ABSTRACT
Objective: We set out to examine the effectiveness of early rehabilitation
for maintaining mobility status during hospitalization in elderly patients with heart
failure. Methods: Using the Japanese Diagnosis Procedure Combination
inpatient database, we retrospectively examined the eligibility of 527,440 consecutive
patients aged ≥60 years who were diagnosed with heart failure with New York Heart
Association class ≥ II at admission between July 2010 and March 2014. Of the 146,735
eligible subjects, 39,357 underwent early rehabilitation and 107,378 underwent non-early
rehabilitation. Early rehabilitation was defined as rehabilitation starting within 3 days
after admission. A multivariable logistic regression analysis and an instrumental variable
analysis were carried out to examine the association of early rehabilitation with changes
in mobility status during hospitalization. Results: The proportion of heart
failure patients with maintained or improved mobility status during hospitalization was
higher in the early rehabilitation group. Multivariable logistic regression analysis
revealed that the early rehabilitation group had a significantly higher proportion with
maintained or improved mobility status (odds ratio, 1.32; 95% confidence interval,
1.21–1.43; P<0.001). The instrumental variable analysis showed that early
rehabilitation was associated with an increased proportion of patients with maintained or
improved mobility status (risk difference, 0.8%; 95% confidence interval, 0.4%–1.1%;
P<0.001). Conclusions: The present study suggests that early
rehabilitation is associated with an increase in the proportion of patients with
maintained or improved mobility status compared with non-early rehabilitation in elderly
inpatients with heart failure.
INTRODUCTION
Heart failure (HF) patients are commonly frail, and HF is associated with adverse health
outcomes.1,2,3,4,5,6) Because there is no gold standard diagnosis for frailty,
frailty within the HF population1) was defined as patients meeting three of the following five
phenotypic criteria for compromised ability to address stressors7): unintentional weight loss, exhaustion, weakness,
low physical activity, and slow walking speed. Transitions between frailty states
(non-frail, pre-frail, and frail) are not irreversible,8,9) and interventions that prevent the inability to perform
essential activities, such as walking at home without assistance, constitute an important
therapeutic strategy.
Previous studies showed that immobilization of elderly patients during hospitalization
after a cardiac event led not only to multiple complications,10) but also to the development of
disability.11) Other
studies showed that the loss of muscle mass through immobilization was associated with
decreased functional ability within 2 days of hospitalization,12) and with higher risks of morbidity, higher
hospital readmission rates, and prolonged periods of physical therapy after
hospitalization.13)
Therefore, early ambulation within the first 3 days of hospitalization, along with careful
planning, a suitable workload, and monitoring, has been recommended to enable inpatients to
achieve appropriate levels of activity as outpatients.14,15)
Previous studies of cardiovascular rehabilitation have provided long-term evidence that
comprehensive programs reduced mortality,16) reduced HF-related hospital admissions,17) improved patient quality of
life,17) and improved
self-reported health status.18)
However, the short-term effectiveness of early rehabilitation on mobility status, such as
walking ability, in elderly inpatients with HF remains to be elucidated.
The purpose of the present retrospective cohort study was to examine, using a national
inpatient database in Japan, the association (with adjustment for multiple factors) of early
rehabilitation with changes in mobility status during hospitalization among elderly
patients.
METHODS
Data Source
The Japanese Diagnosis Procedure Combination database is a national acute-care inpatient
database. The database includes administrative claims data and some detailed clinical data
for approximately 7 million inpatients per year (representing approximately 50% of all
acute-care inpatients in Japan) in more than 1,000 participating hospitals. All 82
academic hospitals are obliged to participate in the database, whereas community hospitals
participate on a voluntary basis. For all patients, the main diagnosis, the comorbidities
present at admission, and the complications occurring during hospitalization are coded
using International Classification of Diseases and Related Health Problems 10th Revision
(ICD-10) codes and text data in Japanese. The database also includes each hospital’s
unique identifier and the following patient details: age; sex; medical procedures,
including types of surgery coded with original Japanese codes; daily records of drug
administration and devices used; New York Heart Association (NYHA) Functional
Classification at admission; activity of daily living scores (including mobility status)
at admission and discharge; and the discharge status. The discharge status has three
categories: discharged to home; discharged to somewhere other than home; and in-hospital
death. The database also includes the dates of the start and cessation of
rehabilitation.
In Japan, hospitals authorized as cardiac rehabilitation facilities must have one or more
full-time cardiologists and two or more well-experienced physiotherapists or nurses, in
addition to a dedicated training room. As of 2015, the number of hospitals providing
cardiac rehabilitation was 782 (51.9%) of 1506 facilities with departments of
cardiology.
For this study, we extracted data on the following complications associated with acute
heart failure occurring during hospitalization: renal failure19)(N19, N170, N178, N179, N180, N189);
pneumonia20)(I189);
sepsis21)(A419); and
stroke22)(I60, I61, I62,
I63, I64, I65, I67, I68, I69). We also extracted data on each patient’s pre-rehabilitation
treatments: catecholamine administration (dopamine, dobutamine, noradrenaline),
carperitide administration, and cardiac surgery (coronary artery bypass grafting,
valvuloplasty, and valve replacement). Use of the following procedures before starting
rehabilitation was also examined: invasive and noninvasive ventilation; intra-aortic
balloon pumping (IABP); percutaneous cardiopulmonary support (PCPS); and continuous
hemodiafiltration (CHDF).
Based on Quan’s algorithm,23) each ICD-10 comorbidity code was converted to the Charlson
Comorbidity Index (CCI). The CCI was divided into three categories: 2, 3–4, and ≥5. The
body mass index (BMI) was calculated and categorized as24) underweight (<18.5 kg/m2), normal
weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese
(≥30.0 kg/m2).
The hospital volume was defined as the average number of HF patients per year admitted to
each hospital, and was categorized into tertiles. Because of the anonymous nature of the
data, the requirement for informed consent was waived. The study was approved by the
Institutional Review Board of The University of Tokyo.
Patient Selection
We identified patients who were diagnosed with HF (ICD-10 codes I110, I500, I501, and
I509); were NYHA class II, III, or IV; and were discharged between July 2010 and March
2014. We excluded the following patients: (i) those aged less than 60 years; (ii) those
designated NYHA class I; (iii) those who underwent cardiac surgery; (iv) those who died
during hospitalization; (v) those who had missing outcome data; and (vi) those who did not
undergo rehabilitation during hospitalization.
Early Rehabilitation
We defined early rehabilitation as rehabilitation provided by physical therapists and
occupational therapists within 3 days after admission, in line with the definition in a
previous guidline.14)
Outcome Measures
The outcome was maintained or improved mobility status between admission and discharge
for each patient. Based on the Barthel Index, the level-surface mobility status was
evaluated using four scores: immobile (0); wheelchair independent (1); walking with the
help of one person (2); and independent, but patients may use an aid, such as a stick
(3).25) In the present
study, we calculated the difference in mobility scores between admission and discharge.
Patients were categorized into two groups: mobility maintained or improved (≥0) and
mobility unmaintained (<0).
Statistical Analysis
The χ2-test and Mann-Whitney U-test were used to compare categorical variables
and continuous variables, respectively, between the early and non-early rehabilitation
groups. The number needed to treat (NNT) was calculated to estimate the number of patients
who would need to be treated with early rehabilitation rather than non-early
rehabilitation for one additional patient to benefit. A multivariable binary logistic
regression analysis was carried out to analyze the relationship between early
rehabilitation and mobility status during hospitalization with adjustment for age, sex,
mobility status at admission, NYHA class, BMI, CCI, pre-rehabilitation cardiopulmonary
support (i.e., catecholamine administration, mechanical ventilation, IABP, and PCPS),
carperitide administration, receipt of CHDF, complications (pneumonia, renal failure,
sepsis, and stroke), and hospital volume.
Because the data derived from multiple hospitals were structured by two strata (hospitals
and patients), we accounted for clustering within hospitals using a generalized estimating
equation with an exchangeable working correlation matrix and a robust estimator
variance–covariance matrix.26,27) All statistical analyses were carried out using IBM SPSS
statistics, version 22.0 (IBM, Armonk, NY). Values of P<0.05 were considered
significant.
Instrumental Variable (IV) Analysis
Conventional approaches, such as multivariable logistic regression analyses, cannot
adjust for hidden biases caused by unmeasured confounders. Consequently, we conducted an
IV analysis as a confirmatory investigation. The key assumptions of IV analysis
are28,29): (i) the IV is highly correlated
with the treatment, (ii) the IV is not correlated with any measured or unmeasured
variables among the patient characteristics, and (iii) the IV does not affect patient
outcomes except through the treatment.
The provision of early rehabilitation to HF patients may depend on the attending
physicians’ attitudes toward rehabilitation and the availability of cardiovascular
rehabilitation staff at an individual hospital. If a given hospital tends to conduct early
rehabilitation independently of patient characteristics, early rehabilitation will be
determined more strongly by the hospital in which the patient is treated than by the
patient’s particular risk factors. Under such conditions, the proportion of patients
receiving early rehabilitation provision per hospital can act as an IV, thereby permitting
a “natural experiment” for an unbiased estimate of the outcome even in the presence of
unmeasured confounders.28,29) IV analysis assumes that a patient’s choice of hospital is
made independently of the hospital’s orientation toward early rehabilitation, and that a
hospital’s conduct of early rehabilitation is independent of the outcome. A consistent
result from an IV analysis can serve as a useful confirmation of a conventional
analysis.
In the IV analysis, we included only patients admitted to hospitals treating at least 20
eligible HF patients during the study period. The continuous variable of the IV analysis
(the proportion of patients receiving early rehabilitation provision per hospital) was
dichotomized using the cut-off value of the 75th percentile of the proportions among the
eligible patients. A two-stage least-squares method was used to estimate the risk
difference in maintained or improved mobility status and its 95% confidence interval
between the early and non-early rehabilitation groups with adjustment for measured and
unmeasured variables. For this step, we used the ivreg2 procedure in
Stata version 12 (StataCorp, College Station, TX). To confirm that the proportion of
patients receiving early rehabilitation provision per hospital was not a weak IV, we used
a partial F-test.30) The null hypothesis was that there was no association
between the IV and the outcome. An F-statistic of >10 was considered to suggest that
the IV was not weak.30)
RESULTS
We identified a total of 527,440 patients who were diagnosed with HF at admission in 1,279
hospitals during the study period. We selected 146,735 eligible patients including 39,357
(26.8%) who underwent early rehabilitation and 107,378 (73.2%) who underwent non-early
rehabilitation (Fig. 1). The mean (standard
deviation: SD) age was 82.0 (8.6) years. The mean (SD) interval from admission to starting
rehabilitation and the length of hospital stay were 9.1 (11.8) days and 31.8 (30.0) days,
respectively. The period between admission and the start of rehabilitation was shorter in
the early rehabilitation group than in the non-early rehabilitation group [2.3 (0.6) vs.
11.5 (12.9) days]. The early rehabilitation group also had a shorter length of stay than the
non-early rehabilitation group [24.3 (21.8) vs. 34.4 (31.6) days].
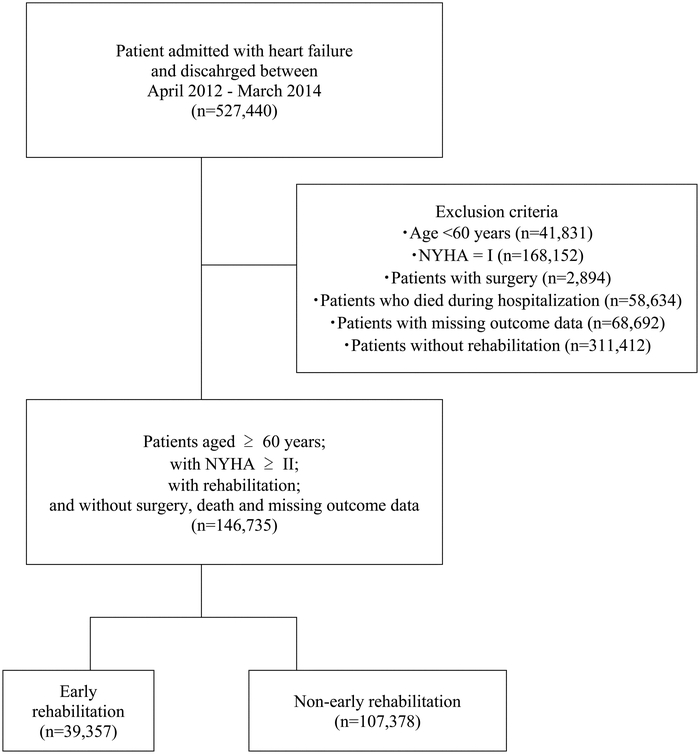
Table 1 shows the patient characteristics for
the early and non-early rehabilitation groups. The patients in the early rehabilitation
group were significantly more likely to be older, and to have a lower NYHA class, lower BMI,
and lower CCI scores. Patients in the early rehabilitation group were significantly less
likely require cardiopulmonary support, to be administered carperitide, to undergo CHDF, or
to have complications. Moreover, high-volume hospitals were more likely to conduct early
rehabilitation.
Table 1.
Patient characteristics and mobility status in the early and non-early
rehabilitation groups
|
|
All patients
(n =146,735) |
Early rehabilitation
(n
=39,357) |
Non-early
rehabilitation
(n =107,378) |
P |
| Age category (years), n (%) |
<0.001 |
|
60–69 |
14,630 |
(10.0) |
3,641 |
(9.3) |
10,989 |
(10.2) |
|
|
70–79 |
35,906 |
(24.5) |
9,269 |
(23.6) |
26,637 |
(24.8) |
|
|
80–89 |
68,754 |
(46.9) |
18,224 |
(46.3) |
50,530 |
(47.1) |
|
|
≥90 |
27,445 |
(18.7) |
8,223 |
(20.9) |
19,222 |
(17.9) |
|
| Sex, n (%) |
0.064 |
|
Male |
67,019 |
(45.7) |
17,819 |
(45.3) |
49,200 |
(45.8) |
|
|
Female |
79,716 |
(54.3) |
21,538 |
(54.7) |
58,178 |
(54.2) |
|
| NYHA class at admission, n (%) |
<0.001 |
|
II |
43,410 |
(29.6) |
13,194 |
(33.5) |
30,216 |
(28.1) |
|
|
III |
56,020 |
(38.2) |
14,869 |
(37.8) |
41,151 |
(38.3) |
|
|
IV |
47,305 |
(32.2) |
11,294 |
(28.7) |
36,011 |
(33.5) |
|
| Body mass index (kg/m2), n
(%) |
<0.001 |
|
18.5–22.9 |
58,339 |
(39.8) |
15,953 |
(40.5) |
42,386 |
(39.5) |
|
|
<18.5 |
21,809 |
(14.9) |
6,061 |
(15.4) |
15,748 |
(14.7) |
|
|
23.0–24.9 |
20,447 |
(13.9) |
5,666 |
(14.4) |
14,781 |
(13.8) |
|
|
25.0–29.9 |
21,930 |
(14.9) |
5,729 |
(14.6) |
16,201 |
(15.1) |
|
|
≥30 |
5,829 |
(4.0) |
1,502 |
(3.8) |
4,327 |
(4.0) |
|
|
missing |
18,381 |
(12.5) |
4,446 |
(11.3) |
13,935 |
(13.0) |
|
| Charlson Comorbidity Index |
<0.001 |
|
2 |
92,267 |
(62.9) |
25,461 |
(64.7) |
66,806 |
(62.2) |
|
|
3–4 |
49,310 |
(33.6) |
12,617 |
(32.1) |
36,693 |
(34.2) |
|
|
≥5 |
5,142 |
(3.5) |
1,273 |
(3.2) |
3,869 |
(3.6) |
|
|
missing |
16 |
(0.0) |
6 |
(0.0) |
10 |
(0.0) |
|
| Pre-rehabilitation treatment, n (%) |
|
| Receipt of cardiopulmonary support |
41,368 |
(28.2) |
8,020 |
(20.4) |
33,348 |
(31.1) |
<0.001 |
|
Use of catecholamine |
25,825 |
(17.6) |
4,001 |
(10.2) |
21,824 |
(20.3) |
<0.001 |
|
Receipt of ventilation |
24,219 |
(16.5) |
5,114 |
(13.0) |
19,105 |
(17.8) |
<0.001 |
|
Receipt of IABP |
9,490 |
(6.5) |
63 |
(0.2) |
9,427 |
(8.8) |
<0.001 |
|
Receipt of PCPS |
67 |
(0.0) |
1 |
(0.0) |
66 |
(0.1) |
<0.001 |
|
Use of carperitide |
61,579 |
(42.0) |
14,346 |
(36.5) |
47,233 |
(44.0) |
<0.001 |
|
Receipt of CHDF |
1,161 |
(0.8) |
77 |
(0.2) |
1,084 |
(1.0) |
<0.001 |
| Complications, n (%) |
|
|
Pneumonia |
5,898 |
(4.0) |
1,176 |
(3.0) |
4,722 |
(4.4) |
<0.001 |
|
Renal failure |
640 |
(0.4) |
202 |
(0.5) |
438 |
(0.4) |
0.007 |
|
Sepsis |
790 |
(0.5) |
141 |
(0.4) |
649 |
(0.6) |
<0.001 |
|
Stroke |
2,073 |
(1.4) |
386 |
(1.0) |
1,687 |
(1.6) |
<0.001 |
| Hospital volume (per year), n (%) |
<0.001 |
|
≤256 |
49,018 |
(33.4) |
12,259 |
(31.1) |
36,759 |
(34.2) |
|
|
257–454 |
47,360 |
(32.3) |
12,414 |
(31.5) |
34,946 |
(32.5) |
|
|
≥455 |
50,357 |
(34.3) |
14,684 |
(37.3) |
35,673 |
(33.2) |
|
| Mobility status at admission, n (%) |
<0.001 |
|
3 |
41,121 |
(28.0) |
11,584 |
(29.4) |
29,537 |
(27.5) |
|
|
2 |
21,971 |
(15.0) |
5,961 |
(15.1) |
16,010 |
(14.9) |
|
|
1 |
13,927 |
(9.5) |
3,503 |
(8.9) |
10,424 |
(9.7) |
|
|
0 |
69,716 |
(47.5) |
18,309 |
(46.5) |
51,407 |
(47.9) |
|
| Mobility status at discharge, n (%) |
<0.001 |
|
3 |
74,000 |
(50.4) |
20,845 |
(53.0) |
53,155 |
(49.5) |
|
|
2 |
30,796 |
(21.0) |
7,723 |
(19.6) |
23,073 |
(21.5) |
|
|
1 |
12,635 |
(8.6) |
3,107 |
(7.9) |
9,528 |
(8.9) |
|
|
0 |
29,304 |
(20.0) |
7,682 |
(19.5) |
21,622 |
(20.1) |
|
IABP, intra-aortic balloon pumping; PCPS, percutaneous cardiopulmonary support; CHDF,
continuous hemodiafiltration.
Mobility refers to indoors mobility about the house or ward and may include the use of
an aid. If using a wheelchair, patients must be able to negotiate corners/doors unaided.
Mobility 3 denotes independent (but patients may use any aid, e.g., a stick); mobility 2
denotes the ability to walk with the help of one person (verbal or physical support);
mobility 1 denotes wheelchair independent, including the ability to negotiate corners,
etc.; and mobility 0 denotes immobile.
The proportion of patients with immobility decreased from 47.5% at admission to 20.0% at
discharge. As shown in Table 2, the crude
proportion of patients with maintained or improved mobility status was significantly higher
in the early rehabilitation group than in the non-early rehabilitation group (94.7% vs.
93.3%; P<0.001) and the NNT was 71.4 (95% confidence interval, 61.1–93.0).
Table 2.
The crude proportion of patients with maintained and improved mobility status in
the early and non-early rehabilitation groups
|
All patients (n=146,735) |
Early rehabilitation (n=39,357) |
Non-early
rehabilitation (n=107,378) |
P |
Number needed to treat |
95% confidence interval |
| Maintained or improved mobility status, n (%) |
137,494
(93.7) |
37,269
(94.7) |
100,225
(93.3) |
<0.001 |
71.4 |
61.1–93.0 |
| Unmaintained mobility status, n (%) |
9,241
(6.3) |
2,088
(5.3) |
7,153
(6.7) |
Table 3 shows the results of multivariable
binary logistic regression analysis for changes in mobility status during hospitalization.
Compared with the non-early rehabilitation group, the early rehabilitation group was
significantly more likely to have maintained or improved mobility status (odds ratio, 1.32;
95% confidence interval, 1.21–1.43, P<0.001). The following factors were significantly
associated with a lower probability of maintained or improved mobility status: higher age,
being female, being NYHA class III or IV, having higher CCI, receipt of CHDF, and
complications of pneumonia, sepsis, and stroke. Receipt of carperitide and the complication
of renal failure were associated with a higher probability of maintained or improved
mobility status.
Table 3.
Multivariable logistic regression analysis for maintained or improved mobility
status at discharge in patients with acute heart failure
|
|
Odds ratio |
95% confidence interval |
P |
| Rehabilitation |
|
Non-early rehabilitation |
Reference |
|
|
|
|
|
Early rehabilitation |
1.32 |
1.21 |
– |
1.43 |
<0.001 |
| Age (years) |
|
60–69 |
Reference |
|
|
|
|
|
70–79 |
0.56 |
0.50 |
– |
0.63 |
<0.001 |
|
80–89 |
0.33 |
0.29 |
– |
0.37 |
<0.001 |
|
≥90 |
0.21 |
0.18 |
– |
0.24 |
<0.001 |
| Sex |
|
Male |
Reference |
|
|
|
|
|
Female |
0.84 |
0.80 |
– |
0.88 |
<0.001 |
| NYHA class at admission |
|
II |
Reference |
|
|
|
|
|
III |
0.80 |
0.76 |
– |
0.86 |
<0.001 |
|
IV |
0.83 |
0.77 |
– |
0.91 |
0.457 |
| Body mass index (kg/m2) |
|
18.5–22.9 |
Reference |
|
|
|
|
|
<18.5 |
0.88 |
0.83 |
– |
0.94 |
<0.001 |
|
23.0–24.9 |
1.08 |
1.01 |
– |
1.16 |
0.028 |
|
25.0–29.9 |
1.16 |
1.08 |
– |
1.24 |
<0.001 |
|
≥30 |
1.06 |
0.94 |
– |
1.21 |
0.339 |
|
missing |
0.98 |
0.90 |
– |
1.06 |
0.620 |
| Charlson Comorbidity Index |
|
2 |
Reference |
|
|
|
|
|
3–4 |
0.78 |
0.61 |
– |
1.00 |
<0.001 |
|
≥5 |
0.58 |
0.52 |
– |
0.65 |
<0.001 |
| Pre-rehabilitation treatment |
|
Receipt of cardiopulmonary support |
0.95 |
0.88 |
– |
1.01 |
0.092 |
|
Use of carperitide |
1.08 |
1.01 |
– |
1.16 |
0.029 |
|
Receipt of CHDF |
0.78 |
0.61 |
– |
1.00 |
0.046 |
| Complications |
|
Pneumonia |
0.63 |
0.57 |
– |
0.70 |
<0.001 |
|
Renal failure |
1.57 |
1.06 |
– |
2.31 |
0.024 |
|
Sepsis |
0.56 |
0.44 |
– |
0.72 |
0.001 |
|
Stroke |
0.45 |
0.42 |
– |
0.58 |
<0.001 |
| Hospital volume (per year) |
|
≤256 |
Reference |
|
|
|
|
|
257–454 |
1.08 |
0.96 |
– |
1.22 |
0.214 |
|
≥455 |
1.07 |
0.94 |
– |
1.23 |
0.272 |
In the IV analysis, we included 146,263 patients admitted to 1,142 hospitals that treated
at least 20 eligible HF patients during the study period. The continuous IV variable (the
proportion of patients receiving early rehabilitation provision per hospital) was
dichotomized by the cut-off value of 27.0%, which was the 75th percentile of the
proportions. The F-statistic showed that the proportion of patients
receiving early rehabilitation was a strong IV (F=46.8; P<0.01). In the
IV analysis, early rehabilitation was associated with an increased proportion of maintained
or improved mobility status (risk difference, 0.8%; 95% confidence interval, 0.4%–1.1%;
P<0.001).
DISCUSSION
In the present study, we used a large nationwide acute-care inpatient database to examine
the association of early rehabilitation with changes in mobility status during
hospitalization in HF patients with NYHA class II, III, or IV. The results showed that early
rehabilitation intervention within 3 days after admission was associated with a higher
proportion of HF patients with maintained or improved mobility status.
The association between early rehabilitation and mobility status is likely related with the
symptom of frailty. Generally, frailty develops in older people; consequently we excluded
patients aged less than 60 years.
Cardiac rehabilitation is generally divided into three phases: inpatient program (phase I),
outpatient program (phase II), and maintenance (phase III). In phase I, physical
rehabilitation aims to minimize the influence of inactivity and maintain or improve muscle
strength and mobility. However, to the best of our knowledge, no previous studies have
analyzed the effectiveness of early rehabilitation for elderly inpatients with HF at
improving or maintaining mobility during phase I. It is noteworthy that a previous study
found that the length of hospital stay in patients with HF in Japan was longer than those in
other countries.31) The reason
for this was the difference in clinical practice patterns between Japan and western
countries. This may limit the generalizability of the findings, however, the management of
maintaining mobility status remains important considering activity of daily living after
discharge.
Maintaining mobility status is also important for preventing frailty. Frailty is generally
defined as a multidimensional syndrome arising from the interplay of genetic, biological,
physical, psychological, social, and environmental factors.32) Therefore, a comprehensive rehabilitation program
including patient education, psychological intervention, and nutrition management is
recommended to prevent frailty. Previous studies showed that frailty was associated with
reduced lower-limb muscle strength,33) and that muscle weakness with muscle wasting was a frequent
comorbidity among patients with HF.34) Consequently, early physical exercise training may represent
a core component of inpatient rehabilitation to prevent physical inactivity, muscle
weakness, and reduced muscle strength.
Previous studies have reported the effects of physical exercise in patients with heart
disease in terms of muscle fibers and the mitochondrial apparatus,35,36,37) the neuroendocrine system,38) cardiac function through anti-remodeling
effects,36) and improvement
of heart perfusion.39) In the
present study, the details of the rehabilitation programs were not determined, and the
mechanism for the effectiveness of early rehabilitation on maintaining mobility remains
unclear. However, we speculate that interventions such as early rehabilitation could play an
important role in preventing the progression of disability.
The present study has several limitations. First, the database does not include detailed
information about the severity of cardiac dysfunction (e.g., the left ventricular ejection
fraction or underlying diseases). Second, the database includes information relating to the
period of hospitalization only. Consequently, we were unable to analyze pre-hospital and
post-discharge outcomes, including long-term mobility. Third, mobility status may be
affected not only by the level of performance, but also by risk management to prevent falls.
Fourth, in the present study, we used mobility status as the outcome, but the validity and
reliability of recorded data on the outcome have not been evaluated. Moreover, approximately
15% of the outcome data were missing, and the distribution of the missing data might not
have been random.
CONCLUSIONS
Although the changes in mobility status were multifactorial, the present retrospective
study using a national inpatient database showed that early rehabilitation was independently
associated with a reduction in unmaintained mobility status in elderly HF patients with NYHA
class II, III, or IV.
ACKNOWLEDGEMENTS
This study was funded by grants from the Ministry of Health, Labour and Welfare, Japan and
The Japan Agency for Medical Research and Development.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
- 1. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch
C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA, Cardiovascular Health
Study Collaborative Research Group: Frailty in older adults: evidence for a phenotype. J
Gerontol A Biol Sci Med Sci 2001;56:M146–M157. PMID:11253156,
DOI:10.1093/gerona/56.3.M146
- 2. Rockwood K, Howlett SE, MacKnight C, Beattie BL,
Bergman H, Hébert R, Hogan DB, Wolfson C, McDowell I: Prevalence, attributes, and outcomes
of fitness and frailty in community-dwelling older adults: report from the Canadian study
of health and aging. J Gerontol A Biol Sci Med Sci 2004;59:1310–1317. PMID:15699531,
DOI:10.1093/gerona/59.12.1310
- 3. Fugate Woods N, LaCroix AZ, Gray SL, Aragaki A,
Cochrane BB, Brunner RL, Masaki K, Murray A, Newman AB, Women’s Health Initiative:
Frailty: emergence and consequences in women aged 65 and older in the Women’s Health
Initiative Observational Study. J Am Geriatr Soc 2005;53:1321–1330. PMID:16078957,
DOI:10.1111/j.1532-5415.2005.53405.x
- 4. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood
K: Frailty in elderly people. Lancet 2013;381:752–762. PMID:23395245,
DOI:10.1016/S0140-6736(12)62167-9
- 5. Murad K, Kitzman DW: Frailty and multiple
comorbidities in the elderly patient with heart failure: implications for management.
Heart Fail Rev 2012;17:581–588. PMID:21626426,
DOI:10.1007/s10741-011-9258-y
- 6. Jha SR, Ha HS, Hickman LD, Hannu M, Davidson PM,
Macdonald PS, Newton PJ: Frailty in advanced heart failure: a systematic review. Heart
Fail Rev 2015;20:553–560. PMID:25982016, DOI:10.1007/s10741-015-9493-8
- 7. Xue QL: The frailty syndrome: definition and
natural history. Clin Geriatr Med 2011;27:1–15. PMID:21093718,
DOI:10.1016/j.cger.2010.08.009
- 8. Gill TM, Gahbauer EA, Allore HG, Han L:
Transitions between frailty states among community-living older persons. Arch Intern Med
2006;166:418–423. PMID:16505261, DOI:10.1001/archinte.166.4.418
- 9. Guralnik JM, Ferrucci L, Balfour JL, Volpato S,
Di Iorio A: Progressive versus catastrophic loss of the ability to walk: implications for
the prevention of mobility loss. J Am Geriatr Soc 2001;49:1463–1470. PMID:11890584,
DOI:10.1046/j.1532-5415.2001.4911238.x
- 10. Atkins JR, Kautz DD: ICU progressive mobility.
Nurs Crit Care 2015;10:19–21. DOI:10.1097/01.CCN.0000471006.01956.e1
- 11. Gill TM, Allore HG, Holford TR, Guo Z:
Hospitalization, restricted activity, and the development of disability among older
persons. JAMA 2004;292:2115–2124. PMID:15523072,
DOI:10.1001/jama.292.17.2115
- 12. Freeman R, Maley K: Mobilization of intensive
care cardiac surgery patients on mechanical circulatory support. Crit Care Nurs Q
2013;36:73–88. PMID:23221444, DOI:10.1097/CNQ.0b013e31827532c3
- 13. Adler J, Malone D: Early mobilization in the
intensive care unit: a systematic review. Cardiopulm Phys Ther J
2012;23:5–13.
- 14. American College of Sports Medicine (ACSM): ACSM’s
guidelines for exercise testing and prescription (9th ed). Philadelphia, PA: Lippincott
Williams and Wilkins; 2004.
- 15. Rion JH, Kautz DD: The walk to save: benefit of
inpatient cardiac rehabilitation. Medsurg Nurs 2016;25:159–162.
- 16. Piepoli MF, Davos C, Francis DP, Coats AJ,
ExTraMATCH Collaborative: Exercise training meta-analysis of trials in patients with
chronic heart failure (ExTraMATCH). BMJ 2004;328:189. PMID:14729656,
DOI:10.1136/bmj.328.7441.711-b
- 17. Davies EJ, Moxham T, Rees K, Singh S, Coats AJ,
Ebrahim S, Lough F, Taylor RS: Exercise based rehabilitation for heart failure. Cochrane
Database Syst Rev 2010;CD003331.
- 18. Flynn KE1, Piña IL, Whellan DJ, Lin L, Blumenthal
JA, Ellis SJ, Fine LJ, Howlett JG, Keteyian SJ, Kitzman DW, Kraus WE, Miller NH, Schulman
KA, Spertus JA, O’Connor CM, Weinfurt KP: Effects of exercise training on health status in
patients with chronic heart failure. HF-ACTION Randomized Controlled Trial. JAMA
2009;301:1451–1459.
- 19. Mullens W, Abrahams Z, Francis GS, Sokos G,
Taylor DO, Starling RC, Young JB, Tang WH: Importance of venous congestion for worsening
of renal function in advanced decompensated heart failure. J Am Coll Cardiol, 2009 17;
53(7): 589–596.
- 20. Musher DM, Rueda AM, Kaka AS, Mapara SM: The
association between pneumococcal pneumonia and acute cardiac events. Clin Infect Dis
2007;45:158–165. PMID:17578773, DOI:10.1086/518849
- 21. Merx MW, Weber C: Sepsis and the heart.
Circulation 2007;116:793–802. PMID:17698745,
DOI:10.1161/CIRCULATIONAHA.106.678359
- 22. Watson RD, Gibbs CR, Lip GY: ABC of heart
failure: Clinical features and complications. BMJ 2000;320:236–239. PMID:10642237,
DOI:10.1136/bmj.320.7229.236
- 23. Quan H, Sundararajan V, Halfon P, Fong A, Burnand
B, Luthi JC, Saunders LD, Beck CA, Feasby TE, Ghali WA: Coding algorithms for defining
comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care 2005;43:1130–1139.
PMID:16224307, DOI:10.1097/01.mlr.0000182534.19832.83
- 24. WHO: Obesity: preventing and managing the global
epidemic. In: Report of a WHO Consultation, WHO Technical Report Series 894. Geneva: World
Health Organization; 2000.
- 25. Collin C, Wade DT, Davies S, Horne V: The Barthel
ADL Index: a reliability study. Int Disabil Stud 1988;10:61–63. PMID:3403500,
DOI:10.3109/09638288809164103
- 26. Zeger SL, Liang KY: Longitudinal data analysis
for discrete and continuous outcomes. Biometrics 1986;42:121–130. PMID:3719049,
DOI:10.2307/2531248
- 27. Hubbard AE, Ahern J, Fleischer NL, Laan MV,
Lippman SA, Jewell N, Bruckner T, Satariano WA: To GEE or not to GEE. Epidemiology
2010;21:467–474. PMID:20220526, DOI:10.1097/EDE.0b013e3181caeb90
- 28. Newhouse JP, McClellan M: Econometrics in
outcomes research: the use of instrumental variables. Annu Rev Public Health
1998;19:17–34. PMID:9611610, DOI:10.1146/annurev.publhealth.19.1.17
- 29. Brookhart MA, Rassen JA, Schneeweiss S:
Instrumental variable methods in comparative safety and effectiveness research.
Pharmacoepidemiol Drug Saf 2010;19:537–554. PMID:20354968,
DOI:10.1002/pds.1908
- 30. Staiger D, Stock JH: Instrumental variables
regression with weak instruments. Econometrica 1997;65:557–586.
DOI:10.2307/2171753
- 31. Konishi M, Ishida J, Springer J, von Haehling S,
Akashi YJ, Shimokawa H, Anker SD: Heart failure epidemiology and novel treatments in
Japan: facts and numbers. ESC Heart Fail 2016;3:145–151. PMID:27840692,
DOI:10.1002/ehf2.12103
- 32. Walston J, Hadley EC, Ferrucci L, Guralnik JM,
Newman AB, Studenski SA, Ershler WB, Harris T, Fried LP: Research agenda for frailty in
older adults: toward a better understanding of physiology and etiology: summary from the
American Geriatrics Society/National Institute on Aging Research Conference on Frailty in
Older Adults. J Am Geriatr Soc 2006;54:991–1001. PMID:16776798,
DOI:10.1111/j.1532-5415.2006.00745.x
- 33. Batista FS, Gomes GA, Neri AL, Guariento ME,
Cintra FA, Sousa ML, D’Elboux MJ: Relationship between lower-limb muscle strength and
frailty among elderly people. Sao Paulo Med J 2012;130:102–108. PMID:22481756,
DOI:10.1590/S1516-31802012000200006
- 34. Fülster S, Tacke M, Sandek A, Ebner N, Tschöpe C,
Doehner W, Anker SD, von Haehling S: Muscle wasting in patients with chronic heart
failure: results from the studies investigating co-morbidities aggravating heart failure
(SICA-HF). Eur Heart J 2013;34:512–519. PMID:23178647,
DOI:10.1093/eurheartj/ehs381
- 35. Kavazis AN, Alvarez S, Talbert E, Lee Y, Powers
SK: Exercise training induces a cardioprotective phenotype and alterations in cardiac
subsarcolemmal and intermyofibrillar mitochondrial proteins. Am J Physiol Heart Circ
Physiol 2009;297:H144–H152. PMID:19429812,
DOI:10.1152/ajpheart.01278.2008
- 36. Campos JC, Queliconi BB, Dourado PM, Cunha TF,
Zambelli VO, Bechara LR, Kowaltowski AJ, Brum PC, Mochly-Rosen D, Ferreira JC: Exercise
training restores cardiac protein quality control in heart failure. PLoS One
2012;7:e52764. PMID:23300764, DOI:10.1371/journal.pone.0052764
- 37. Jiang HK, Wang YH, Sun L, He X, Zhao M, Feng ZH,
Yu XJ, Zang WJ: Aerobic interval training attenuates mitochondrial dysfunction in rats
post-myocardial infarction: roles of mitochondrial network dynamics. Int J Mol Sci
2014;15:5304–5322. PMID:24675698, DOI:10.3390/ijms15045304
- 38. Zucker IH, Xiao L, Haack KK: The central
renin–angiotensin system and sympathetic nerve activity in chronic heart failure. Clin Sci
2014;126:695–706. PMID:24490814, DOI:10.1042/CS20130294
- 39. Kendziorra K, Walther C, Foerster M,
Möbius-Winkler S, Conradi K, Schuler G, Sabri O, Hambrecht R, Kluge R: Changes in
myocardial perfusion due to physical exercise in patients with stable coronary artery
disease. Eur J Nucl Med Mol Imaging 2005;32:813–819. PMID:15776230,
DOI:10.1007/s00259-005-1768-1