Abstract
Lumbar spondylolysis is commonly recognized at a single-level of the lumbar spine and frequently affects the L5 pars interarticularis unilaterally or bilaterally. Some reports have described multiple-level spondylolysis, most cases of which occur at consecutive lumbar segments. We herein present a rare case of lumbar spondylolysis involving nonconsecutive multiple-level segments; only eight such cases have been reported previously. A 38-year-old man presented with a 10-month history of chronic severe low back pain. Lumbar flexion–extension radiographs and computed tomography revealed spondylolysis at the level of L3 and L5, whereas no spondylolisthesis was present and the intervertebral disc spaces were maintained at all levels. Because 6 months of conservative management failed and repeated diagnostic blocks confirmed that the fracture of the L3 pars interarticularis was generating pain, repair of the bilateral L3 pars interarticularis with the smiley face rod method was performed. At the last follow-up 1 year after surgery, the patient had resumed normal life as a laborer and reported no back pain.
Introduction
Lumbar spondylolysis is caused by repetitive stress of the pars interarticularis with subsequent microfracture which may lead to bony defect or spondylolisthesis.1,2) It is usually recognized at a single level in the lumbar spine and frequently affects the L5 pars interarticularis unilaterally or bilaterally.1,2) Some reports have described multiple-level spondylolysis, most cases of which are located at consecutive lumbar segments.3–8) Non-consecutive multiple-level spondylolysis affecting the lumbar spine is rare; to our knowledge, only eight such cases have been documented in the literature (Table 1).1,8–12) We herein describe a 38-year-old man with noncontiguous multiple-level spondylolysis at L3 and L5 that was successfully treated with single-level repair of the pars interarticularis at L3. The preoperative management and surgical strategy used for this patient are discussed.
Table 1
Reported cases of nonconsecutive lumbar spondylolysis
| Authors |
Age/sex |
Physical activity |
Symptom |
Level |
Treatment |
| Ravichandran (1980) |
33/M |
Rugby player |
LBP + bilateral leg pain |
L3 + L5 |
Intertransverse fusion of L2–L4 |
| 43/M |
Manual labor |
LBP + right leg pain |
L2 + L4 |
Repair of L2 by Buck method + L4–S1 interspinous fusion |
| Ranawat et al. (2003) |
N/A |
Cricket player |
N/A |
L1 + L3 + L5 |
Repair of L5 by screw placement into the defects |
| Chung et al. (2007) |
20/M |
N/A |
N/A |
L3 + L5 |
Repair of L3 + L5 by screw and hook method |
| 20/M |
N/A |
N/A |
L3 + L5 |
Repair of L3 + L5 by screw and hook method |
| Nayeemuddin et al. (2011) |
16/M |
Football player |
LBP |
L3 + L5 |
Conservative treatment |
| Elgafy et al. (2015) |
18/M |
Baseball player |
LBP |
L2 + L5 |
Repair of L2 by screw and hook method |
| Voisin et al. (2018) |
50/M |
N/A |
LBP + right leg paresthesia |
L3 + L5 |
Repair of L3 + L5 by smiley face rod method |
| Present case |
38/M |
Manual labor |
LBP |
L3 + L5 |
Repair of L3 by smiley face rod method |
M: male, Age is presented in years, LBP: Low back pain.
Case Report
An otherwise healthy 38-year-old man working as a manual laborer presented with a 10-month history of chronic severe low back pain. Conservative treatment including administration of nonsteroidal anti-inflammatory drugs and use of an orthosis had been conducted by his home doctor for the previous 6 months, but this treatment was unsuccessful. At the presentation neurological examination revealed no motor weakness or sensory disturbance in the bilateral lower extremities. Dynamic lumbar radiographs showed no spondylolisthesis, and the intervertebral disc spaces were maintained at all levels; however, spondylolysis at L3 and L5 was suspected (Figs. 1A and 1B). Lumbar magnetic resonance imaging (MRI) revealed degeneration of the L3/4 and L5/S1 discs (Fig. 1C). A computed tomography (CT) scan confirmed bilateral defects with marginal sclerosis at the pars interarticularis of L3 and L5 with mild spinal canal stenosis and no foraminal stenosis. Additionally, osteophyte formation was observed around the L3 but not L5 pars interarticularis (Figs. 2A–2E). Based on this finding, we speculated that unstable micromovement around the L3 pars interarticularis had caused the low back pain. To confirm this speculation and relieve the patient’s severe back pain, the fracture of the L3 pars interarticularis was injected with lidocaine and steroids under fluoroscopic guidance. Immediately after injection, the patient reported pain relief, which lasted for several weeks. One month after the injection, the pars interarticularis was injected again because of recurrent severe lumbago. At this time, the fracture of the L5 pars interarticularis was injected for confirmation, but this injection resulted in no pain relief. Therefore, the L3 pars interarticularis was injected, resulting in immediate pain relief. Because 6 months of conservative management failed and the diagnostic block indicated that the fracture of the L3 pars interarticularis was generating the pain, surgical treatment was recommended for the L3 pars interarticularis.

Although MRI revealed slight degeneration of the L3/4 disc (Fig. 1C), bilateral repair of the L3 pars interarticularis rather than L3/4 fusion surgery was indicated because the radiographic findings demonstrated no spondylolisthesis and maintenance of both the intervertebral disc spaces and mobility of L3/4 (Figs. 1A and 1B).
Surgery
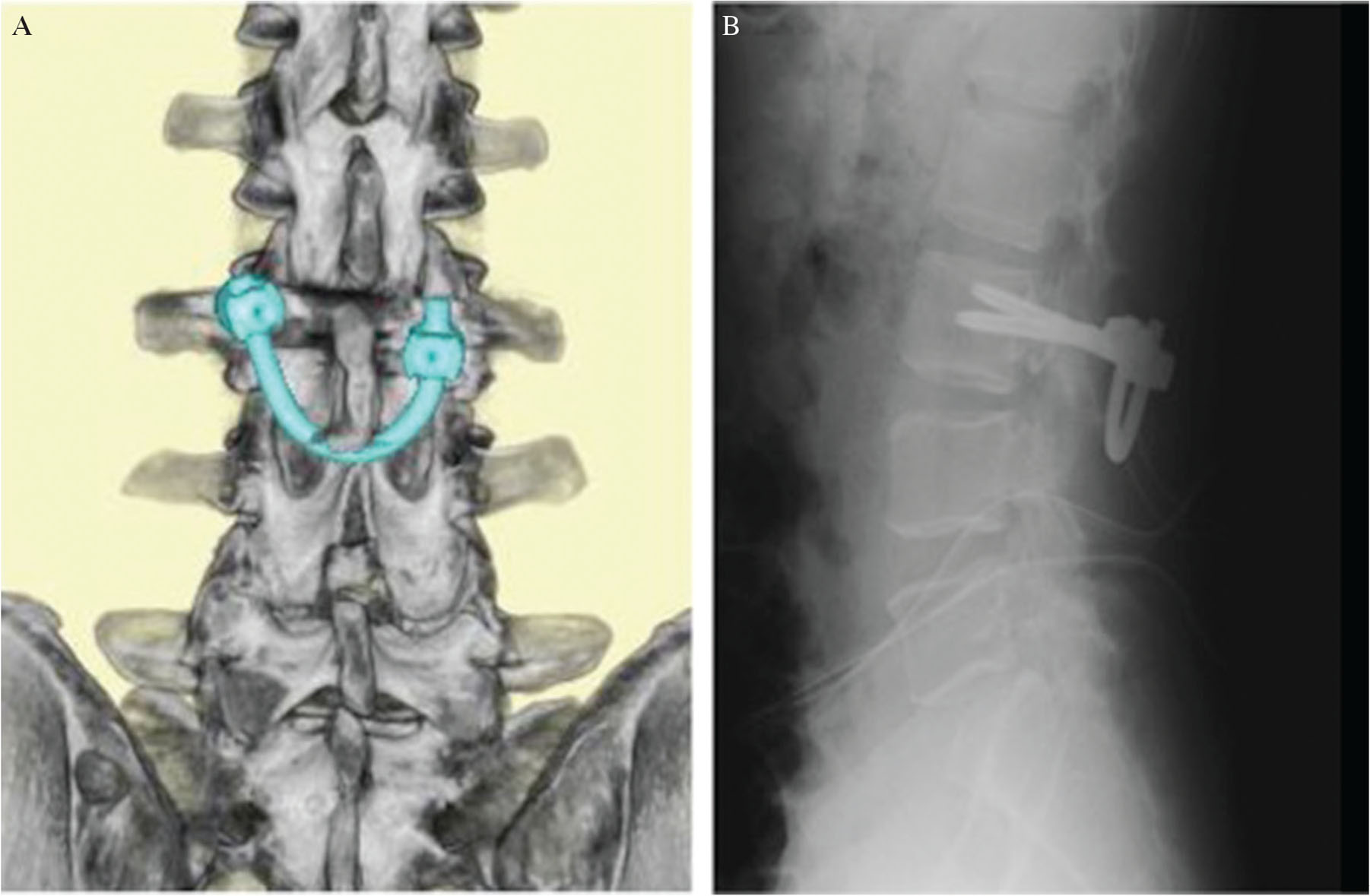
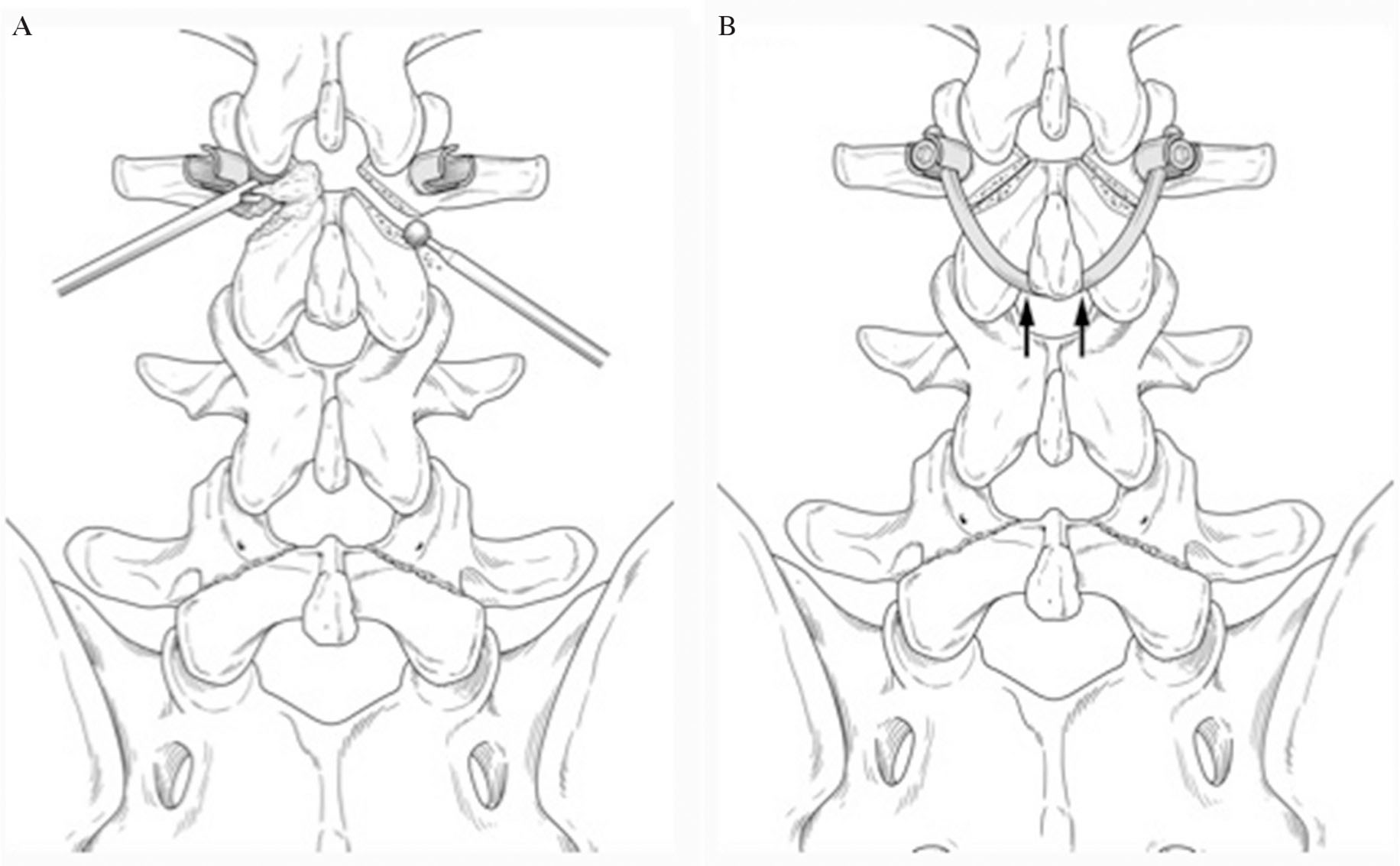
Of several reported methods of direct repair, the smiley face rod method was adopted.13) A 7-cm midline skin incision was made, and the paraspinal musculature was retracted laterally to expose the bilateral L3 lamina, pars interarticularis, and transverse process. Using anatomic landmarks and fluoroscopic guidance, a starting hole for the pedicle screw was burred, the hole was tapped, and bilateral multiaxial pedicle screws were inserted (Fig. 3A). The pars interarticularis defect and osteophyte around it were exposed. Using a diamond surgical bur and curette, the osteophyte and synovium of the pseudarthrotic part of the spondylolytic segment was removed to refresh the defects. Cancellous bone was harvested from the iliac crest and placed in the defect before screw insertion. A 100-mm-long rod was bent to fit and placed immediately caudal to the L3 spinous process. The loose lamina was fixed more firmly after the bent rod was bumped against the spinous process using a rod pusher (Fig. 3B). Cancellous bone was implanted into the pars defects (Figs. 4A and 4B).
The patient’s post-operative course was uneventful, and his symptoms improved immediately. He was allowed to stand and walk 2 days after the surgery with a hard brace, and he resumed his work as a laborer 1 month after surgery. Six months postoperatively, the patient reported no back pain, and advanced activity was tolerated without problems.
Discussion
Lumbar spondylolysis most commonly occurs at a single spinal level and usually responds well to conservative treatment; however, some patients’ symptoms do not improve and require surgical intervention.1,2) The main surgical methods are posterolateral arthrodesis and direct repair. Posterolateral arthrodesis of the posterior elements has been commonly performed for years. However, a disadvantage is loss of motion at the affected segment, which increases loading on the adjacent segment.14) Direct repair has the advantage of preserving the segmental motion, which is preferred in younger patients without severe disc degeneration or instability. Several methods of direct repair have been reported to date. In 1968, Kimura15) first reported pars interarticularis repair without instrumentation; however this technique had a disadvantage in that prolonged bed rest and immobilization were required. In 1970, Buck16) reported fixation of the pars with a screw across the pars defect. Proper placement of screws was subsequently considered to be technically difficult. The wiring method, a procedure used to stabilize the loose posterior arch with wire, was described in 1992. However, this technique also had a shortcoming in that placement of the wires under the transverse process was difficult and caused significant bleeding.17) In 2005, Roca et al.18) introduced the pedicle screw and hook method, a procedure used to compress pars defects with pedicle screws and angled lamina hooks. Good clinical and biomechanical results have been reported by this method; however, the surgical results of this method were significantly better among patients ≤20 years than ≥21 years of age.18) In the present study, we repaired the pars interarticularis with the smiley face rod method. This method was first reported in 1999 by Gillet and Petit,19) who called it the “V-rod method.” The screw head and rod resemble a smiley face on the anteroposterior plain radiograph; thus, this technique came to be known as the “smiley face rod method.”13) Ulibarri et al.20) reported that biomechanical evaluation of this method showed excellent stability of a spondylolytic defect in comparison with other types of direct repair surgery.
The incidence of the spondylolysis varies according to race. Previous studies have shown the lowest incidence (1–2%) in the African population and the highest incidence (about 50%) in the Inuit population.21,22) An incidence of about 6% has been reported in the Asian population.21,22)
As for multiple-level spondylolysis, 0.3–5.6% of the incidence have been reported, and most such cases involve consecutive lumbar segments.3,5,8)
Multiple-level spondylolysis has also been reported to be more often seen among men than women, and most cases are associated with sports, trauma and heavy labor.3–9) Therefore, similar to single-level spondylolysis, the mechanical factor is considered to play a decisive role for pathogenesis of multiple-level spondylolysis.9) Despite the fact that single-level pars defects respond well to conservative treatment, conservative measures for multiple-level spondylolysis patients often fail and surgery is frequently required.3,6,8)
In patients with multiple-level spondylolysis without spondylolisthesis, satisfactory surgical results of direct repair of pars interarticularis and posterolateral arthrodesis have been reported.10)
Only eight previous cases of nonconsecutive multiple-level lumbar spondylolysis have been reported (Table 1).1,8–12) Of these eight cases, pars fractures were recognized at L3 and L5 in five patients. All seven patients whose sex was confirmed were male and all five patients whose physical activity was confirmed were athletes, supporting the notion that mechanical factors are also a main contributor to the pathogenesis of nonconsecutive multiple-level lumbar spondylolysis. Conservative treatment was successful in one patient,11) but surgical treatment was performed in the other seven patients because of failed conservative treatment.1,8–10,12) Of these seven surgically treated patients, intertransverse fusion was performed for one patient6) and direct pars repair using a screw and hook system was performed for three patients.9,10) As described above, the smiley face rod method was used for our patient because he was 38 years old and previous reports have indicated excellent stability of spondylolytic defects when using this method in comparison with other direct repair surgeries.20) Furthermore, Voisin et al.12) recently reported good surgical results of the smiley face rod method in a 50-year-old patient with L3 and L5 spondylolysis.
Previous researchers have recommended that the pain source should routinely be confirmed before surgery by infiltration of a local anesthetic in the defects.23,24) We performed repeated blocks for the pars interarticularis to isolate the symptomatic level in our patient with nonconsecutive lumbar spondylolysis. Furthermore, Elgafy et al.9) isolated the symptomatic level using both a block for the pars interarticularis and SPECT scan, and repair of the pars interarticularis was performed only for the symptomatic level. Increased radionuclide uptake within the pars indicates a stress reaction and possibly a more acute pathology; this is therefore considered to be a useful test for a more accurate diagnosis.25)
The upper lumbar spine was symptomatic in both our case and that described by Elgafy et al.9) In addition, patients with multiple-level spondylolysis usually develop spondylolisthesis at L4 and L5 (mostly at L4). In contrast, single-level isthmic spondylolisthesis most commonly occurs at L5.26) The upper level might be likely to become symptomatic in such cases; however, accumulation of more cases of symptomatic consecutive or nonconsecutive multiple-level spondylolysis with confirmation of the symptomatic levels is necessary to confirm this.
In conclusion, we have described a rare case of nonconsecutive spondylolysis successfully treated with primary repair of a single level using the smiley face rod method. This case report emphasizes the importance of preoperative examination including repeated blocks for the pars interarticularis to identify the symptomatic level.
Acknowledgment
We thank Angela Morben, DVM, ELS, from Edanz Group (www.edanzediting.com/ac), for editing a draft of this manuscript.
Conflicts of Interest Disclosure
The authors declare that they have no conflicts of interest.
References
- 1) Ranawat VS, Dowell JK, Heywood-Waddington MB: Stress fractures of the lumbar pars interarticularis in athletes: a review based on long-term results of 18 professional cricketers. Injury 34: 915–919, 2003
- 2) Standaert CJ, Herring SA: Spondylolysis: a critical review. Br J Sports Med 34: 415–422, 2000
- 3) Al-Sebai MW, Al-Khawashki H: Spondyloptosis and multiple-level spondylolysis. Eur Spine J 8: 75–77, 1999
- 4) Chang JH, Lee CH, Wu SS, Lin LC: Management of multiple level spondylolysis of the lumbar spine in young males: a report of six cases. J Formos Med Assoc 100: 497–502, 2001
- 5) Eingorn D, Pizzutillo PD: Pars interarticularis fusion of multiple levels of lumbar spondylolysis. A case report. Spine 10: 250–252, 1985
- 6) Nozawa S, Shimizu K, Miyamoto K, Tanaka M: Repair of pars interarticularis defect by segmental wire fixation in young athletes with spondylolysis. Am J Sports Med 31: 359–364, 2003
- 7) Ogawa H, Nishimoto H, Hosoe H, Suzuki N, Kanamori Y, Shimizu K: Clinical outcome after segmental wire fixation and bone grafting for repair of the defects in multiple level lumbar spondylolysis. J Spinal Disord Tech 20: 521–525, 2007
- 8) Ravichandran G: Multiple lumbar spondylolyses. Spine (Phila Pa 1976) 5: 552–557, 1980
- 9) Elgafy H, Hart RC, Tanios M: Nonconsecutive pars interarticularis defects. Am J Orthop (Belle Mead NJ) 44: E526–E529, 2015
- 10) Chung CH, Chiu HM, Wang SJ, Hsu SY, Wei YS: Direct repair of multiple levels lumbar spondylolysis by pedicle screw laminar hook and bone grafting: clinical, CT, and MRI-assessed study. J Spinal Disord Tech 20: 399–402, 2007
- 11) Nayeemuddin M, Richards PJ, Ahmed EB: The imaging and management of nonconsecutive pars interarticularis defects: a case report and review of literature. Spine J 11: 1157–1163, 2011
- 12) Voisin MR, Witiw CD, Deorajh R, et al.: Multilevel spondylolysis repair using the “smiley face” technique with 3-dimensional intraoperative spinal navigation. World Neurosurg 109: e609–e614, 2018
- 13) Yamashita K, Higashino K, Sakai T: The reduction and direct repair of isthmic spondylolisthesis using the smiley face rod method in adolescent athlete: technical note. J Med Invest 64: 168–172, 2017
- 14) Ghiselli G, Wang JC, Bhatia NN, Hsu WK, Dawson EG: Adjacent segment degeneration in the lumbar spine. J Bone Joint Surg Am 86-A: 1497–1503, 2004
- 15) Kimura M: My method of filing the lesion with spongy bone in spondylolysis and spondylolistesis. Seikei Geka 19: 285–296, 1968 (Japanese)
- 16) Buck JE: Direct repair of the defect in spondylolisthesis. Preliminary report. J Bone Joint Surg Br 52: 432–437, 1970
- 17) Johnson GV, Thompson AG: The Scott wiring technique for direct repair of lumbar spondylolysis. J Bone Joint Surg Br 74: 426–430, 1992
- 18) Roca J, Iborra M, Cavanilles-Walker JM, Albertí G: Direct repair of spondylolysis using a new pedicle screw hook fixation: clinical and CT-assessed study: an analysis of 19 patients. J Spinal Disord Tech 18 Suppl: S82–S89, 2005
- 19) Gillet P, Petit M: Direct repair of spondylolysis without spondylolisthesis, using a rod-screw construct and bone grafting of the pars defect. Spine (Phila Pa 1976) 24: 1252–1256, 1999
- 20) Ulibarri JA, Anderson PA, Escarcega T, Mann D, Noonan KJ: Biomechanical and clinical evaluation of a novel technique for surgical repair of spondylolysis in adolescents. Spine (Phila Pa 1976) 31: 2067–2072, 2006
- 21) Sairyo K, Sakai T, Yasui N, Dezawa A: Conservative treatment for pediatric lumbar spondylolysis to achieve bone healing using a hard brace: what type and how long?: clinical article. J Neurosurg Spine 16: 610–614, 2012
- 22) Sakai T, Sairyo K, Takao S, Nishitani H, Yasui N: Incidence of lumbar spondylolysis in the general population in Japan based on multidetector computed tomography scans from two thousand subjects. Spine (Phila Pa 1976) 34: 2346–2350, 2009
- 23) Suh PB, Esses SI, Kostuik JP: Repair of pars interarticularis defect. The prognostic value of pars infiltration. Spine (Phila Pa 1976) 16: S445–S448, 1991
- 24) Wu SS, Lee CH, Chen PQ: Operative repair of symptomatic spondylolysis following a positive response to diagnostic pars injection. J Spinal Disord 12: 10–16, 1999
- 25) Anderson K, Sarwark JF, Conway JJ, Logue ES, Schafer MF: Quantitative assessment with SPECT imaging of stress injuries of the pars interarticularis and response to bracing. J Pediatr Orthop 20: 28–33, 2000
- 26) Liu X, Wang L, Yuan S, Tian Y, Zheng Y, Li J: Multiple-level lumbar spondylolysis and spondylolisthesis. J Neurosurg Spine 22: 283–287, 2015