Abstract
Transforaminal full-endoscopic spine surgery (TF-FESS) is a novel minimally invasive spine surgery that requires only an 8-mm skin incision and causes minimal damage to the paravertebral muscles. To perform TF-FESS safely and efficiently, preoperative planning is quite important as the intervention requires anatomical understanding and high technical skills. Recently, three-dimensional (3D) printing has become a useful tool in various surgeries, and several studies have addressed its efficacy; however, there are no reports on the application of 3D printing to FESS. In this study, we present two cases of severe lumbar deformities for which preoperative 3D printing was useful. The 3D printing enabled the surgeons to visualize and plan the drilling of the superior articular process for a successful foraminoplasty at a low cost. The manufacturing equipment cost about USD 900 and is able to produce an actual-size model at a cost of less than USD 10 per patient. In conclusion, preoperative planning using 3D printing should be adopted to safely perform FESS.
Introduction
In recent years, minimally invasive surgery with endoscopy has undergone major developments. One type of minimally invasive spinal surgery currently in use is transforaminal full-endoscopic spine surgery (TF-FESS),1,2) which requires only an 8-mm skin incision and causes less damage to the paravertebral muscles.3) TF-FESS can be performed under local anesthesia, which allows for spine surgery in elderly patients with poor general condition and can prevent severe nerve damage because the patients are awake.4,5) In the first decade, TF-FESS was initially indicated for the removal of herniated nucleus pulposus.6) With the invention of an ultra-thin high-speed surgical drill, surgical options and techniques have advanced in recent years. Using the high-speed drill technique, transforaminal full-endoscopic lumbar foraminoplasty (TF-FELF) has been successfully performed.6)
Despite these benefits, TF-FESS demands a high level of skill because the surgical working space is limited compared with other common spine surgeries, and access to the spinal canal is difficult in patients with severe spinal deformity. Therefore, surgery under local anesthesia should be performed as quickly as possible.
Adequate preoperative planning can favor the achievement of successful TF-FELF. Three-dimensional (3D) printing is becoming one of the latest tools in orthopedic surgery.7-10) In the field of the spinal surgery, in particular, 3D printing has been used for cases of deformity,11) pediatrics,1) tumor,12) and fusion surgery.11) However, there is no report on the application of 3D models to FESS.
In this study, we report two patients who underwent TF-FELF, in which an actual-size 3D printing model was useful for the surgery.
This study was approved by the ethics board of Tokushima Prefectural Miyoshi Hospital. Informed consent was obtained from all patients, and patients' information was anonymized and de-identified before analysis.
Case Report
Case 1
The patient was a 59-year-old man who presented to our institution with continuous low back pain and numbness of the right lower limb. He had undergone two lumbar decompression surgeries at the L4-L5 level 20 years beforehand. He had numbness in the right L4 dermatome and a positive finding on the right femoral nerve stretching test. The manual muscle test was within the normal range. Plain X-ray revealed severe lumbar deformity (Fig. 1A, B), and magnetic resonance imaging (MRI) and computed tomography (CT) showed severe foraminal stenosis at the right L4-L5 level (Figs. 1C, D and 2A, B). Immediate pain relief and pain reproduction were confirmed by a selective nerve root block of the right L4. Based on these findings, the diagnosis was right L4 radiculopathy caused by lumbar foraminal stenosis at L4-L5.

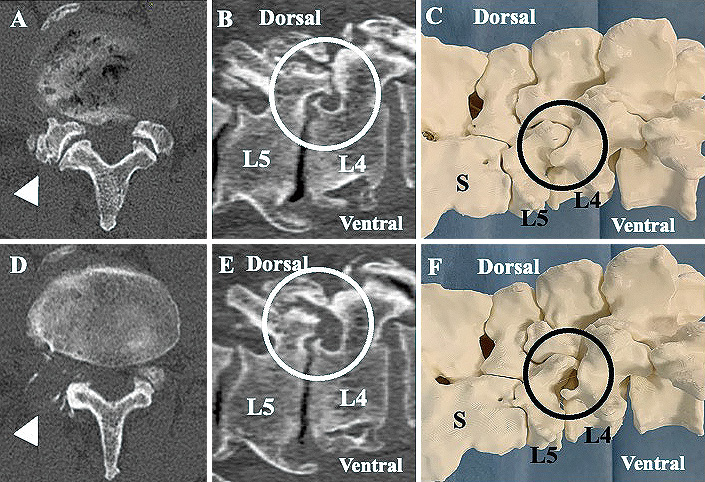
TF-FELF was planned for this patient. In FELF, the superior articular process (SAP) was shaved by a high-speed bar using the transforaminal approach.6) Because the lumbar deformity and osteophytes contributed to severe foraminal and spinal canal stenosis, we employed 3D printing for preoperative planning (Fig. 2C). The 3D printing model was generated using raw imaging data of 1.0-mm slice of CT scan (Aquilion ONE, TOSHIBA MEDICAL SYSTEMS CORPORATION). The fused filament fabrication/fused deposition modeling (FFF/FDM) technique is employed, and acrylonitrile butadiene styrene (ABS) filament is used as the material. An actual-size model of the patient's lumbar spine enabled us to visualize the lumbar deformity in detail and to simulate the placement of the cannula for endoscopy and the scheduled extent of the SAP shaving.
The patient underwent TF-FELF with local anesthesia. During the surgery, the 3D printing models were placed outside of the sterile field, and anatomy was checked during the surgery. Using the outside-in technique, after partial removal of the SAP of L5 and the osteophytes around the accessory process of L4, the L4 nerve root was decompressed with foraminoplasty. Immediately after the surgery, the patient's right-leg pain and numbness improved. Postoperative CT (Fig. 2D, E) revealed an enlarged foramen of L4-L5. We confirmed the extent of the bone shaving using postoperative 3D printing (Fig. 2F).
Case 2
The second case was a 75-year-old woman who underwent lumbar laminectomy at L3-L4, L4-L5, and L5-S1 for lumbar spinal stenosis 1 year before. Although she had an uneventful course with no complications, she developed right-leg pain and numbness 4 months after the surgery. Plain X-ray (Fig. 3A, B), MRI (Fig. 3C, D), and CT (Fig. 4A, B) revealed severe deformity and osseous foraminal stenosis caused by osteophytes of the L5-S facet joints, which resulted in right L5 nerve root radiculopathy.

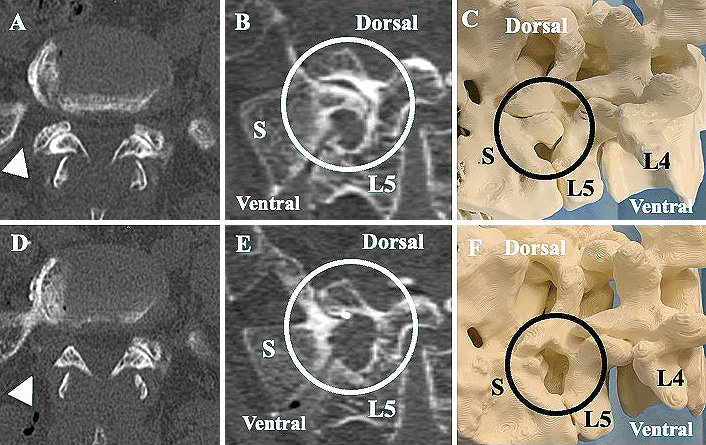
The patient underwent TF-FELF under local anesthesia. The transforaminal approach at L5-S is typically difficult as the iliac crest interferes with the cannula placement.2,6) Therefore, 3D printing was created using the same method as in case 1 and used to elucidate the positional relationship between the lumbar spine and iliac crest. Using preoperative 3D printing, we simulated the cannula insertion and the area for shaving of the SAP of S1 (Fig. 4C). Using the outside-in technique, the SAP of S1 and the sacral alar were partially removed, the L5-S foramen was enlarged, and the L5 nerve root was decompressed. The patient's leg pain and numbness improved immediately after the surgery. Postoperative CT scans revealed foraminal enlargement (Fig. 4D, E), and the postoperative 3D printing model clearly showed that the extent of the bone shaving matched that of the preoperative plan (Fig. 4F).
Discussion
TF-FESS is usually feasible with only an 8-mm skin incision and minimal damage to the paravertebral muscles under local anesthesia and is currently the least-invasive spinal surgery. However, compared with other surgeries performed under general anesthesia, the surgeons are forced to perform all steps of the procedure quickly and smoothly as the patient is awake during the surgery. To perform TF-FELF for foraminal stenosis, foraminoplasty is required, during which the intervertebral foramen of the lumbar spine is enlarged using a high-speed trephine drill.6) In particular, for patients with severe spinal deformity or proliferative fibro-osseous changes around the facet joint, TF-FELF is highly technically demanding.
Ahn et al. categorized the applications of 3D models in spine surgery into four categories: surgical planning, patient-specific guides for instrumentation, patient-specific implants, and education.9) For surgical planning, 3D printing provides better understanding of complex spinal deformities.9,11,13,14) The present cases in which FELF was performed are re-operation case or high-iliac L5-S cases, in which 3D printing was useful for planning the cannula approach and the shaving extent of the SAP. Transforaminal approach of the L5-S and L4-L5 level with high iliac crest, which interferes with the cannula placement, is difficult,6) and 3D printings could be useful. In re-operative case, the anatomy of the lumbar spine is more complicated than the virgin lumbar; furthermore, the use of 3D printings is recommended. Sakai et al. reported a pediatric patient with os odontoideum who was successfully treated with the aid of surgical planning using a preoperative 3D printing model.1) Zhao et al. reported that 3D printing was used pre-operatively to calculate the angle for the insertion of percutaneous tubular retractors.15)
The average operating time in the present cases is 61.5 min. Takeuchi et al. reported that the average operating time in TF-FESS is about 73.2-75.7 min.3) Taken together, the operating time could be reduced by using accurate preoperative planning with a 3D model.
3D printing is generally created by adding a chosen material layer by layer. There are three commonly used methods: fused filament fabrication/fused deposition modeling (FFF/FDM), selective laser sintering (SLS), and stereolithography (SLA). In FFF/FDM, layers are made by depositing a heat-softened polymer by a computer-controlled extrusion nozzle, SLS involves a focused energy source (such as an electron beam or a laser) acting upon a fine powder bed of varied materials, and SLA uses a light curable resin, on which an optical light energy source works.16) FFF/FDM 3D printers are fast and cost effective but commonly use materials with a low melting point, which cannot withstand sterilization. Our 3D printer is FFF/FDM, and we use the 3D printings for preoperative planning and intraoperative anatomical conformation by placing those 3D printing models outside of the sterile field.
Currently, the manufacturing equipment for 3D models is not particularly expensive. The system that we use cost less than USD 1,000 and is able to produce an actual-size model at a cost of less than USD 10 per patient. In addition, the material that we used in the 3D printer for the presented cases, namely, ABS filament, can be sterilized. Taken together, 3D printing is useful from both economic and medical perspectives.
We reported two cases of FESS performed for severe spinal deformity that benefited from the use of 3D printing. Preoperative planning using 3D printing should be adopted to improve the safety of FESS.
Conflicts of Interest Disclosure
All authors have no conflict of interest.
References
- 1) Sakai T, Tezuka F, Abe M, et al.: Pediatric patient with incidental Os odontoideum safely treated with posterior fixation using rod-hook system and preoperative planning using 3D printer: a case report. J Neurol Surg A Cent Eur Neurosurg 78: 306-309, 2017
- 2) Yoshinari H, Tezuka F, Yamashita K, et al.: Transforaminal full-endoscopic lumbar discectomy under local anesthesia in awake and aware conditions: the inside-out and outside-in techniques. Curr Rev Musculoskelet Med 12: 311-317, 2019
- 3) Takeuchi M, Yamashita K, Hashimoto A, et al.: Return to the original work activity following the full-endoscopic lumbar surgery under the local anesthesia. Neurol Med Chir (Tokyo) 61: 144-151, 2021
- 4) Kitahama Y, Sairyo K, Dezawa A: Percutaneous endoscopic transforaminal approach to decompress the lateral recess in an elderly patient with spinal canal stenosis, herniated nucleus pulposus and pulmonary comorbidities. Asian J Endosc Surg 6: 130-133, 2013
- 5) Sairyo K, Egawa H, Matsuura T, et al.: State of the art: transforaminal approach for percutaneous endoscopic lumbar discectomy under local anesthesia. J Med Invest 61: 217-225, 2014
- 6) Sairyo K, Chikawa T, Nagamachi A: State-of-the-art transforaminal percutaneous endoscopic lumbar surgery under local anesthesia: discectomy, foraminoplasty, and ventral facetectomy. J Orthop Sci 23: 229-236, 2018
- 7) Kim JW, Lee Y, Seo J, et al.: Clinical experience with three-dimensional printing techniques in orthopedic trauma. J Orthop Sci 23: 383-388, 2018
- 8) Fadero PE, Shah M: Three dimensional (3D) modelling and surgical planning in trauma and orthopaedics. Surgeon 12: 328-333, 2014
- 9) Ahn J, Sheha ED, Gandhi SD, Colman MW: Three-dimensional printing and models: current applications, limitations, and trends in spinal surgery. Semin Spine Surg 32: 100790, 2020
- 10) Kamishina H, Sugawara T, Nakata K, et al.: Clinical application of 3D printing technology to the surgical treatment of atlantoaxial subluxation in small breed dogs. PLoS One 14: e0216445, 2019
- 11) Garg B, Mehta N: Current status of 3D printing in spine surgery. J Clin Orthop Trauma 9: 218-225, 2018
- 12) Xiao JR, Huang WD, Yang XH, et al.: En bloc resection of primary malignant bone tumor in the cervical spine based on 3-dimensional printing technology. Orthop Surg 8: 171-178, 2016
- 13) Yang M, Li C, Li Y, et al.: Application of 3D rapid prototyping technology in posterior corrective surgery for Lenke 1 adolescent idiopathic scoliosis patients. Medicine (Baltimore) 94: e582, 2015
- 14) Yamaguchi JT, Hsu WK: Three-dimensional printing in minimally invasive spine surgery. Curr Rev Musculoskelet Med 12: 425-435, 2019
- 15) Zhao W, Shen C, Cai R, et al.: Minimally invasive surgery for resection of ossification of the ligamentum flavum in the thoracic spine. Wideochir Inne Tech Maloinwazyjne 12: 96-105, 2017
- 16) Tong Y, Kaplan DJ, Spivak JM, Bendo JA: Three-dimensional printing in spine surgery: a review of current applications. Spine J 20: 833-846, 2020