Case Reports
Dyspnea Associated with Cervical Spondylotic Radiculopathy: A Case Report and Review of Literatures
2021 Volume 8 Issue 1 Pages 195-200
Details
2021 Volume 8 Issue 1 Pages 195-200
When a patient presents with dyspnea, most physicians immediately associate it with cardiopulmonary diseases but not with the neurologic ones. Dyspnea due to cervical spondylosis rarely occurs, making it under-recognized. We report a case of a 57-year-old man who complained of dyspnea a month after his traffic accident. Chest X-ray showed a left diaphragm elevation, and cervical computed tomography (CT) revealed foraminal stenoses at C3/4, C4/5, and C5/6 on both sides, especially C3/4 on the left side. Anterior cervical discectomy and fusion at C3/4 and C4/5 were performed via a standard anterior cervical approach. Foraminal stenoses due to osteophyte were found to be more severe in the left side; therefore, thorough foraminotomies were performed. Titanium-coated polyether–ether–ketone (PEEK) cages filled with an artificial bone graft were inserted into both intervertebral spaces. His dyspnea improved immediately after the operation. Postoperative spirometry showed a gradually improving respiratory function. Therefore, cervical spondylosis should be considered to cause dyspnea, although it is an atypical symptom. Considering previous reports, outcomes achieved with surgical treatment were better than that with conservative therapy for cervical spondylotic radiculopathy-related dyspnea.
When a patient presents with dyspnea, most physicians immediately associate it with cardiopulmonary diseases, such as airway constriction or heart failure. However, dyspnea accompanied by diaphragmatic paralysis is suspected to be a phrenic nerve palsy, which may occur due to bronchogenic carcinoma, thoracic/neck surgeries, trauma, infection, or neurologic disease.1) However, involvement of the cervical spinal cord or nerve is seldom considered even though phrenic nerves originate from them. Herein, we report a rare case of cervical spondylotic radiculopathy with dyspnea. Related literatures were reviewed, and the efficacy of their surgical treatments was shown.
A 57-year-old man was referred to our hospital with dyspnea that started 2 months before his presentation. He had a traffic accident 3 months before presentation and was diagnosed with spinous process fractures from C3 to C6, sternum, and second to fourth ribs on the right side at a previous hospital. At the time, chest X-ray showed no abnormal findings (Fig. 1a). As the pain gradually decreased, he started to complain of dyspnea. His symptom gradually worsened, making it hard to go up the stairs and lie down to sleep. He visited the respiratory medicine and neurology departments of the previous hospital. Chest X-ray and computed tomography (CT) did not show any abnormal findings without elevation of the left diaphragm which was the contralateral side of rib fractures (Fig. 1b), thereby traumatic phrenic nerve palsy was suspected.

The patient had no medical history such as cardiopulmonary diseases; however, he was a current smoker. Neurological examination revealed a subtle paresthesia on the right forearm at the radial side as well as dyspnea and no hyperreflexia of the deep tendon reflexes nor spasticity. Flexion–extension views of the cervical X-ray did not show cervical instability. Cervical CT showed foraminal stenoses at C3/4, C4/5, and C5/6 on both sides, especially C3/4 on the left side (white arrow); however, the spinal canal was not that narrow (Fig. 2a–2c). Cervical magnetic resonance imaging (MRI) revealed mild disk bulging at C3/4, C4/5, and C5/6 without lateralities nor an intramedullary high signal on T2-weighted images (Fig. 2d–2f). Spirometry showed a mixed obstructive and restrictive defect with percent forced vital capacity (FVC) of 68.2%, and forced expiratory volume percent in one second (FEV1.0/FVC) of 56.4%. The latter dysfunction might be caused by smoking. The left phrenic nerve stimulation test2) suggested a low electrical potential. Based on these findings, his symptoms were suspected to be caused by cervical spondylotic radiculopathy at the left C4.

As the patient’s symptom might be triggered by trauma, whether it could be improved or not remains unclear. However, he opted to undergo surgery as no other options were available to resolve the problem. Finally, anterior cervical discectomy and fusion at C3/4 and C4/5 were performed to effectively decompress the nerve roots. The disk level to be operated was determined based on the phrenic nerve anatomy and his symptom of paresthesia on the right forearm.
Operative procedureAfter the induction of general anesthesia, the patient was placed in a neutral supine position. A transverse right-side skin incision was made to expose the C3, C4, and C5 vertebrae via a standard anterior cervical approach. Discectomies and bilateral foraminotomies were performed at each level. Foraminal stenoses due to osteophyte were more severe in the left sides (Supplementary Fig. 1, left; Supplementary Fig. 1 is available online.); therefore, thorough foraminotomies were performed using a bone curette and an ultrasonic aspirator, confirming sufficient root nerve decompressions (Supplementary Fig. 1, right). The posterior longitudinal ligament was excised, and no migrating disc was ensured. Titanium-coated polyether–ether–ketone (PEEK) cages (Mecta-C Cervical Cage; Medacta International, Castel San Pietro, Ticino, Switzerland) filled with an artificial bone graft made of hydroxyapatite and collagen and Refit (Hoya Technosurgical, Tokyo, Japan) were inserted into both intervertebral spaces. Intraoperative somatosensory- and motor-evoked potentials remained stable.
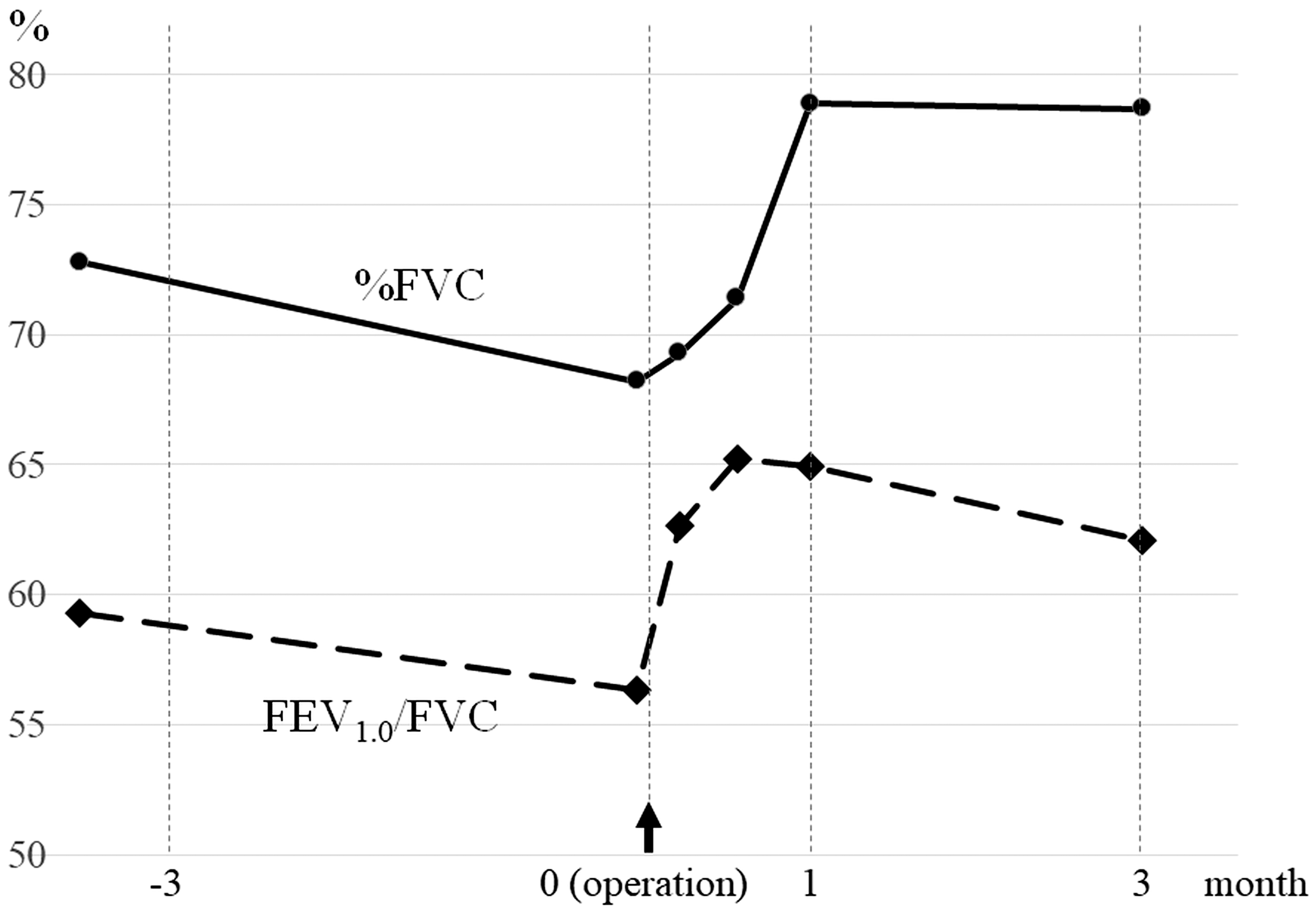
Postoperative courseNo complication or device failures were reported. During the immediate postoperative period, his dyspnea was ameliorated, allowing him to lie down without discomfort. Chest X-ray showed an improved hemidiaphragmatic elevation on the left side (Fig. 1c). Cervical CT proved expansion of each intervertebral foramen (Fig. 2g–2i). Postoperative spirometry also showed a gradually improving respiratory function: the %FVC became 78.9% and FEV1.0/FVC became 64.9% 1 month postoperatively (Fig. 3).
Dyspnea is an extremely rare symptom in cervical spondylosis, making it difficult to diagnose alone. To our best knowledge, only 10 cases of phrenic nerve palsy associated with cervical spondylotic radiculopathy exist, including the present case2–10) (Table 1), with nearly the same number of case reports associated with cervical myelopathy,11–19) and some case series showed a declined respiratory function in cervical myelopathy.20,21) Diagnosis of dyspnea associated with cervical spondylotic myelopathy is relatively straightforward because canal stenosis is easy to be recognized on radiological studies without paying any special attention and patients with cervical spondylotic myelopathy who complain of a dyspnea generally have other neurological symptoms. In contrast, dyspnea due to spinal nerve compression could be missed, especially if the spinal cord was not severely compressed. Radiological and neurological findings may be subtle as shown in the current case. Indeed, phrenic nerve palsy has been reportedly caused by motor root compression and the phrenic nerve receives its input from the third to fifth cervical nerve roots: the fourth nerve roots provide the main supply and the third/fifth roots are supplemental5,22); however, this fact may not be sufficiently recognized, and their compression is not carefully considered. In addition, no symptoms of the upper extremity usually accompany C4 radiculopathy, making it difficult to diagnose.
| Author, Year | Age, sex | Symptoms | Radiological findings | Treatment | Course of respiratory function (follow-up period) |
|---|---|---|---|---|---|
| Buszek et al., 19833) | 67, M | Shortness of breath Paracervical pain bil wrist/finger/shoulder weakness |
C3-5 canal stenosis bil C3/4, C4/5 foraminal steno |
C2-6 laminoplasty with C3/4, C4/5 foraminotomy |
Improved (6 weeks) |
| Cloward, 19884) | 47, F | Neck, lt arm pain lt hand numbness lt arm weakness Difficulty to sing |
C5/6, C6/7 canal stenosis lt C4/5 disc herniation |
C4/5, C5/6, C6/7 ACDF | Improved (ND) |
| Hayashi et al., 20055) | 64, M | Nuchal pain Dyspnea lt arm weakness lt arm hypesthesia |
C3/4 disc herniation and thickened ligamentum flavum C3 retrospondylolisthesis bil C3/4 foraminal stenosis C4-C7 osteophytes |
C3-7 laminoplasty | %VC: 66.6% → 73.9% FEV1.0%: 68.2% → 67.7% (6 weeks) |
| Weiss et al., 20116) | 59, M | Recurrent pneumonia Radiating pain | lt C2/3, C3/4 foraminal stenosis | Posterior cervical root Decompression | improved, no more pneumonia (10 month) |
| Reddy and Josephson, 20147) | 87, M | Orthopnea lt deltoid weakness |
bil C2/3, C3/4, C4/5 foraminal stenosis | BiPAP | not improved (over 2 years) |
| John and Tavee, 20158) | 49, M | Neck pain Orthopnea |
rt C3/4, C4/5, C5/6, lt C6/7 Foraminal stenosis |
BiPAP | %VC: 41% → 59% FEV1.0%: 71.5% → 76.3% (6 months) residual mild orthopnea (9 months) |
| Keelan et al., 20179) | 63, M | bil shoulder and neck discomfort Orthopnea | C5/6 canal stenosis C4/5, C5/6 disc bulging bil C3/4, C4/5 foraminal stenosis |
BiPAP Posterior foraminotomies |
not improved (ND) FVC: 3.88L → 4.86L |
| Singleton et al., 201810) | 64, M | Shortness of breath Intermittent neck pain |
rt C3/4, C4/5 foraminal stenosi | FEV1.0%: 62.9% → 64.4% (3 months) | |
| Manabe et al., 20192) | 70, M | lt arm pain bil hands numbness bil deltoids and rt biceps weakness Radicular pain (rt C5 dermatome) Hypoesthesia (below C5 dermatome) |
C3 retrospondylolisthesis C3/4 canal stenosis C3/4, lt C4/5 foraminal stenosis |
C4 laminoplasty +rt C3/4 foraminotomy +lt C4/5 foraminotomy +C2-5 posterior fusion |
%VC: 90.2% → 102.6% FEV1.0%: 72.5% → 72.3% (10 days) |
| Present case, 2020 | 57, M | Dyspnea lt arm numbness |
lt C3/4, bil C5/6 foraminal stenosis C3/4, C4/5 mild disc bulging |
C3/4, C4/5 ACDF | %VC: 68.2% → 78.7% FEV1.0%: 56.4% → 74.0% (3 months) |
ACDF: anterior cervical discectomy and fusion, bil: bilateral, BiPAP: bilevel airway positive pressure, C: cervical, F: female, FEV1.0%: forced expiratory volume percent in one second, FVC: forced vital capacity, lt: left, M: male, ND: not described, rt: right, %VC: percent vital capacity.
Among reported cases of cervical spondylotic radiculopathy-related dyspnea, there were nine men and one woman. Their mean age was 62.7 (range, 47–87) years. Most of them (9/10) had foraminal stenosis at C3/4 or C4 root compression. Multiple nerve roots were involved in eight cases, including the present case. The present case with severe foraminal stenosis at C3/4 and mild at C4/5; nevertheless, nerve decompressions were performed for both levels based on the following perspectives: (1) decompression of the C5 nerve root partially associated with the phrenic nerve could additionally improve dyspnea and (2) multiple nerve roots were involved and targeted for operation in most reported cases. Seven patients underwent surgical treatments, whereas the others received conservative therapies, such as bilevel airway positive pressure. When improvement is defined as ameliorations of dyspnea and/or respiratory function, all patients who underwent surgery improved, whereas those who did not undergo surgery did not improve. Surgical decompression for dyspnea due to cervical spondylotic radiculopathy tended to improve the symptom compared with conservative therapy statistically (Fisher's exact test, p = 0.0667).
As described above, reports of phrenic nerve palsy with cervical spondylotic radiculopathy are relatively rare. However, such cases might be more potentially observed. O’Beirne et al.23) reported that ipsilateral cervical foraminal stenoses are commonly detected in patients diagnosed with “idiopathic” diaphragmatic paralysis. They also argued that cervical foraminal stenosis may possibly be an underrecognized cause of diaphragmatic palsy. Thus, whether foraminal stenosis exists or not in patients complaining of dyspnea or diaphragmatic paralysis of unknown cause should be carefully considered. In conclusion, we reported a rare case of surgically improved cervical spondylotic radiculopathy with dyspnea. Therefore, cervical spondylosis may cause dyspnea, although it is an atypical symptom, and latent patients may have not been diagnosed yet. Considering previous reports, better outcomes can be achieved with surgical treatment than with conservative therapy for dyspnea included by cervical spondylosis.
The authors report no conflict of interest associated with this paper. All authors have registered online Self-reported COI Disclosure Statement Forms through the website for JNS members.
Foraminal stenoses due to osteophytes were more severe at the left sides at C3/4 (left, double arrows). After the resection of the lateral osteophyte, enough decompression of the posterolateral corner where the left C4 nerve root might be running was confirmed (right, asterisk).