Abstract
The occurrence of cerebral vasospasm secondary to bacterial meningitis is relatively rare. Furthermore, there is no specific treatment cerebral vasospasm. Endovascular treatment may be essential for cases with the advanced clinical course. Balloon angioplasty or intra-arterial injection of verapamil, nicardipine, or nitroglycerin has been previously reported. We experienced successful treatment using intra-arterial infusion of fasudil hydrochloride. To our knowledge, this is the first case to report the intra-arterial injection of fasudil hydrochloride for treating cerebral vasospasm secondary to bacterial meningitis. A 37-year-old female who presented with dizziness had a right cerebellar tumor that was excised and diagnosed as glioblastoma. On postoperative day 10, Streptococcus oralis meningitis was detected. On postoperative day 20, the patient developed right hemiparesis with a severe vasospasm of the bilateral middle cerebral artery and anterior cerebral artery. Intra-arterial fasudil hydrochloride injection was performed for 3 days, following which the patient’s symptoms improved. Symptomatic cerebral vasospasm secondary to bacterial meningitis is relatively rare and difficult to treat; in selected cases, intra-arterial fasudil hydrochloride injection was an effective treatment for cerebral vasospasm secondary to bacterial meningitis.
Introduction
The occurrence of cerebral vasospasm secondary to bacterial meningitis is relatively rare compared with that after subarachnoid hemorrhage (SAH). Cerebral vasospasm that concurrently occurs after meningitis is not often detected as promptly as that after SAH, and it can cause severe complications.1) Furthermore, there is no specific and definitive treatment strategy for this condition, and this is similar to SAH. We treated patients with cerebral vasospasm secondary to bacterial meningitis using intra-arterial infusion of fasudil hydrochloride.
Case Report
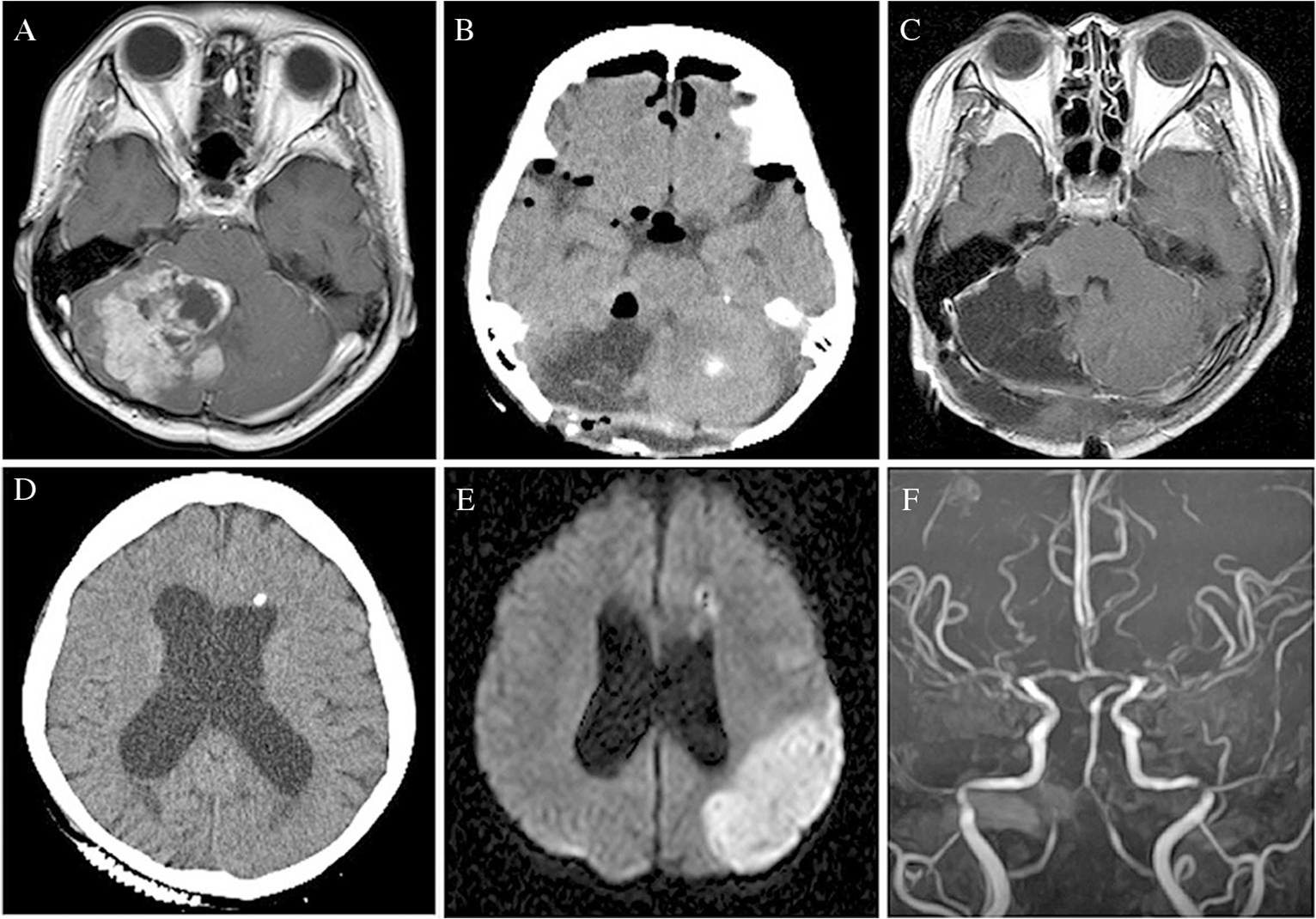
A 37-year-old female presented with dizziness. Mild cerebellar ataxia was observed in the right upper limb. MRI revealed an enhanced cystic mass lesion in the right cerebellar hemisphere (Fig. 1A). A gross total tumor excision was performed, the pathological diagnosis was glioblastoma (isocitrate dehydrogenase; wild-type, WHO grade IV). Intraoperative bleeding was not excessive (Figs. 1B and 1C), and the postoperative course was relatively good. However, Streptococcus oralis meningitis was detected on postoperative day 10. Ventricular drainage was performed on postoperative day 17 because of hydrocephalus (Fig. 1D); the meningitis had resolved by antimicrobial therapy. On postoperative day 20, the patient developed consciousness disturbance and right hemiparesis, and diffusion-weighted MRI showed a high-intensity region in the left parietal lobe (Fig. 1E). Magnetic resonance angiography showed poor visualization of bilateral middle cerebral artery and anterior cerebral artery (Fig. 1F), which was consistent with severe vasospasm by digital subtraction angiography (Figs. 2A and 2B). Fasudil hydrochloride (Asahi Kasei Corp., Tokyo, Japan) was intra-arterially administered to preserve antegrade blood flow and prevent further infarction.
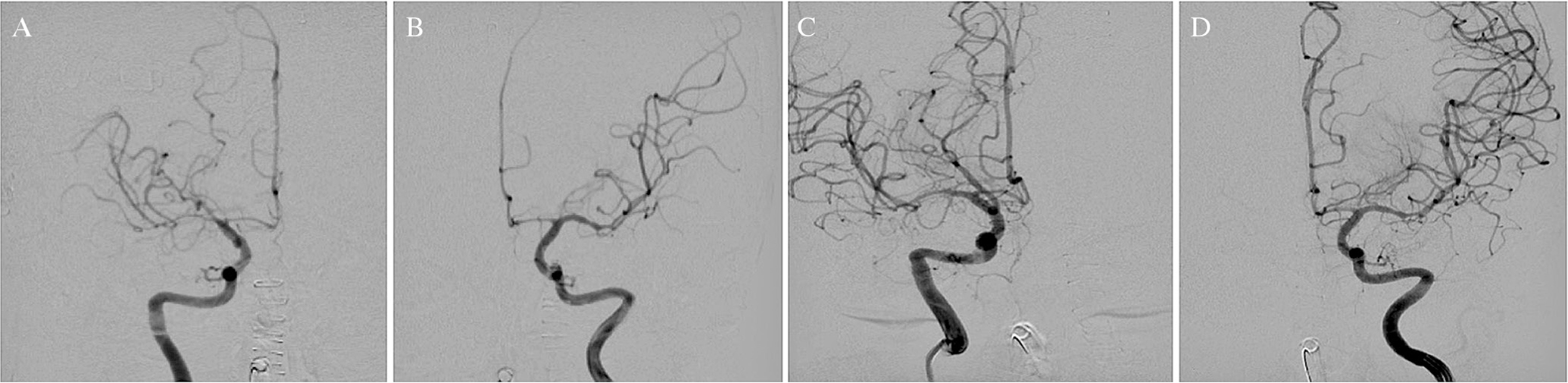
The patient was placed under local anesthesia, and a 5-French sheath was inserted in the right femoral artery. After systematic heparinization, a 5-French guiding catheter was positioned in the left internal carotid artery (ICA) and a microcatheter (Excelsior SL-10; Stryker, Kalamazoo, MI, USA) was navigated to the distal ICA. Thereafter, fasudil hydrochloride (15 mg) was injected for 10 min (1.5 mg/min). A similar procedure was performed on the right side, and the same amount of fasudil hydrochloride was injected. After natural reversal of heparin, CT revealed no new infarction after treatment. Cerebral vasospasm was improved by 3 days of fasudil hydrochloride injection (Figs. 2C and 2D). The patient’s symptoms gradually improved, and she was discharged with mild hemiparesis (modified Rankin Scale 2).
Discussion
Despite improvements in antimicrobial therapy, bacterial meningitis still has clinically significant morbidity and mortality.2,3) The clinical outcomes of bacterial meningitis are often affected by intracranial consequences, such as cerebral edema, hydrocephalus, and cerebrovascular complications.2,4) Cerebrovascular complications are common, but severe cerebral vasospasm that causes ischemic injury is rarely reported.5) Conversely, postmortem histopathological evaluation of patients who died of acute bacterial meningitis suggests that the occurrence of cerebral vasospasm is more frequent than reported.6) The pathogenesis of cerebral vasospasm in bacterial meningitis has not been elucidated and it is likely that inflammatory cytokines, leukocytes in the cerebrospinal fluid, and spasm-induced free radicals are involved.7–9)
The onset, duration, and recommended treatment of cerebral vasospasm associated with SAH are well known. Conversely, vasospasm associated with meningitis is relatively rare and treatment strategies are not well known.2) Hypervolemia, hypertension, and hemodilution (triple H) therapy can prevent ischemic deficit after cerebral vasospasm associated with meningitis but it is not always effective.10) Triple H therapy may also be harmful to patients because of the risk of cerebral hemorrhage in central nervous system infections.6)
Balloon angioplasty is regarded as an effective treatment for local cerebral vasospasm; however, inflammation weakens the arterial wall and increases the risk of vessel rupture during balloon inflation.1) Conversely, intra-arterial vasodilation is safe and extensively effective and results in a mild-to-moderate improvement in vessel diameter and distal flow. The treatment stabilizes the clinical condition and does not cause vascular rupture.7)
Nimodipine, nicardipine, papaverine, verapamil, and fasudil hydrochloride have been reported as intra-arterial vasodilator for vasospasm.11–17) Nimodipine and nicardipine have been associated with decreased arterial blood pressure.6) Papaverine is associated with the risk of injury to the vascular endothelium and media and should be used with caution. Furthermore, the risk of severe adverse effects, such as respiratory depression, tachycardia, systemic hypotension, cerebral hypertension, and brainstem symptoms must also be considered for papaverine.15,16) Fasudil hydrochloride is a novel and potent vasodilator. It inhibits protein kinases, such as Rho kinase, myosin light chain kinase, protein kinase C, and myosin light chain phosphorylation.18) Fasudil is as or more effective than nimodipine for the prevention of cerebral vasospasm and subsequent ischemic injury in patients undergoing SAH surgery.18) Fasudil hydrochloride is relatively safe, has little effect on blood pressure, has a dose-dependent effect on the relaxation of convulsive vascular tone, few effects on vascular endothelium or media, and contributes to its relative safety.19)
Recently, five cases of endovascular treatment for vasospasm secondary to bacterial meningitis have been reported (Table 1). All patients were male with an average age of 42 (20–57) years. Only one case was associated with postoperative meningitis.20) Two cases were treated with intra-arterial verapamil,5,7) one with intra-arterial nicardipine,7) and one with intra-arterial nitroglycerin and balloon angioplasty.21) All patients showed good recovery; therefore, an intra-arterial vasodilator, especially fasudil hydrochloride, might be a better option for vasospasm secondary to bacterial meningitis.
Table 1
Summary of treatment cases for vasospasm secondary to bacterial meningitis
| Author (year) |
Age(y)/Sex |
Strain |
Cause |
Timing (days) |
Place of spasm |
Treatment |
Outcome |
| Chaichana (2007)20) |
49/M |
Gram-positive cocci |
Post-operation |
14 |
ICA/ACA/MCA |
Triple H |
GR |
| Buechner (2012)21) |
20/M |
Staphylococcus aureus |
Sphenoid sinusitis |
11 |
ICA and MCA |
Nitroglycerin, PTA |
GR |
| Taqui (2014) |
38/M |
Streptococcus pneumoniae |
Mastoiditis |
9 |
VBA/PCA/ICA |
Verapamil |
GR |
| Taqui (2014)7) |
57/M |
Streptococcus pneumoniae |
Pneumoniae |
10 |
ICA/MCA/ACA |
Nicardipine |
GR |
| Nussbaum (2015)5) |
46/M |
Streptococcus viridans |
Sinusitis |
14 |
PCA |
Verapamil, Bypass |
GR |
| Present case |
37/F |
Streptococcus oralis |
Post-operation |
14 |
ACA/MCA |
Fasudil hydrochloride |
GR |
ACA: anterior cerebral artery, GR: good recovery, ICA: internal carotid artery, MCA: middle cerebral artery, PCA: posterior cerebral artery, triple H: hypervolemia, hypertension, and hemodilution therapy, VBA: vertebrobasilar artery.
Conclusion
Symptomatic cerebral vasospasm secondary to bacterial meningitis is relatively rare and difficult to treat. Endovascular treatment could be considered in selected cases of symptomatic cerebral vasospasm after meningitis. Intra-arterial vasodilator injection may be safer compared with balloon angioplasty. Fasudil hydrochloride should be considered for use as a vasodilator.
Acknowledgment
We would like to thank Dr. Takashi Maruyama and Dr. Syunsuke Tsuzuki for the initial treatment of this case.
Conflicts of Interest Disclosure
The authors have no financial conflicts of interests. All authors who are members of The Japan Neurological Society have registered online self-reported COI Disclosure Statement Forms through the JNS member website.
References
- 1) Hu YC, Newman CB, Bristol R, McDougall CG, Albuquerque FC: Percutaneous transluminal angioplasty in a patient with vasospasm secondary to coccidioidal meningitis: case report and review of the literature. J Neurointerv Surg 3: 62–65, 2011
- 2) Kawaguchi T, Ogawa Y, Inoue T, Tominaga T: Cerebral arteritis with extremely late onset secondary to bacterial meningitis -case report-. Neurol Med Chir (Tokyo) 51: 302–305, 2011
- 3) van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M: Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med 351: 1849–1859, 2004
- 4) Pfister HW, Borasio GD, Dirnagl U, Bauer M, Einhäupl KM: Cerebrovascular complications of bacterial meningitis in adults. Neurology 42: 1497–1504, 1992
- 5) Nussbaum ES, Lowary J, Nussbaum LA: A multidisciplinary approach to the treatment of severe cerebral vasospasm following bacterial meningitis: a case report and literature review. Surg Neurol Int 6: 148, 2015
- 6) Klein M, Koedel U, Pfefferkorn T, Zeller G, Woehrl B, Pfister HW: Arterial cerebrovascular complications in 94 adults with acute bacterial meningitis. Crit Care 15: R281, 2011
- 7) Taqui A, Koffman L, Hui F, et al.: Intra-arterial vasodilator therapy for parainfectious cerebral vasospasm. J Neurol Sci 340: 225–229, 2014
- 8) Fassbender K, Schminke U, Ries S, et al.: Endothelial-derived adhesion molecules in bacterial meningitis: association to cytokine release and intrathecal leukocyte-recruitment. J Neuroimmunol 74: 130–134, 1997
- 9) Fassbender K, Ries S, Schminke U, Schneider S, Hennerici M: Inflammatory cytokines in CSF in bacterial meningitis: association with altered blood flow velocities in basal cerebral arteries. J Neurol Neurosurg Psychiatry 61: 57–61, 1996
- 10) Kassell NF, Peerless SJ, Durward QJ, Beck DW, Drake CG, Adams HP: Treatment of ischemic deficits from vasospasm with intravascular volume expansion and induced arterial hypertension. Neurosurgery 11: 337–343, 1982
- 11) Albanna W, Weiss M, Müller M, et al.: Endovascular rescue therapies for refractory vasospasm after subarachnoid hemorrhage: a prospective evaluation study using multimodal, continuous event neuromonitoring. Neurosurgery 80: 942–949, 2017
- 12) Aburto-Murrieta Y, Marquez-Romero JM, Bonifacio-Delgadillo D, López I, Hernández-Curiel B: Endovascular treatment: balloon angioplasty versus nimodipine intra-arterial for medically refractory cerebral vasospasm following aneurysmal subarachnoid hemorrhage. Vasc Endovascular Surg 46: 460–465, 2012
- 13) Keuskamp J, Murali R, Chao KH: High-dose intraarterial verapamil in the treatment of cerebral vasospasm after aneurysmal subarachnoid hemorrhage. J Neurosurg 108: 458–463, 2008
- 14) Mazumdar A, Rivet DJ, Derdeyn CP, Cross DT, Moran CJ: Effect of intraarterial verapamil on the diameter of vasospastic intracranial arteries in patients with cerebral vasospasm. Neurosurg Focus 21: E15, 2006
- 15) Mathis JM, DeNardo A, Jensen ME, Scott J, Dion JE: Transient neurologic events associated with intraarterial papaverine infusion for subarachnoid hemorrhage-induced vasospasm. AJNR Am J Neuroradiol 15: 1671–1674, 1994
- 16) McAuliffe W, Townsend M, Eskridge JM, Newell DW, Grady MS, Winn HR: Intracranial pressure changes induced during papaverine infusion for treatment of vasospasm. J Neurosurg 83: 430–434, 1995
- 17) Tachibana E, Harada T, Shibuya M, et al.: Intra-arterial infusion of fasudil hydrochloride for treating vasospasm following subarachnoid haemorrhage. Acta Neurochir (Wien) 141: 13–19, 1999
- 18) Zhao J, Zhou D, Guo J, et al.; Fasudil Aneurysmal Subarachnoid Hemorrhage Study Group: Efficacy and safety of fasudil in patients with subarachnoid hemorrhage: final results of a randomized trial of fasudil versus nimodipine. Neurol Med Chir (Tokyo) 51: 679–683, 2011
- 19) Tanaka K, Minami H, Kota M, Kuwamura K, Kohmura E: Treatment of cerebral vasospasm with intra-arterial fasudil hydrochloride. Neurosurgery 56: 214–223, 2005
- 20) Chaichana K, Riley LH 3rd, Tamargo RJ. Delayed cerebral vasospasm secondary to bacterial meningitis after lumbosacral spinal surgery: case report. Neurosurgery 60: E206–E207, 2007
- 21) Buechner D, Gelfand MS, Cleveland KO. Percutaneous transluminal angioplasty in a patient with vasospasm due to staphylococcal meningitis. J Neurosurg 117: 103–106, 2012
