Abstract
Although the synchronous occurrence of testicular seminoma and systemic sarcoidosis has been reported, that of intracranial germinoma and systemic sarcoidosis is unknown. A 26-year-old man presented with symptoms of panhypopituitarism and consciousness disturbance. Imaging demonstrated a large nodule in the upper right lung field and swelling of multiple bilateral pulmonary and mediastinal lymph nodes in addition to the bifocal pineal and suprasellar tumors with obstructive hydrocephalus. The pathological diagnosis of the intracranial bifocal tumors was pure germinoma, whereas that of the mediastinal lymph nodes was epithelioid granuloma. Three courses of chemotherapy using carboplatin and etoposide were administered, followed by whole ventricle irradiation. The intracranial tumors completely disappeared, but the lung nodule and mediastinal lymph nodes progressed. Whole-body fluorine-18-fluorodeoxyglucose positron emission tomography demonstrated accumulation in the mediastinal lymphadenopathy, lung masses, and multiple lymph nodes of the whole body. Transbronchial lung biopsy revealed epithelioid granuloma with multinucleated giant cells. In conjunction with the high blood concentration of angiotensin-converting enzyme and soluble interleukin-2 receptor, these findings established a diagnosis of sarcoidosis. This is the first report of synchronous occurrence of intracranial germinoma and sarcoidosis. Such coexistence is extremely rare, but we should mind that sarcoidosis can occur with intracranial germinoma.
Introduction
Although the synchronous occurrence of testicular seminoma and systemic sarcoidosis has been reported,1–4) that of intracranial germinoma and systemic sarcoidosis is unknown. We report a unique case of synchronous occurrence of intracranial germinoma and systemic sarcoidosis.
Case Study
Clinical course
A 26-year-old man presented with a 4-month history of general fatigue, walking disturbance, loss of appetite, and body weight loss. He had also suffered from polyuria, urinary incontinence, and pubic hair loss. Chest CT demonstrated a large nodule in the upper right lung field and swelling of multiple bilateral pulmonary and mediastinal lymph nodes (Fig. 1A and 1D). MRI demonstrated bifocal pineal and suprasellar tumor with obstructive hydrocephalus (Fig. 2A–C). The serum human chorionic gonadotropin (HCG), HCG-β, and alpha-fetoprotein (AFP) level was 4 mIU/mL (normal, <2mIU/mL), 0.4 ng/mL (normal, <0.1 ng/mL), and 2 ng/mL (normal, <10 ng/mL), respectively. The patient underwent a biopsy of suprasellar and pineal tumors using neuro-endoscopy and endoscopic ultrasound-guided fine-needle aspiration of the mediastinal lymph nodes. The pathological diagnosis was pure germinoma of the intracranial bifocal tumor (Fig. 3A–C). In contrast, only epithelioid granuloma was found in the mediastinal lymph nodes (Fig. 3D), which were immunohistologically negative for c-KIT (Fig. 3E) and placental alkaline phosphatase (Fig. 3F).

Fig. 1
Coronal chest contrast-enhanced CT scans obtained before chemotherapy (A and D), 2 weeks after the start of chemotherapy (B and E), and after three courses of chemotherapy (C and F). Dotted arrows, arrows, and arrowheads indicate the nodule in the right upper lung field, mediastinal lymph node, and lymph nodes located between the recurrent laryngeal nerve and the right common carotid artery, respectively.
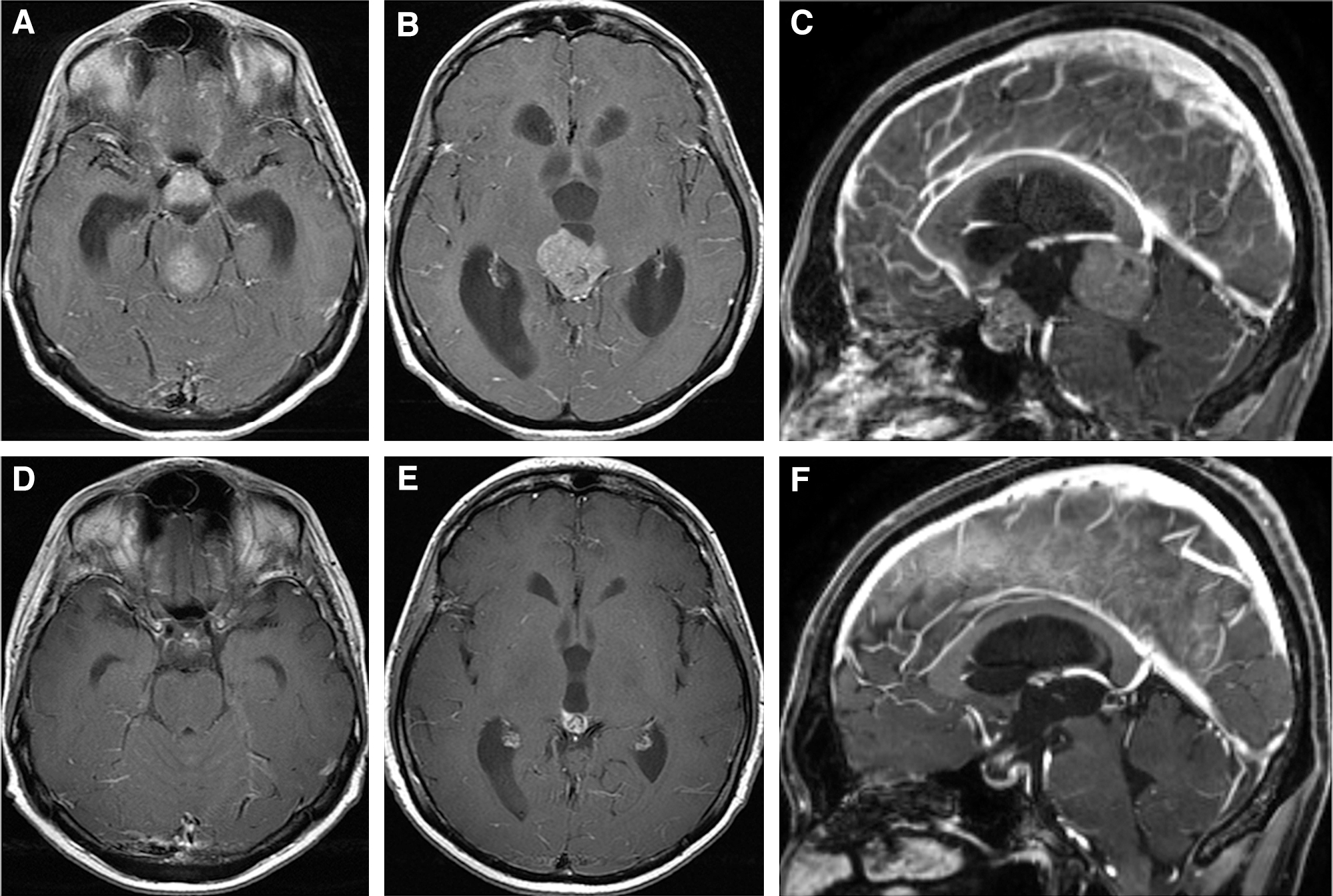
Fig. 2
Contrast-enhanced MRIs obtained before chemotherapy (A–C) and after three courses of chemotherapy and irradiation (D–F). (A, B, D, and E) Axial images, (C and F) midsagittal images.

Fig. 3
Photomicrographs of hematoxylin and eosin staining ((A, G) original magnification ×200; (D) original magnification ×100), and immunohistochemical staining (original magnification ×400) for c-KIT (B and E) and placental alkaline phosphatase (C and F) of the biopsied specimens from the pineal lesion (A–C), from the mediastinum lymph nodes obtained by endoscopic ultrasound-guided fine needle aspiration before chemotherapy (D–F), and from the mediastinum lymph node specimen obtained by transbronchial lung biopsy after three courses of chemotherapy (G).
Carboplatin and etoposide (CARE) administration with dexamethasone as an antiemetic agent was prescribed. MRI and CT obtained 2 weeks after the start of CARE therapy demonstrated apparent shrinkage of suprasellar and pineal tumors, a nodule in the upper right lung field, and the mediastinal lymph nodes (Fig. 1B and 1E). MRI after three courses of CARE therapy and whole ventricle irradiation 23.4 Gy showed complete disappearance of the intracranial bifocal tumors (Fig. 2D–F). Chest CT demonstrated shrinkage of some mediastinal lymph nodes, but a progression of the nodule in the right upper lung and swelling of the lymph nodes located between the recurrent laryngeal nerve and the right common carotid artery (Fig. 1C and 1F).
Whole-body fluorine-18-fluorodeoxyglucose positron emission tomography (FDG-PET) demonstrated accumulation in the mediastinal lymphadenopathy, lung masses, and multiple lymph nodes of the whole body (Fig. 4). Subsequently, a transbronchial lung biopsy was performed. Histological examination of specimens from the right upper lung mass showed epithelioid granuloma with multinucleated giant cells (Fig. 3G). These findings, in conjunction with the high blood concentration of angiotensin-converting enzyme (ACE, 32.4 U/L) and soluble interleukin-2 receptor (sIL-2R, 962 U/mL), established diagnosis of the body lymphadenopathies as sarcoidosis.

Fig. 4
Whole-body fluorine-18-fluorodeoxyglucose positron emission tomography image.
Discussion
The present case is the first report of synchronous occurrence of intracranial germinoma and systemic sarcoidosis. The diagnosis of sarcoidosis is based on three major criteria5,6): clinical presentation, histological findings of non-necrotizing granulomatous inflammation, and the exclusion of alternative causes of other granulomatous diseases, which were all met by the present case. Germinomas sometimes appear predominantly as a granulomatous reaction,7) so we presumed that this patient had intracranial and mediastinal multiple germinomas at the initiation of therapy. Indeed, there were case reports of metachronous intracranial germinoma and mediastinal seminoma8) or mediastinal growing teratoma syndrome.9) However, after three courses of CARE therapy, chest CT showed progression of lymphadenopathy and FDG-PET demonstrated accumulation of FDG into the whole-body lymph nodes. Evidence of multisystem organ involvement supports sarcoidosis, not a sarcoid-like reaction10); therefore, we could diagnose sarcoidosis in this patient.
Several epidemiological studies suggested a correlation between sarcoidosis and cancer.10–12) Sarcoidosis affects immune dysregulation and chronic inflammation, which may increase the frequency of mutation and potentiate the risk of generating malignancy.10–12) On the contrary, whether cancer causes sarcoidosis is not fully understood due to its rarity.10,13) Among the rare, a literature review presented that the cumulative incidence of sarcoidosis after testicular cancers is approximately 100-fold higher than a general population of young white men,4,14) and the interval between the initial diagnosis of testicular cancer and the following sarcoidosis was 12–288 months.13,14) We should note the presence of selection bias and surveillance bias,10,12) but previous findings suggested a correlation between testicular tumor and sarcoidosis. Similarly, intracranial germinoma, a counterpart of the testicular tumor, and sarcoidosis can correlate. These two diseases were synchronously found in our case, and symptomatic disease duration was 4 months; therefore, we suspected that the preceding sarcoidosis might cause intracranial germinoma and not vice versa. In general, simultaneous sarcoidosis and cancer are associated with poor prognosis,15,16) but particularly sarcoidosis in testicular cancer is not related to prognosis.17) The prognostic importance of simultaneous sarcoidosis and germinoma is unknown; therefore, careful observation is mandatory.
Sarcoidosis is generally treated with steroids and immunosuppressive agents. The nodule in the upper right lung field and mediastinal lymph nodes were reduced after the first course of CARE chemotherapy, probably because the protocol included steroid administration. These lesions could easily be misdiagnosed as germinoma. Since CT and MRI cannot clearly differentiate between germ cell tumors and sarcoidosis, tissue biopsy and blood sampling to examine the concentrations of ACE and sIL-2R were necessary to make the definitive diagnosis of sarcoidosis. Also, FDG-PET was not sufficient to diagnose germinoma,18) but helped to detect sarcoidosis.19) Some patients with mediastinal lesions coexistent with testicular germ cell tumor have been treated under misdiagnoses of sarcoidosis, resulting in inadequate interventions for true metastatic germ cell tumor, or have died due to unnecessary chemotherapy for sarcoidosis.3,20) We should be aware that sarcoidosis can occur in patients with intracranial germ cell tumors.
Conclusion
We reported a case of synchronous occurrence of intracranial germinoma and systemic sarcoidosis. The etiological association between intracranial germinoma and sarcoidosis is still unclear, but neurosurgeons should be aware of such coexistence.
Ethics Approval
The ethics committee of Kitasato University School of Medicine and the Japan Neurosurgical Society do not require ethics approval for case reports.
Informed Consent
Written informed consent was obtained from the patient.
Conflicts of Interest Disclosure
The authors declare that they have no conflict of interest.
References
- 1) Jeurkar N, Mamtani R, Vaughn DJ: Granulomatosis and testicular germ cell tumors. Urology 80: 1303–1306, 2012
- 2) Kaikani W, Boyle H, Chatte G, et al.: Sarcoid-like granulomatosis and testicular germ cell tumor: the ‘Great Imitator’. Oncology 81: 319–324, 2011
- 3) Tjan-Heijnen VC, Vlasveld LT, Pernet FP, Pauwels P, De Mulder PH: Coincidence of seminoma and sarcoidosis: a myth or fact? Ann Oncol 9: 321–325, 1998
- 4) Toner GC, Bosl GJ: Sarcoidosis, “Sarcoid-like lymphadenopathy,” and testicular germ cell tumors. Am J Med 89: 651–656, 1990
- 5) Statement on sarcoidosis: Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med 160: 736–755, 1999
- 6) Crouser ED, Maier LA, Wilson KC, et al.: Diagnosis and detection of sarcoidosis. An official American thoracic society clinical practice guideline. Am J Respir Crit Care Med 201: e26–e51, 2020
- 7) Endo T, Kumabe T, Ikeda H, Shirane R, Yoshimoto T: Neurohypophyseal germinoma histologically misidentified as granulomatous hypophysitis. Acta Neurochir (Wien) 144: 1233–1237, 2002
- 8) Bedano PM, Bonnin J, Einhorn LH: Metachronous intracranial germinoma in a patient with a previous primary mediastinal seminoma. J Clin Oncol 24: 2386–2387, 2006
- 9) Iwata H, Mori Y, Takagi H, et al.: Mediastinal growing teratoma syndrome after cisplatin-based chemotherapy and radiotherapy for intracranial germinoma. J Thorac Cardiovasc Surg 127: 291–293, 2004
- 10) Chopra A, Judson MA: How are cancer and connective tissue diseases related to sarcoidosis? Curr Opin Pulm Med 21: 517–524, 2015
- 11) Cohen PR, Kurzrock R: Sarcoidosis and malignancy. Clin Dermatol 25: 326–333, 2007
- 12) Søgaard KK, Sværke C, Thomsen RW, Nørgaard M: Sarcoidosis and subsequent cancer risk: a Danish nationwide cohort study. Eur Respir J 45: 269–272, 2015
- 13) Grados A, Ebbo M, Bernit E, et al.: Sarcoidosis occurring after solid cancer: a nonfortuitous association: report of 12 cases and review of the literature. Medicine (Baltimore) 94: e928, 2015
- 14) Rayson D, Burch PA, Richardson RL: Sarcoidosis and testicular carcinoma. Cancer 83: 337–343, 1998
- 15) Spiekermann C, Kuhlencord M, Huss S, Rudack C, Weiss D: Coexistence of sarcoidosis and metastatic lesions: a diagnostic and therapeutic dilemma. Oncol Lett 14: 7643–7652, 2017
- 16) Boffetta P, Rabkin CS, Gridley G: A cohort study of cancer among sarcoidosis patients. Int J Cancer 124: 2697–2700, 2009
- 17) Paparel P, Devonec M, Perrin P, et al.: Association between sarcoidosis and testicular carcinoma: a diagnostic pitfall. Sarcoidosis Vasc Diffuse Lung Dis 24: 95–101, 2007
- 18) Okochi Y, Nihashi T, Fujii M, et al.: Clinical use of (11)C-methionine and (18)F-FDG-PET for germinoma in central nervous system. Ann Nucl Med 28: 94–102, 2014
- 19) Orii M, Imanishi T, Akasaka T: Assessment of cardiac sarcoidosis with advanced imaging modalities. Biomed Res Int 2014, 897956, 2014
- 20) Colebunders R, Bultinck J, Servais J, Denis L: A patient with testis seminoma, sarcoidosis, and neutropenic enterocolitis. Hum Pathol 15: 394–396, 1984