ABSTRACT
Objective: We retrospectively investigated the preoperative and
postoperative sports and physical activities (SPA) of elderly patients with medial
compartment knee osteoarthritis who underwent opening-wedge high tibial osteotomy (OWHTO).
Methods: Fifty-six patients (62 knees) with medial compartment knee
osteoarthritis were included in the study. The patients comprised 45 women and 11 men with
a mean age at surgery of 71.6 years (range, 65–81 years). The mean follow-up period was
51±7 months. Patients who performed SPA to maintain their health for at least 30 min per
session more than once a week were defined as SPA cases. The preoperative and
postoperative ratios of SPA cases, the time to resuming or starting postoperative SPA, and
the frequency of performing postoperative SPA were investigated. Clinical results were
assessed using the Lysholm score. Results: Fifteen patients (26.7%) performed
SPA before OWHTO and 14 (25.0%) performed SPA after OWHTO (P=0.21). The mean time to
resuming or starting SPA after surgery was 14.1±10.0 months, and the frequency of
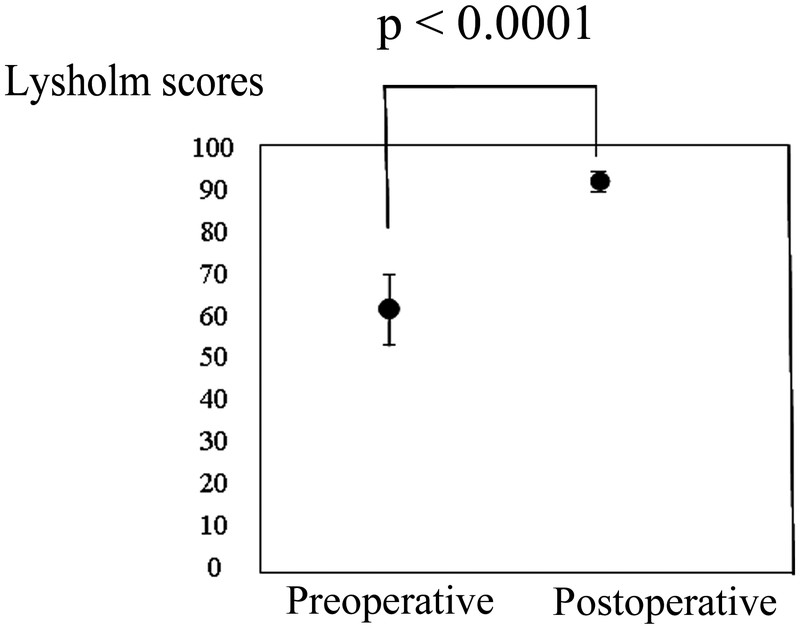
postoperative SPA sessions was 4.2±2.1 per week. The mean Lysholm score significantly
improved from 60.8±8.9 preoperatively to 92.5±2.5 postoperatively (P<0.0001).
Conclusion: The ratio of patients who performed SPA after OWHTO was still
<30% , and it took a comparatively long time for patients to resume or start SPA after
surgery.
INTRODUCTION
Knee osteoarthritis (OA) is a frequently disabling health condition in adults and is costly
in terms of healthcare resources. Opening-wedge high tibial osteotomy (OWHTO) is a surgical
procedure used to treat relatively early-stage medial compartment knee OA.1,2) By changing the axis of the lower limb using an
extra-articular approach, OWHTO preserves the native articular surface and decreases the
excess stress in the medial compartment of the knee.3,4,5)
After OWHTO, patients generally have no limits on their activities of daily living.
Excellent clinical results of OWHTO have been reported.1,2,3,4,5)
However, the activities performed by patients with knee OA before and after osteotomy have
rarely been described. The sports and physical activities (SPA) performed by patients with
knee OA before and after valgus knee osteotomy have been investigated and several reports
have been published.6,7,8) These studies involved patients with a wide range of ages
and included younger patients who resumed high-impact sports such as tennis and rugby
postoperatively.
Differences exist in the physical abilities and lifestyles of younger versus elderly
people. Elderly people experience a decline in mobility, which can cause sarcopenia and
frailty.9,10,11,12) Moreover, elderly patients with gait disorders such as knee
OA are thought to be at higher risk of lifestyle-related diseases and disuse syndrome.
Aerobic and muscle-strengthening exercises have been recommended for elderly people. Knee OA
and other conditions, however, may impede aerobic exercise. Improvement in the knee function
and the amelioration of pain of elderly patients with knee OA can create opportunities for
increased activities and therefore offer the potential to prevent various diseases
postoperatively. Many people in Japan retire at 65 years of age. Consequently, people aged
>65 years have adequate time to enjoy various health-promoting activities, including SPA.
SPA performed by elderly patients before and after OWHTO have not been reported. We
retrospectively investigated the preoperative and postoperative SPA of elderly patients aged
>65 years with medial compartment knee OA who underwent OWHTO. The excess stress in the
medial compartment of the knees and knee pain significantly would decrease after OWHTO. We
considered that the amount and variety of SPA performed by elderly patients might improve
postoperatively.
METHODS
Fifty-six patients (62 knees) with medial compartment knee OA were investigated. The
patients comprised 45 women and 11 men with a mean age at surgery of 71.6 years (range,
65–81 years). The mean follow-up period was 51±7 months. The correction angle was planned to
produce a lower-limb mechanical axis passing through approximately 70% of the width of the
tibial articular surface from its medial margin on anteroposterior full-length radiographs
of the lower limbs in the supine position. All surgical procedures were performed by the
method employed by Lobenhoffer and Agneskirchner.13) The superficial medial collateral ligament and pes
anserinus were dissected from the medial cortex of the tibia, and an osteotomy was
performed. Lower limb alignment was confirmed under an image intensifier during the
operation. Beta-tricalcium phosphate blocks were inserted into the osteotomy gap, and the
osteotomy site was fixed using a locking compression plate. The average preoperative and
postoperative lower limb alignments were evaluated by the femorotibial angle (FTA) and the
passing point of the lower-limb mechanical axis on the tibial plateau (%MA: the medial
margin of the tibial plateau is defined as 0% and the lateral margin is defined as 100%) on
anteroposterior full-length radiographs of the lower limbs while weight bearing.
Muscle strengthening exercises and range-of-motion exercises were started 1 day after
surgery. Partial weight bearing was permitted from 1 week after surgery, and full weight
bearing was permitted from 4 weeks after surgery. Partial weight bearing was, however, not
permitted until 3 weeks after surgery in patients with microfractures.14,15) SPA were generally permitted after the patients
were able to go smoothly up and down stairs without postoperative knee pain.
RESULTS
The preoperative FTA and %MA were 181.8°±6.3° and 18.6%±12.7%, respectively, whereas the
average postoperative FTA and %MA were 170.9°±3.2° and 64.0%±9.8%, respectively.
Fifteen patients (26.7%) performed SPA before OWHTO, whereas 14 (25.0%) performed SPA after
OWHTO. There was no significant difference between the preoperative and postoperative
numbers of patients performing SPA (P=0.21). The types of preoperative and postoperative SPA
are shown in Table 1. One patient participated
in three activities preoperatively and the other 14 patients participated in one activity.
Postoperatively, nine patients performed two or three activities. Three of the 15 patients
who performed SPA before OWHTO resumed the same type of SPA postoperatively. Two of the 15
patients quit performing SPA altogether; their preoperative SPA had been softball and
tennis, respectively. Two other patients changed the type of SPA postoperatively. The
remaining eight patients were able to perform other types of SPA postoperatively in addition
to their preoperative SPA. Three patients who did not perform SPA preoperatively started
performing SPA postoperatively. Overall, 11 (19.6%) patients were able to improve the amount
of SPA performed postoperatively. In the 14 patients performing SPA postoperatively, the
mean time to resuming or starting SPA after surgery was 14.1±10.0 months, and the frequency
of activities postoperatively was 4.2±2.1 per week. The mean Lysholm score significantly
improved from 60.8±8.9 preoperatively to 92.5±2.5 postoperatively (P<0.0001) (Fig. 1).
Table 1.
Preoperative and postoperative types of SPA (numbers of patients
participating)
| Before OWHTO* |
After OWHTO** |
| Walking (5) |
Walking (11) |
| Swimming (4) |
Swimming (9) |
| Golf (1) |
Golf (2) |
| Tai chi (1) |
Tai chi (1) |
| Japanese archery (1) |
Japanese archery (1) |
| Trekking (1) |
Trekking (2) |
| Cycling (1) |
Sports gym*** (1) |
| Table tennis (1) |
Social dancing (1) |
| Tennis (1) |
Gardening (1) |
| Softball (1) |
|
*One patient participated in three activities before OWHTO.
**Nine patients participated in two or three activities after OWHTO.
***The term "sports gym" refers to moderate exercise at a workout gym.
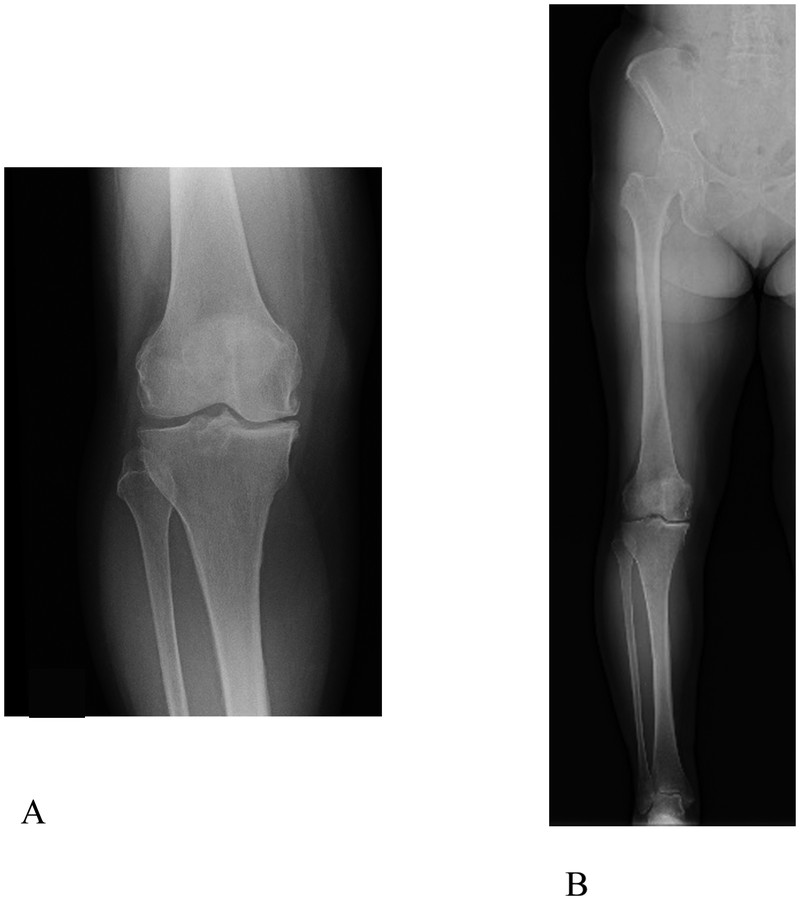
A 72-year-old woman developed right knee pain without a trigger and eventually had
difficulty walking. She was diagnosed with Kellgren–Lawrence grade III OA in her right
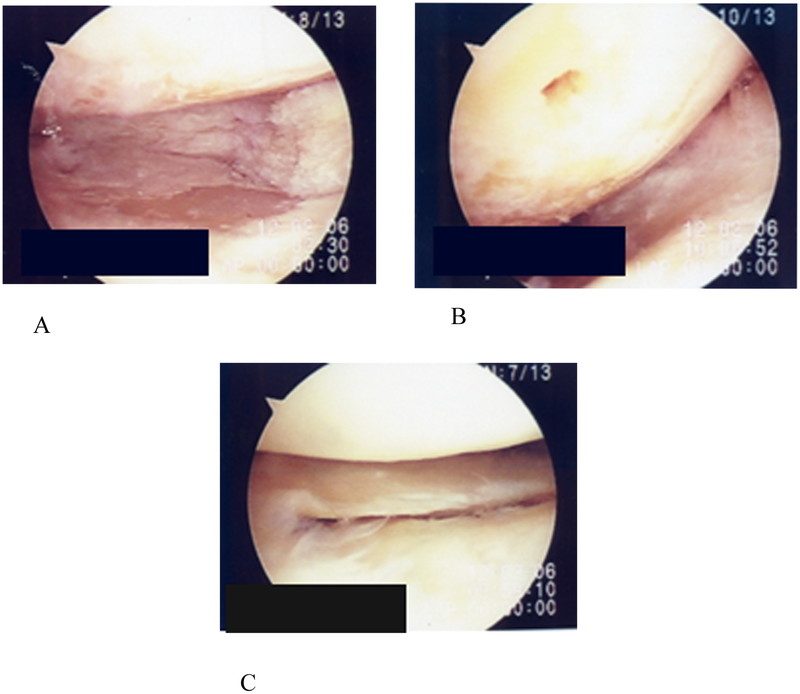
knee (Fig. 2). Arthroscopy before OWHTO revealed
cartilage wear on the medial femoral condyle and surface of the tibia on the opposite site
and exposure of subchondral bone (Fig. 3). OWHTO
was performed. The preoperative FTA and %MA were 180° and 24.3%, respectively, whereas the
postoperative FTA and %MA were 170° and 60.0%, respectively (Figs. 2 and 4). The
preoperative Lysholm score was 65 points and the 2-year postoperative Lysholm score had
improved to 89 points. Preoperatively, the patient enjoyed table tennis twice a week,
whereas she enjoyed ground golf (a recreational sport for elderly people similar to golf)
twice a week postoperatively.
DISCUSSION
In this study, we investigated the preoperative and postoperative SPA of elderly patients
aged >65 years with medial compartment knee OA who underwent OWHTO. In Japan, people
generally retire from work at the age of 65 years. Some people’s work involves heavy labor,
and not all people aged <65 years who perform heavy labor have a habit of also performing
SPA. Accurate evaluation of the postoperative improvements in the activities of patients
aged <65 years cannot be achieved by investigating SPA only: the types and quality of
labor also require consideration. Most patients in this study had retired from work;
additionally, none of the patients had performed heavy labor. Evaluation of changes in
activities other than SPA was not possible in our study. However, the patients who did not
regularly perform SPA in their daily life postoperatively likely experienced improvements in
activities such as stair climbing because of the improvements in their Lysholm scores.
Research on patients’ actual preoperative and postoperative lifestyles or physical abilities
is needed in a format other than a question-based study.
The lower limb alignment in our patients was considered to be sufficiently corrected after
OWHTO because our results were comparable with those of previous reports.5,16) Our hypothesis was that the amount of SPA performed by
elderly patients might improve after OWHTO. However, the improvement ratio of SPA was 19.6%
(<20%). The number of patients with medial compartment knee OA who performed SPA after
OWHTO was not significantly higher than that before surgery in this study. Thirteen patients
continued SPA preoperatively and postoperatively in some way, and some of these patients
performed two or three activities postoperatively.
Faschingbauer et al.8) reported
that patients with an average age of 42 and the highest work intensity returned to work
19.1±9.1 weeks after OWHTO. In the present study, the average time until resuming or
starting SPA after surgery was more than 1 year. It took our patients a comparatively long
time to resume or start SPA postoperatively, although there were differences in the
work-related and non-work-related activities between our patients and those of Faschingbauer
et al. This long delay may have caused our patients’ difficulty in resuming or starting SPA
postoperatively. Advancing age during the rehabilitation period might influence whether
these elderly patients want to resume or start SPA. Patients might either have no
established aims or even forget their aims of OWHTO and rehabilitation. After OWHTO, two
patients in our study quit performing their preoperative SPA of softball and tennis. These
activities are high-demand sports that are difficult to resume after OWHTO. These two
patients did not perform other SPA postoperatively. Postoperative residual pain and loss of
muscle strength might be a larger burden to these patients than previously
considered.6) Takeuchi et
al.17) reported that early
weight-bearing exercises enabled full weight bearing at 2 weeks after OWHTO. Accelerating
the start of walking postoperatively could help to maintain patients’ motivation for
rehabilitation and resuming SPA. However, detailed studies of treatment after OWHTO for
elderly patients are needed from viewpoints other than orthopedic surgery.
The duration and frequency of SPA when performed for health improvement should be either
more than 20 min per session more than three times a week or more than 30 min intermittently
almost every day.18,19) The exercise intensity should be
minimal in consideration of each patient’s exercise capability at the beginning. The
exercise regimen should be designed for the long term, preventing patients from growing
tired of performing SPA. Additionally, rehabilitation programs for elderly patients should
be based on the physiological and psychological changes associated with aging. However,
application of these recommendations to elderly patients performing SPA might be difficult
because many of them have various chronic diseases in addition to the above-mentioned
changes. Instead, elderly patients could be advised to perform SPA based on their subjective
complaints, including pain, respiratory discomfort, and palpitation. An established protocol
for smoother performance of SPA after OWHTO is needed.
CONCLUSION
The proportion of elderly patients with medial compartment knee OA who performed SPA after
OWHTO was still <30%, which was unchanged from the preoperative value. Moreover, it took
a relatively long time for patients to resume or start SPA after surgery.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
- 1. Koshino T, Murase T, Saito T: Medial
opening-wedge high tibial osteotomy with use of porous hydroxyapatite to treat medial
compartment osteoarthritis of the knee. J Bone Joint Surg Am
2003;85:78–85.
- 2. Dowd GS, Somayaji HS, Uthukuri M: High tibial
osteotomy for medial compartment osteoarthritis. Knee 2006;13:87–92.
- 3. Nha KW, Lee YS, Hwang DH, Kwon JH, Chae DJ, Park
YJ, Kim JI: Second-look arthroscopic findings after open-wedge high tibia osteotomy
focusing on the posterior root tears of the medial meniscus. Arthroscopy
2013;29:226–231.
- 4. Fujisawa Y, Masuhara K, Shiomi S: The effect of
high tibial osteotomy on osteoarthritis of the knee. Arthroscopic study of 54 knee joints.
Orthop Clin North Am 1979;10:585–608.
- 5. Akamatsu Y, Mitugi N, Mochida Y, Taki N,
Kobayashi H, Takeuchi R, Saito T: Navigated opening wedge high tibial osteotomy improves
intraoperative correction angle compared with conventional method. Knee Surg Sports
Traumatol Arthrosc 2012;20:586–593.
- 6. Salzmann GM, Ahrens P, Naal FD, El-Azab H, Spang
JT, Imhoff AB, Lorenz S: Sporting activity after high tibial osteotomy for the treatment
of medial compartment knee osteoarthritis. Am J Sports Med
2009;37:312–318.
- 7. Saragaglia D, Rouchy RC, Krayan A, Refaie R:
Return to sports after valgus osteotomy of the knee joint in patients with medial
unicompartmental osteoarthritis. Int Orthop 2014;38:2109–2114.
- 8. Faschingbauer M, Nelitz M, Uraub S, Reichel H,
Dornacher D: Return to work and sporting activities after high tibial osteotomy. Int
Orthop 2015;39:1527–1534.
- 9. Martinez BP, Batista AK, Ramos IR, Dantas JC,
Gomes IB, Júnior LA, Camalier Camalier Camelier FRCamelier AA. J Bras Pneumol
2016;42:196–202.
- 10. El Maghraoui A, Ebo’o FB, Sadni S, Majjad A,
Hamza T, Mounach A: Is there a relation between pre-sarcopenia, cachexia and osteoporosis
in patients with ankylosing spondylitis? BMC Musculoskelet Disord
2016;17:268.
- 11. Rozzini R: Aging clinical problems: a difficult
balance between age and frailty. Monaldi Arch Chest Dis 2015;84:727.
- 12. Berglund H, Hasson H, Wilhelmson K, Dunér A,
Dahlin-lvanoff S: The impact of socioeconomic conditions, social networks, and health on
frail older people’s life satisfaction: a cross-sectional study. Health Psychol Rev
2016;4:26–31.
- 13. Lobenhoffer P, Agneskirchner JD: Improvements in
surgical technique of valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc
2003;11:132–138.
- 14. Matsunaga D, Akizuki S, Takizawa T, Yamazaki I,
Kuraishi J: Repair of articular cartilage and clinical outcome after osteotomy with
microfracture or abrasion arthroplasty for medial gonarthrosis. Knee
2007;14:465–471.
- 15. Schuster P, Schultz M, Mayer P, Schlumberger M,
Immendoerfer M, Richter J: Open-wedge high tibial osteotomy and combined
abrasion/microfracture in severe medial osteoarthritis and varus malalignment: 5-year
results and arthroscopic findings after 2 years. Arthroscopy
2015;31:1279–1288.
- 16. Bito H, Takeuchi R, Kumagai K, Aratake M, Saito
I, Hayashi R, Sasaki Y, Aota Y, Saito T: A predictive factor for acquiring an ideal lower
limb realignment after opening-wedge high tibial osteotomy. Knee Surg Sports Traumatol
Arthrosc 2009;17:382–389.
- 17. Takeuchi R, Ishikawa H, Aratake M, Bito H, Saito
I, Kumagai K, Akamatsu Y, Saito T: Medial opening wedge high tibial osteotomy with early
full weight bearing. Arthroscopy 2009;25:46–53.
- 18. Yamamoto S, Yamasaki H: The recent exercise
prescription. The Bulletin of Keio University Sports Medical Center 1999:33–39 In
Japanese.
- 19. Koguma Y, Yamasaki H: The way of medical check. J
Clin Sports Med 1999;16:653–658 In Japanese.