–244, 2008
- 15) Imada Y, Ikawa F, Ohbayashi N, Matsushige T, Kajihara Y, Inagawa T, Ohba S: [Flow reverse therapy for ruptured dissecting aneurysm of basilar trunk: case report]. No Shinkei Geka 33: 587–592, 2005
- 16) Kai Y, Hamada J, Morioka M, Yano S, Hamasaki K, Ushio Y: Successful treatment of a ruptured dissecting basilar artery aneurysm. Case report. J Neurosurg 100: 1072–1075, 2004
- 17) Leonardi M, Raffi L, Simonetti L, Cenni P: Endovascular treatment of basilar artery dissection by stent deployment. A case report. Interv Neuroradiol 10: 315–319, 2004
- 18) Mori K, Nakayama T, Cho K, Hirano A, Maeda M: Dissecting aneurysms limited to the basilar artery: report of two cases and review of the literature. J Stoke Cerebrovasc Dis 7: 213–221, 1998
- 19) Nakahara T, Satoh H, Mizoue T, Kawamoto H, Kohmo Y, Kurisu K: Dissecting aneurysm of basilar artery presenting with recurrent subarachnoid hemorrhage. Neurosurg Rev 22: 155–158, 1999
- 20) Nakatomi H, Nagata K, Kawamoto S, Furusho JI: Basilar artery occlusion due to spontaneous basilar artery dissection in a child. Acta Neurochir (Wien) 141: 99–104, 1999
- 21) Oyama H, Kito A, Maki H, Noda T, Wada K: [Subarachnoid hemorrhage caused by dissection of the basilar artery: a case report]. No Shinkei Geka 41: 791–795, 2013
- 22) Pozzati E, Andreoli A, Padovani R, Nuzzo G: Dissecting aneurysms of the basilar artery. Neurosurgery 36: 254–258, 1995
- 23) Raychaudhuri R, Yu W, Hatanpaa K, Cavuoti D, Pride GL, White J: Basilar artery dissection treated by Neuroform stenting: fungal stent infection. Surg Neurol 28: 71: 477–480, 2009
- 24) Ross GJ, Ferraro F, DeRiggi L, Scotti LN: Spontaneous healing of basilar artery dissection: MR findings. J Comput Assist Tomogr 18: 292–294, 1994
- 25) Sakamoto S, Ohba S, Shibukawa M, Kiura Y, Okazaki T, Arita K, Kurisu K: Staged bilateral vertebral artery occlusion for ruptured dissecting aneurysms of the basilar artery: a report of 2 cases. Surg Neurol 64: 456–461; discussion 461, 2005
- 26) Woimant F, Spelle L: Spontaneous basilar artery dissection: contribution of magnetic resonance imaging to diagnosis. J Neurol Neurosurg Psychiatr 58: 540, 1995
- 27) Yoshimoto Y, Hoya K, Tanaka Y, Uchida T: Basilar artery dissection. J Neurosurg 102: 476–481, 2005
- 28) Zubkov AY, Sanghvi AN, Cloft HJ, Wijdicks EF, Rabinstein AA: Subarachnoid hemorrhage as a presentation of basilar artery dissection. Neurocrit Care 7: 165–168, 2007
