抄録
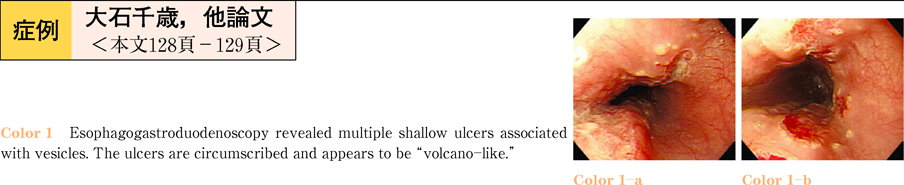
A 22-year-old man who had been suffering from ulcerative colitis (UC) was admitted to our hospital because of complains of fever and chest pain on swallowing in November in 2006. Because he was refractory to 5-aminosalycylates and corticosteroids, immunosuppressive therapy with 6-mericaptopurine (6-MP) was introduced 2 months prior to the presentation. At the time of presentation, he was malaise and had dysphagia. Laboratory tests showed mild anemia and inflammatory responses. Serological assays for viruses including herpes simplex, cytomegalo, varicella, and Epstein-Bar did not demonstrate primary infection. Esophagogastroduodenoscopy revealed multiple ulcers and vesicles with normal-appearing intervening mucosa. Histologic findings were infiltration of inflammatory cells in the epithelia and no specific information for diagnosis was noted. Although clinical evidence of viral infection was not confirmed, he was immunocompromised by 6-MP and endoscopy findings were similar to those of herpes esophagitis. Thus, we administered acyclovir for 7 days. Though oropharyngeal aphtha temporarily appeared, symptomatic and endoscopic resolutions were obtained thereafter. Because symptoms related to UC including bowel frequency, hematochezia and rectal urgency never changed throughout the above period, we concluded that the esophageal lesion was not a part of UC but superimposition of viral infection. Because esophageal involvement in UC is very rare and Crohn's disease affects upper gastrointestinal tract more preferably than UC, we have been following up him carefully.