Abstract
Aneurysms of the A1 segment of the anterior cerebral artery tend to develop in combination with various vascular anomalies of the A1 segment. Arterial branches that originate from the A1 segment and perfuse cortical regions are known to be rare. In this report, we describe a 48-year-old woman who presented with a ruptured aneurysm at the origin of an anomalous cortical artery arising from the A1 segment, for which microsurgical neck clipping was performed. Intraoperatively, the anomalous artery was seen to originate from the A1 segment, running into the interhemispheric fissure. An aneurysm was located at the bifurcation of the anomalous artery and the A1 segment. Postoperative angiography showed that the anomalous artery has branched into the fronto-orbital artery and the frontopolar artery and terminated as the anterior internal frontal arteries. We report a rare case of an aneurysm arising from an anomalous callosomarginal artery that arose from the A1 segment and perfused the cortical region. It is of significance to recognize that an aneurysm can develop at the origin of an anomalous artery that arises from the A1 segment.
Introduction
Aneurysms of the anterior cerebral artery (ACA) are usually detected in the anterior communicating artery or the distal portion of the ACA. Aneurysms of the A1 segment are deemed relatively rare, accounting for 0.88-2.1% of all cerebral aneurysms.1-5) The most common site of the A1 segment aneurysms is the origin of the perforating arteries, accounting for 55.6-88.9% of such aneurysms.2-4) A1 segment aneurysms also tend to be associated with other anomalies, such as fenestration, accessory middle cerebral artery, and azygous ACA.3,4,6,7) Arterial branches that originate from the A1 segment and perfuse cortical regions are rare.6,8-10) Further, origin of the callosomarginal artery (CMA) from the A1 segment has only been rarely reported.11,12)
Herein, we report a case of a patient who had a ruptured aneurysm at the origin of an anomalous CMA arising from the A1 segment of the ACA.
Case Report
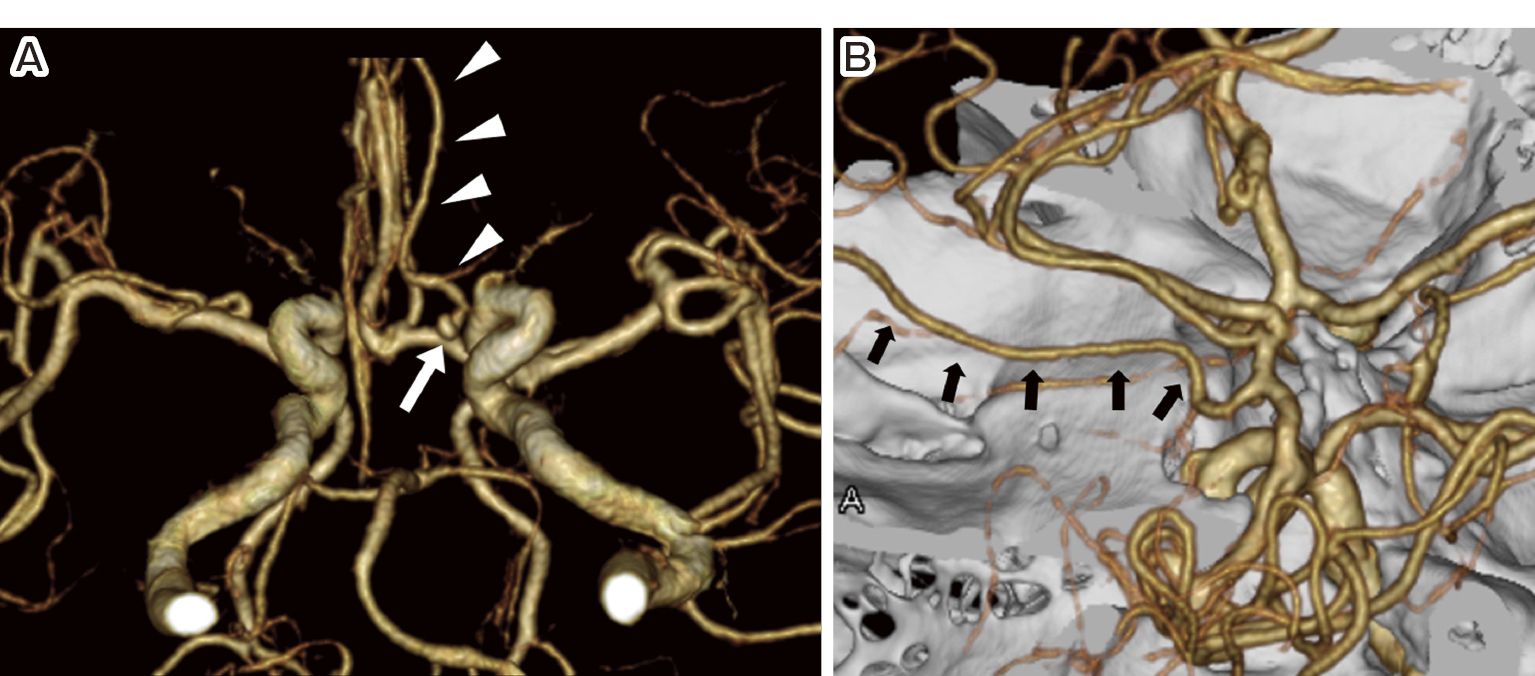
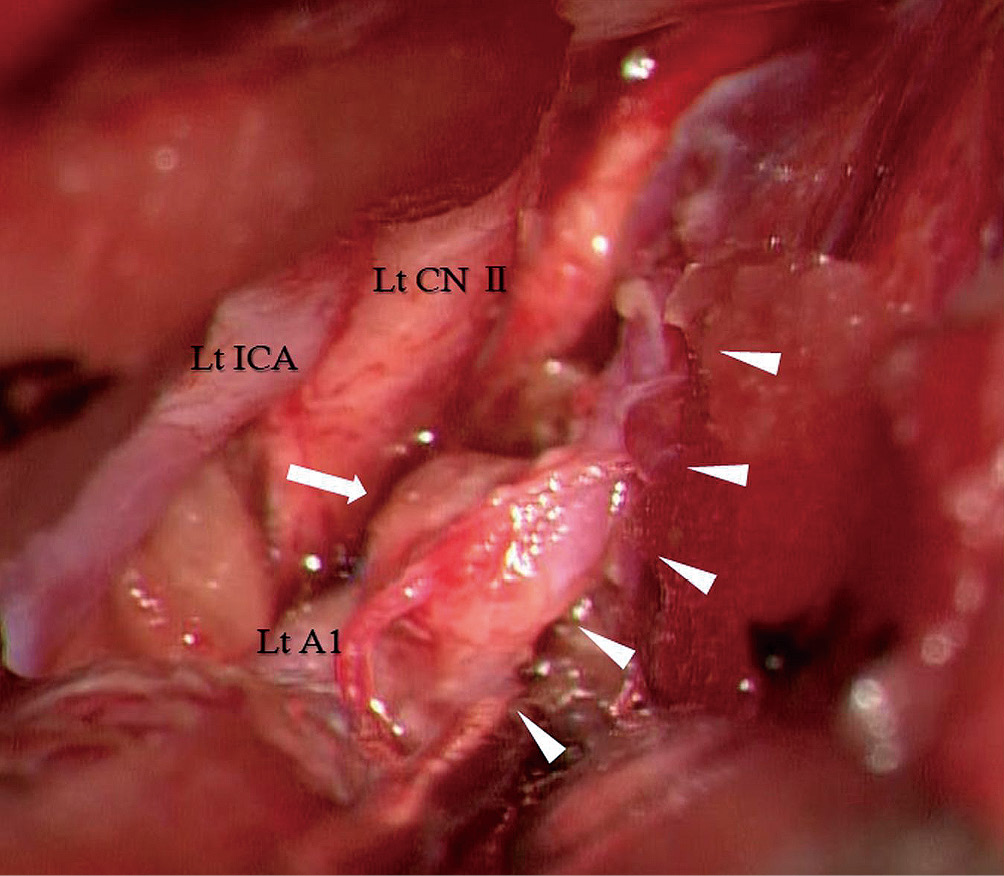
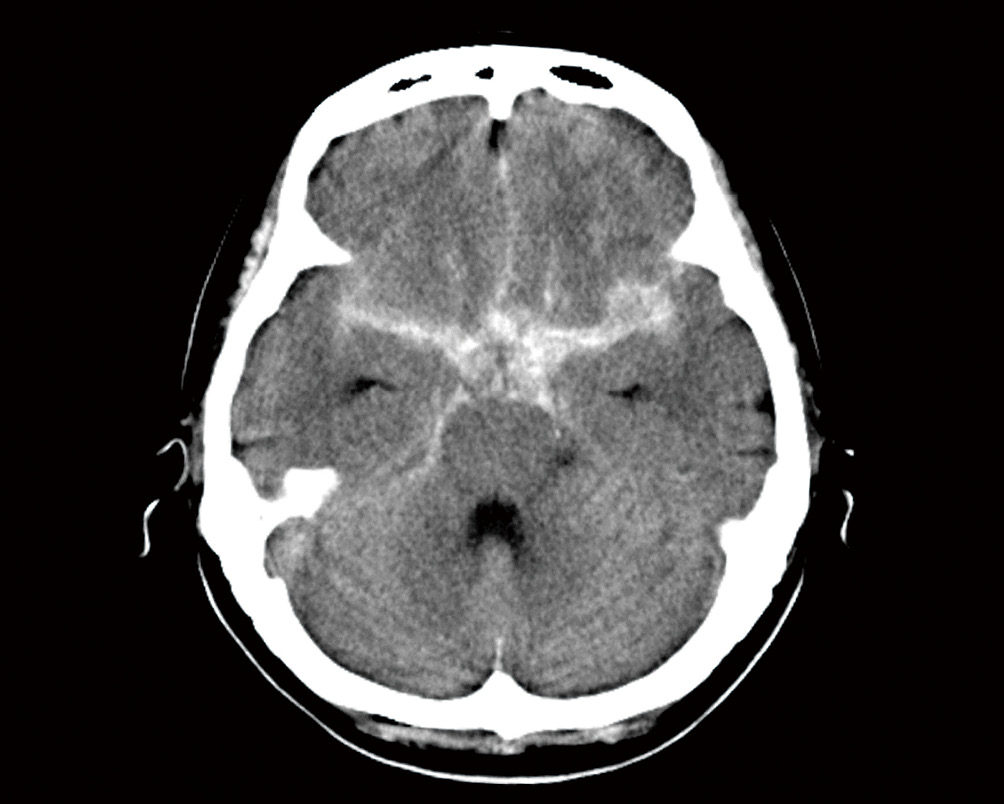
A 48-year-old woman presented with sudden headache. Computed tomography (CT) revealed subarachnoid hemorrhage (SAH) in the basal cistern (Fig. 1). Three-dimensional CT angiography has demonstrated an aneurysm with a major diameter of 2.8 mm, which was located at the bifurcation where the anomalous artery, running along with the left pericallosal artery, originated from the A1 segment of the left ACA (Fig. 2A). The diameter of the left pericallosal artery was noted to be smaller than that of the contralateral pericallosal artery (Fig. 2B). The patient underwent left frontotemporal craniotomy under general anesthesia. Intraoperatively, an aneurysm was confirmed at the bifurcation where the anomalous artery, running toward the interhemispheric fissure, arose from the A1 segment. The aneurysm projected downward and was attached to the left optic nerve (Fig. 3). During aneurysm clipping, absence of perforating arteries originating from the arterial wall around the aneurysm was confirmed.
Postoperative CT angiography confirmed resolution of the aneurysm. Angiography via arterial catheterization demonstrated that the anomalous artery branched into the frontopolar artery and the fronto-orbital artery and terminated as the anterior internal frontal arteries (Fig. 4). The patient's postoperative course was deemed uneventful.
Discussion
The CMA courses in or near the cingulate sulcus, runs parallel to the pericallosal artery, and gives rise to two or more cortical branches.13,14) The artery in this present case was observed to be consistent with the above characteristics of the CMA, and the usual CMA originating from the A2, A3, or A4 segments of the ACA was absent. Thus, this present case was considered to have an anomalous CMA arising from the A1 segment of the ACA. This type of anomalous CMA has only rarely been reported.11,12) Development of the ACA generally begins at around 30 days of embryonic life.15) During the next 20 days, the ACA courses upward between the bilateral expanding cerebral hemispheres, followed by the development of cortical arteries.15) In this present case, the CMA might not have developed normally from the A3 segment for unknown reasons, resulting in the development of the anomalous CMA arising from the A1 segment.
A variant similar to that seen in the present case is the type 3 artery of the persistent primitive olfactory artery (PPOA). The type 3 artery of the PPOA arises from the A1 segment of the ACA and supplies the territory of the distal ACA, as it runs along the olfactory tract and makes a unique hairpin bend.16,17) This present case also had the former two features, although the latter two features differed from the anomaly in this present case.
A previous investigator reported a patient with intracranial hemorrhage due to a ruptured anteriorly directed aneurysm that formed at the origin of an anomalous CMA arising from the A1 segment.11) Our patient, however, suffered SAH due to a ruptured downward-facing aneurysm that formed at the origin of the anomalous CMA. Development of aneurysms in such locations has been reportedly associated with local hemodynamic stress2,3,10-12) and weakness of the arterial wall.12)
Saccular aneurysms of the A1 segment are divided into the following three types according to their site of occurrence: type 1, at the origin of a perforator arising from the A1 segment; type 2, proximal to the A1 fenestration; and type 3, at the end of the hairpin-curved A1 segment without branching arteries (with the A1 segment showing marked elongation and kinking).3) Aneurysms occurring at the bifurcation of a cortical artery arising from the A1 segment have not been classified, indicating that this type of aneurysm is rare.3)
Perforating arteries usually arise from the superior and/or posterior aspect of the A1 segment and run directly to the anterior perforating substance.18) Type 1 aneurysms typically project superiorly and/or posteriorly. Therefore, when type 1 aneurysms are clipped, separation of the perforating arteries from the neck or dome of the aneurysm is required.5,7) In contrast, when the aneurysm anatomically projects downward, as in this present case, it might be unrelated to the origin or course of the perforating arteries; hence, easy clipping of the aneurysm can be performed.
Acknowledgments
The author would like to thank the patient and her family for their cooperation.
Conflicts of Interest Disclosure
The author declares no conflict of interest.
References
- 1) Kassell NF, Torner JC: Size of intracranial aneurysms. Neurosurgery 12: 291-297, 1983
- 2) Wakabayashi T, Tamaki N, Yamashita H, Saya H, Suyama T, Matsumoto S: Angiographic classification of aneurysms of the horizontal segment of the anterior cerebral artery. Surg Neurol 24: 31-34, 1985
- 3) Suzuki M, Onuma T, Sakurai Y, Mizoi K, Ogawa A, Yoshimoto T: Aneurysms arising from the proximal (A1) segment of the anterior cerebral artery. A study of 38 cases. J Neurosurg 76: 455-458, 1992
- 4) Wanibuchi M, Kurokawa Y, Ishiguro M, Fujishige M, Inaba K: Characteristics of aneurysms arising from the horizontal portion of the anterior cerebral artery. Surg Neurol 55: 148-155, 2001
- 5) Yilmaz M, Kalemci O, Yurt A, Durmaz MO, Arda NM: Treatment of aneurysms arising from the proximal (A1) segment of the anterior cerebral artery. Bosn J Basic Med Sci 14: 8-11, 2014
- 6) Marinković S, Milisavljević M, Kovacević M: Anatomical bases for surgical approach to the initial segment of the anterior cerebral artery. Microanatomy of Heubner's artery and perforating branches of the anterior cerebral artery. Surg Radiol Anat 8: 7-18, 1986
- 7) Hino A, Fujimoto M, Iwamoto Y, Oka H, Echigo T: Surgery of proximal anterior cerebral artery aneurysms. Acta Neurochir (Wien) 144: 1291-1296, 2002
- 8) Hong SK: Ruptured proximal anterior cerebral artery (A1) aneurysm located at an anomalous branching of the fronto-orbital artery--a case report. J Korean Med Sci 12: 576-580, 1997
- 9) Lee ER, Eastwood JD: An unusual variant of the fronto-orbital artery. AJNR Am J Neuroradiol 21: 939-940, 2000
- 10) Aso K, Kashimura H, Takeda M, Chida K: An unusual variant of the common trunk of the fronto-orbital and frontopolar arteries associated with a ruptured aneurysm of the A1 segment of the anterior cerebral artery. Surg Neurol Int 6: S418-S420, 2015
- 11) Krishnamoorthy T, Gupta AK, Bhattacharya RN, Rajesh BJ, Purkayastha S: Anomalous origin of the callosomarginal artery from the A1 segment with an associated saccular aneurysm. AJNR Am J Neuroradiol 27: 2075-2077, 2006
- 12) Yoshida J, Kashimura H, Takeda M, Aso K: An unusual variant of the callosomarginal artery from the A1 segment of the anterior cerebral artery. Surg Neurol Int 7: S402-S404, 2016
- 13) Perlmutter D, Rhoton AL: Microsurgical anatomy of the distal anterior cerebral artery. J Neurosurg 49: 204-208, 1978
- 14) Rhoton AL Jr: The supratentorial arteries. Neurosurgery 51: 53-120, 2002
- 15) Bertulli L, Robert T: Embryological development of the human cranio-facial arterial system: a pictorial review. Surg Radiol Anat 43: 961-973, 2021
- 16) Horie N, Morikawa M, Fukuda S, Hayashi K, Suyama K, Nagata I: New variant of persistent primitive olfactory artery associated with a ruptured aneurysm. J Neurosurg 117: 26-28, 2012
- 17) Sato Y, Kashimura H, Takeda M, Chida K, Kubo Y, Ogasawara K: Aneurysm of the A1 segment of the anterior cerebral artery associated with the persistent primitive olfactory artery. World Neurosurg 84: 7-9, 2015
- 18) Rosner SS, Rhoton AL, Ono M, Barry M: Microsurgical anatomy of the anterior perforating arteries. J Neurosurg 61: 468-485, 1984